
Abstract

Esophageal obstruction is a relatively rare event. Common predisposing factors include bulky esophageal carcinomas, achalasia, strictures, diffuse esophageal spasm, and many other conditions. Patients with glottic cancer requiring total laryngectomy have a small but finite rate of pharyngoesophageal obstruction, usually caused by narrow anastomotic segments. We present two cases of esophageal obstruction in postlaryngectomy patients caused not by anastomotic narrowing but by solidification of tube feedings in the distal esophagus during the early postoperative period.
CASE REPORTS
On postoperative day 7 the nasogastric tube was discontinued, and the patient underwent a Gastrografin (meglumine diatrizoate) swallow study. This showed good passage of dye past the site of anastomosis; however, difficult passage of dye was noted in the thoracic esophagus. It was believed that this represented edema caused by nasogastric tube irritation, and the patient began a clear-liquid diet. Approximately 6 hours after starting oral feeding, the patient was noted to have oral and nasal regurgitation of his liquid diet and a subjective sense of the food sticking in his esophagus.
The next day, when the patient continued to regurgitate liquids, a barium swallow was obtained. This test demonstrated a filling defect in the distal esophagus approximately 12 cm in length (Fig. 1). Circumferential barium coating suggested that this represented an intraluminal esophageal mass rather than an intramural mass. No barium was noted entering the stomach.
It was believed that this most likely represented retained food or enteral feedings, and on postoperative day 10 the patient underwent a diagnostic and therapeutic rigid esophagoscopy in the operative suite. The pharyngeal anastomosis was noted to be widely patent; however, thick blue concretions were found in the distal esophagus extending to the level of the gastroesophageal junction. These were meticulously removed with suctioning and forceps, and the esophagoscope was eventually passed into the stomach without further signs of obstruction. A postoperative chest x-ray film revealed no evidence of Gastrografin or barium in the cervical or thoracic esophagus.
The patient again began a clear-liquid diet, which he tolerated without regurgitation. His diet was advanced without difficulty, and he was discharged to home on postoperative day 12. He has had no subsequent feeding complications and remains disease free.
On postoperative day 12 the patient underwent diagnostic and therapeutic rigid esophagoscopy in the surgical suite. Blue concretions were noted in the midesophagus. These were easily removed with irrigation and suctioning. The esophagoscope was then easily passed into the stomach with no evidence of further obstruction.
After the procedure the patient began a liquid diet, which he tolerated well. His diet was advanced without difficulty, and he was discharged. He has had no further feeding difficulties and remains disease free.

Barium swallow revealing a filling defect in the distal esophagus with no evidence of barium entering the stomach.
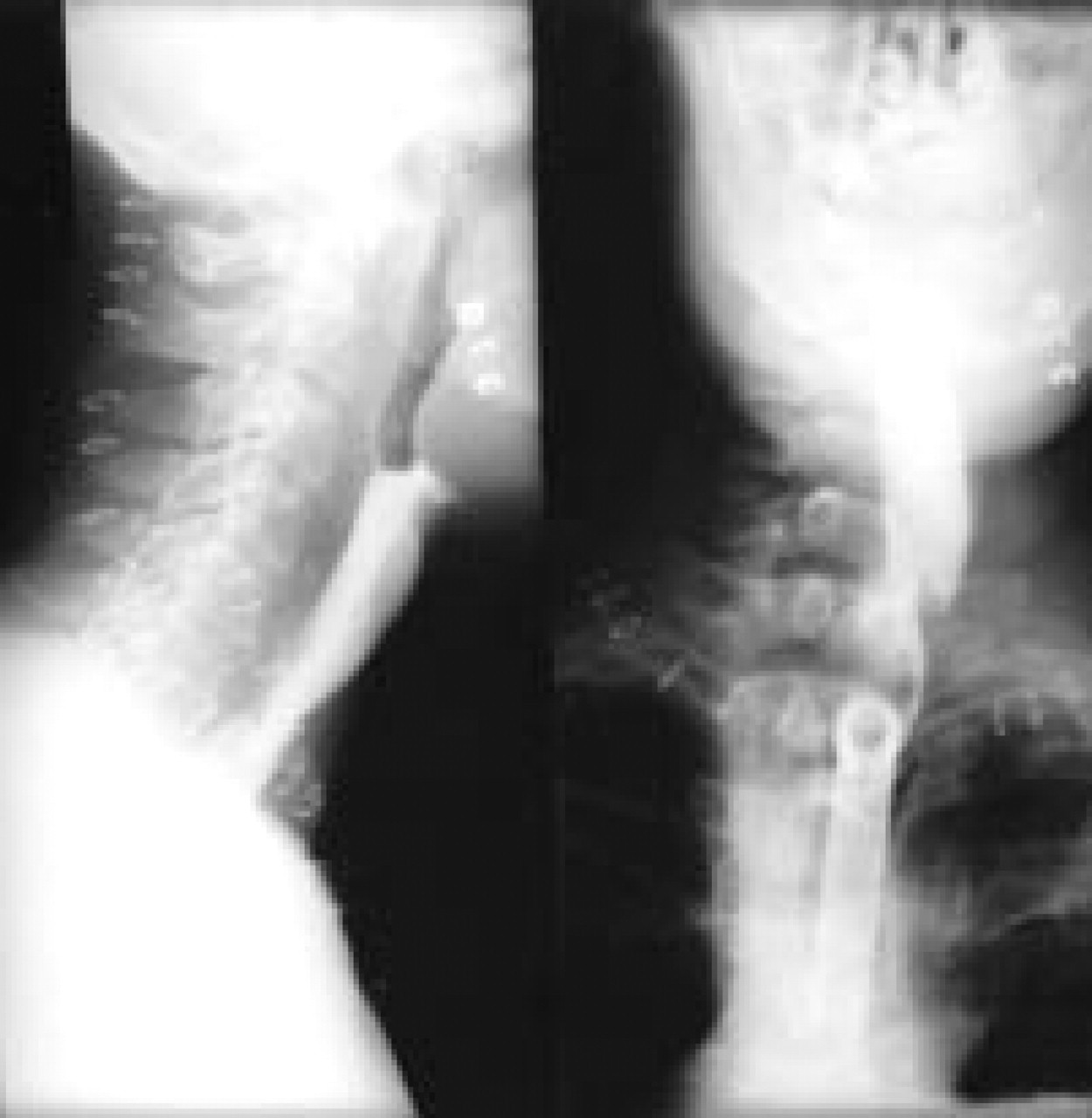
Gastrografin swallow 10 days after laryngectomy revealed a filling defect in the midesophagus with no evidence of dye entering the stomach.
DISCUSSION
Esophageal obstruction caused by tube feedings has rarely been reported in the literature. The earliest reported cases appear to be associated with the intake of Serutan (psyllium), a laxative, in the 1950s. 1 If given with insufficient amounts of water, Serutan was found to form concretions in the stomach and esophagus of patients, causing obstructive symptoms.
In the 1980s it was reported by several groups that sucralfate, when given alone or concurrently with tube feedings, could cause esophageal obstruction. 2 The precise role of sucralfate in the development of esophageal obstruction in these patients is under debate.
More recently, esophageal obstruction caused by disruption of orogastric tubes with subsequent tube-feeding concretions was reported. 3 In vitro experiments performed by that group suggest that solidification of tube feedings could not be explained only by stasis of liquid in the esophageal lumen. Rather they hypothesized that enteral feedings entered the esophagus through disruption of the orogastric tube and esophageal dysmotility, and the presence of a large-bore tube prevented the clearance of the solution from the esophagus. They further hypothesized that acid reflux from the stomach induced the precipitation of protein in the feeding formula, causing the formation of concretions.
We present two cases of tube-feeding concretions occurring in a patient after laryngectomy. These patients did not have orogastric tubes, nor did they receive concomitant sucralfate or antacids. The nasogastric tubes were properly placed, and no significant difficulties occurred either in advancing enteral feedings or with obstructive symptoms while the tubes were in place. Rather, signs and symptoms of obstruction occurred when the nasogastric tube was removed and the patients attempted to take oral feedings. We can only hypothesize that reflux of enteral feedings and gastric acid together into the esophageal lumen allowed the precipitation of protein and the subsequent formation of esophageal concretions around the tube. In addition, esophageal dysmotility may have played a role in the formation of these foreign bodies.
SUMMARY
We report two cases of tube-feeding concretions causing esophageal obstruction in patients after laryngectomy The cause of tube-feeding concretions is unknown at this time but probably involves esophageal stasis caused by esophageal dysmotility, protein precipitation by acidic gastric contents, tube damage, and concomitant use of sucralfate and other antacids. Although this is a rare complication of nasogastric feedings, the diagnosis should be entertained in cases in which postoperative esophageal obstruction is noted in head and neck surgical patients.