
Abstract

A 41-year-old nondiabetic woman, undergoing chemotherapy for acute myelocytic leukemia, went to her oncologist with a 3-day history of right-sided facial pain, right cheek swelling, and low-grade fever. The patient was severely neutropenic and thrombocytopenic because of chemotherapy. She was admitted to the hospital by the oncology service and given intravenous antibiotics.
Examination by the otolaryngology consult team revealed mild right cheek and periorbital swelling. The patient's visual acuity and extraocular motion were intact. She had no cranial nerve deficits. Intranasal endoscopy demonstrated a moderate-sized septal perforation with necrotic tissue along its border, and black/necrotic tissue had replaced the right middle turbinate (Fig 1).
Urgent CT of the paranasal sinuses revealed only pansinusitis with bony destruction of the right uncinate process and middle turbinate and a septal perforation. Amphotericin B therapy was initiated, and the patient was taken urgently to the operating room for debridement of a presumed mucormycosis infection. Frozen-section analysis of the involved tissue indicated an invasive fungal process. Endoscopic debridement of all nonviable tissue was undertaken. An open surgical approach (lateral rhinotomy) was avoided to minimize the chance of postoperative hemorrhage given her refractory thrombocytopenia.
Permanent histopathologic analysis of the excised tissue showed invasion by fungal elements. Fungal cultures subsequently confirmed a diagnosis of mucormycosis. A second-look endoscopic debridement was done 2 days later. Currently the patient has completed full antifungal therapy, and her intranasal examination shows no evidence of fungal disease 5 months after debridement.
DISCUSSION
Paranasal sinus mucormycosis (PSM) is an invasive, highly aggressive fungal infection that usually occurs in diabetic patients in the setting of ketoacidosis or in immunocompromised patients. Patients with PSM typically have fever (44%), nasal ulcerations/black necrotic tissue in the nose (38%), peri orbital or facial edema (34%), visual changes (30%), headache (25%), and facial pain (22%). 1 Typical findings of PSM on CT scan include mucoperiosteal edema of the sinuses associated with bony destruction. 2 Frank involvement of the orbit or brain can occur with mucormycosis. 3 The history and physical examination, including nasal endoscopy, are sufficient to make a presumptive clinical diagnosis. CT scan is useful for detecting sinus disease and bony erosion, whereas MRI is useful for evaluating the status of intracranial and intraorbital structures. Prompt surgical debridement of all clinically non-viable tissue is required. Frozen-section analysis should be obtained before definitive surgical debridement to confirm further the presence of an invasive fungal infection. Appropriate cultures and biopsy specimens for permanent histopathology are taken as well. Surgical debridement can be accomplished endoscopically, as in our case, provided that the involved tissue is limited to the paranasal sinuses and septum. Systemic antifungal therapy and management of hyperglycemia in diabetic patients are the other cornerstones of treatment. In addition, there are reports of improved survival with hyperbaric oxygen therapy as an adjunct to surgical debridement and antifungal therapy. 4
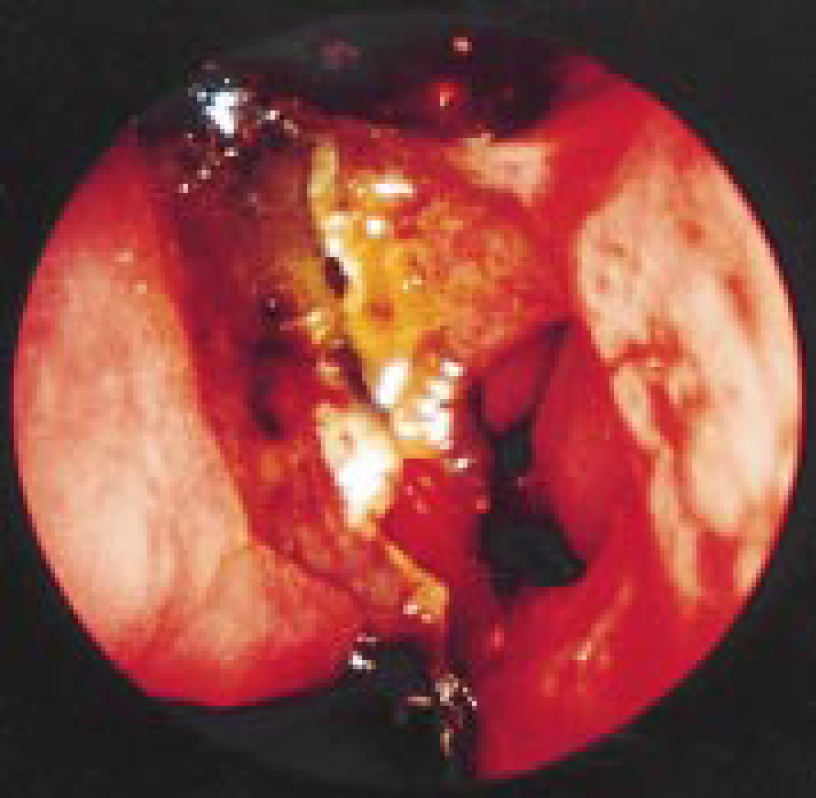
Intranasal view of mucormycosis. Note the septal perforation and necrosis of the right middle turbinate.