
Abstract
BACKGROUND: The aim of this prospective study was to evaluate the efficacy of a combined (local and systemic) steroid therapy on the extent of chronic polypoid rhinosinusitis and patient symptoms.
METHODS AND PATIENTS: Subjects of this study were 20 patients with severe chronic polypoid rhinosinusitis with total or subtotal narrowing of the all sinuses. A nasal budesonide spray (2 × 0.1 mg/day) and an oral fluocortolone medication with a daily reduction during a 12-day period (total dose: 560 mg = group 1) and a 20-day period (total dose: 715 mg = group 2), respectively, were administered. Before and after the steroid treatment we evaluated the extent of the sinusitis with MRI and patient symptoms with symptom-related questionnaires.
RESULTS: A significant reduction (>30%) of the chronic polypoid rhinosinusitis was observed in 50% of MRI findings. The steroid effect on polypoid masses was heterogeneous in different anatomic areas (maxillary sinus 40%, anterior ethmoid 19%, posterior ethmoid 33%, sphenoidal sinus 61%, frontal sinus 46%). Most sinusitis-related symptoms were distinctly diminished in most patients (80%). No major side effects were observed.
CONCLUSIONS: A combined short-term steroid therapy is highly effective in chronic polypoid rhinosinusitis, reducing the mucosal inflammation mainly in the large sinuses and reducing the incidence of symptoms significantly. However, this therapy was insufficient in the anterior ethmoid and cannot replace the current surgical treatment concept of the osteomeatal complex in CPR. The indication for such a short-term steroid therapy is the preoperative treatment. It facilitates functional endoscopic sinus surgery by reducing the extent of surgical procedures, the time, and thereby the risks of sinus surgery. (Otolaryngol Head Neck Surg 1999;120:517-23.)
The pathogenesis of nasal polyposis remains unclear to date. Therapeutic strategies are topics of ongoing discussion. The benefit of functional endoscopic sinus surgery (FESS) in chronic polypoid rhinosinusitis (CPR) is well documented in clinical series, 1,2 and some researchers advocate performing an endoscopic surgical treatment in all cases. 3,4 Other authors recommended medical treatment for routine use and suggest that surgical removal should be reserved for those cases in which the presence of residual or recurrent polyps justifies the inherent risks and discomfort for the patients. 5,6 However, the effect of medical treatment is generally recognized. The efficacy of topical corticosteroids in nasal polyposis has been confirmed by 13 placebo-controlled studies, 7–10 whereas investigations of systemic steroids in CPR have been insufficient. In a review of the literature, we retrieved only three series reporting on effects of systemic steroids in nasal polyposis. 5,6,11
The aim of this prospective study was to evaluate the influence of a combined (local and systemic) steroid therapy on the symptoms and extent of the disease in patients with CPR, to compare these data with those reported in the recent literature and to establish indications for a short-term steroid therapy in this disease.
METHODS AND PATIENTS
A prospective study was performed in the ENT Department of the University of Cologne in 1996. Subjects of this study were 20 patients with severe CPR seeking treatment for FESS. Informed consent was obtained for the study. Exclusion criteria were contraindications for systemic steroid therapy, previous sinus surgery, and acute bacterial sinusitis. At the first visit rhinologic examinations were performed, including a detailed medical history, allergy-screening tests (prick test, allergen-specific IgE levels), and nasal cytology.
The clinical symptoms were assessed on 0-10 visual analog scales (VASs), which considered reduction of general health, nasal obstruction, sense of smell, headache or facial pain, and nasal discharge or postnasal drip.
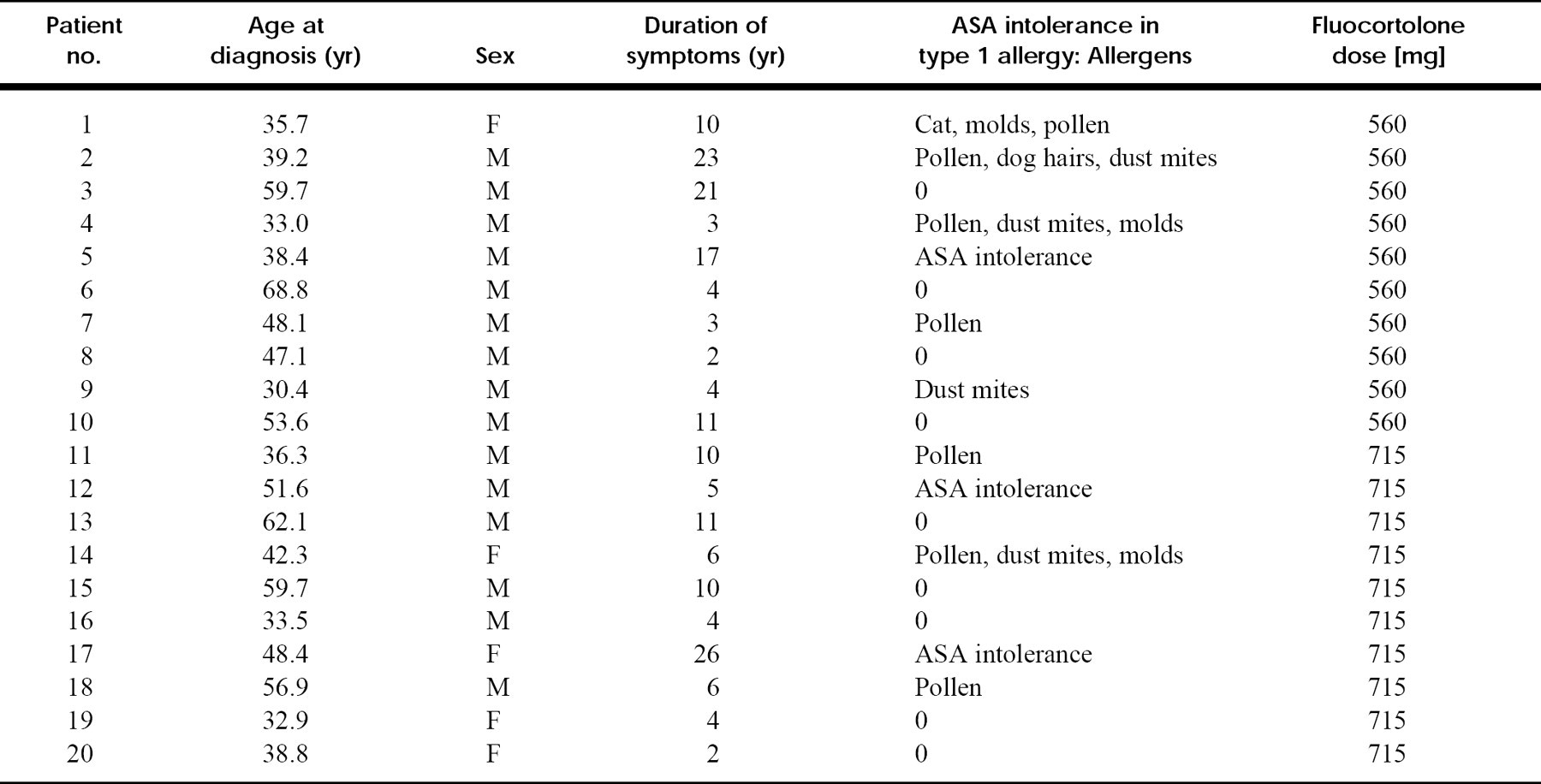
Coronal and transverse MRI of the no se and paranasal sinuses established the diagnosis. Clinical data of patients are condensed in Table 1.
Demographic data and clinical findings of patients
Sinusitis-related symptoms: Results of VASs before and after steroid treatment in all patients
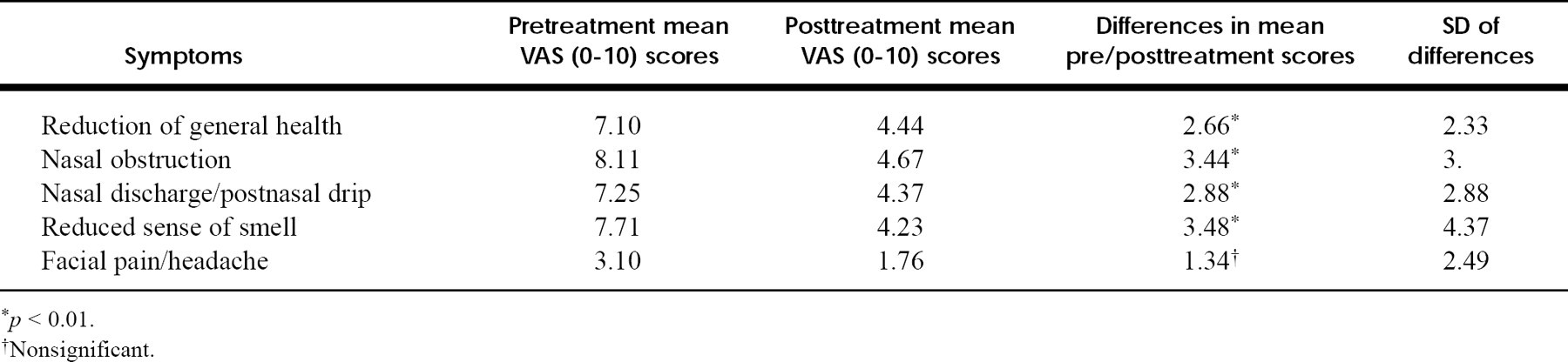
p < 0.01.
Nonsignificant.
TREATMENT PROTOCOL
The patients were randomly divided in two groups: group 1 was treated with a total dose of 560 mg oral fluocortolone for 12 days; and group 2 was treated with a total dose of 715 mg oral fluocortolone for 20 days. The oral steroid medication started with 100 mg fluocortolone in both groups with a progressive reduction of 10 mg. The steroid reduction was performed daily in group 1 during the entire study period and every second day in group 2 after the sixth day of therapy. Additionally, a nasal steroid spray (budesonide, 2 × 0.2 mg/day) was administered during the study period. Medical treatment started after the initial MRI. MRI of the nose and the paranasal sinuses and the patients' self-assessments of symptoms were repeated after the steroid treatment. The duration between the first visit and the reexamination was a mean of 13.6 (SD = 0.84) days in group 1 and 20.6 (SD = 1.4) days in group 2.
MRI Technique and Data Evaluation
All scans were done on a 1.5-Tesla unit (Gyroscan ACS-NT; Philips, Hamburg, Germany). T2-weighted turbo spin echo sequences were obtained with a repetition time of 3000 msec and an echo time of 120 msec in the transverse and coronal planes. Slice thickness was 5 mm with a 0.5 mm intersectional gap. The acquisition matrix was 250 × 512, and the field of view was 230 mm, giving a spatial resolution of 0.5 × 0.9 mm. No MRI contrast medium was given. No topical nasal decongestant was administered before the MRI examination.
Results of digital image processing of MRI scans
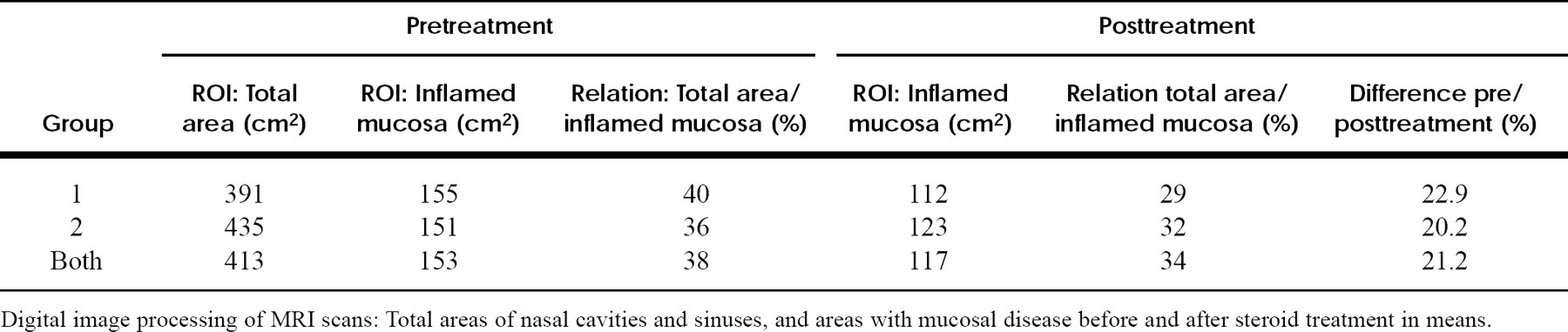
Digital image processing of MRI scans: Total areas of nasal cavities and sinuses, and areas with mucosal disease before and after steroid treatment in means.
Localization of mucosal inflammation in anatomic areas and changes of disease after steroid therapy
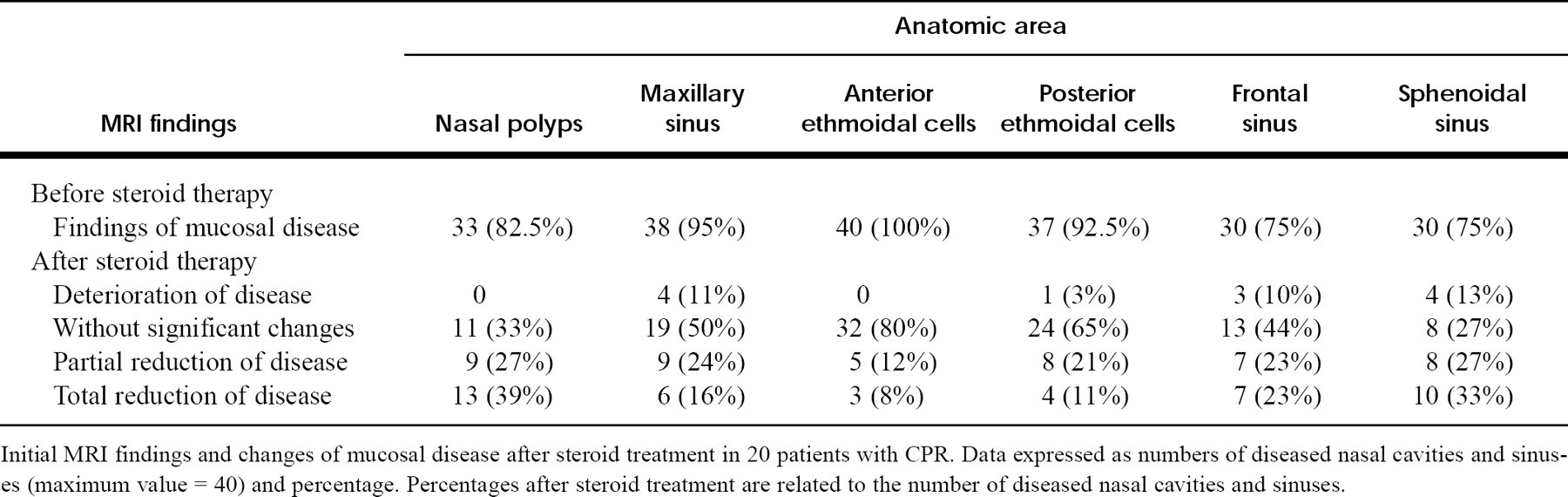
Initial MRI findings and changes of mucosal disease after steroid treatment in 20 patients with CPR. Data expressed as numbers of diseased nasal cavities and sinuses (maximum value = 40) and percentage. Percentages after steroid treatment are related to the number of diseased nasal cavities and sinuses.
Digital Image Processing
The MRI images of the patients were converted to a tagged image file (TIF) format for digital processing on an IBM-compatible workstation. All data were computed in the Image Pro Plus program (version 1.2; Media Cybernetics, Sliver Spring, Md.). First, the gray-scale pictures were converted to a 256 pseudocolor image. Second, pixel scales of images were calibrated. Third, all regions except the nose and the paranasal sinuses (region of interest [ROI]) were cut away on the MRI scans. Identical ROIs were used for the evaluation of disease before and after the steroid treatment. Fourth, a histogram of the polypoid mucosal inflammation was scanned. Fifth, digital counts of the areas with and without mucosal inflammation were performed.
RESULTS
The 20 patients included in this study had a mean age of 45.8 years (range 30 to 68 years), 15 were male and 5 were female, and 8 had type 1 allergy. ASA (anti-steroidal analgetic) intolerance was found in 15% of the patients with oral aspirin provocation. Nine patients did not show any sign of allergy in tests. All subjects completed the study periods. No major side effects were recognized.
Subjective Symptoms
Before steroid treatment the major symptoms were nasal obstruction (VAS mean = 8.11), hyposmia (VAS mean = 7.71), and reduced general health (VAS mean = 7.11), each assessed by 19 patients. Seventeen patients reported nasal discharge and/or postnasal drip (VAS mean = 7.25). Only half of the patients initially had headache (VAS mean = 3.10).
Three patients (2, 3, and 14) were completely free of symptoms after the steroid treatment. The results of the VASs are summarized in Table 2. Multivariate analysis of variance was used to test the correlation between patient symptoms before and after steroid treatment. Reduced general health, nasal obstruction, nasal discharge, and reduced sense of smell, as assessed on the mean VAS, were significantly improved after the steroid therapy. No statistically significant differences were observed between the two groups.
Pearson's test was performed to check bivariate correlations between the reduction of symptoms in VAS and the reduction of the sinusitis in MRI. The correlation was found to be significant at the 0.01 level for general health (r20 = 0.70), nasal obstruction (r20 = 0.79), and nasal discharge (r20 = 0.71).
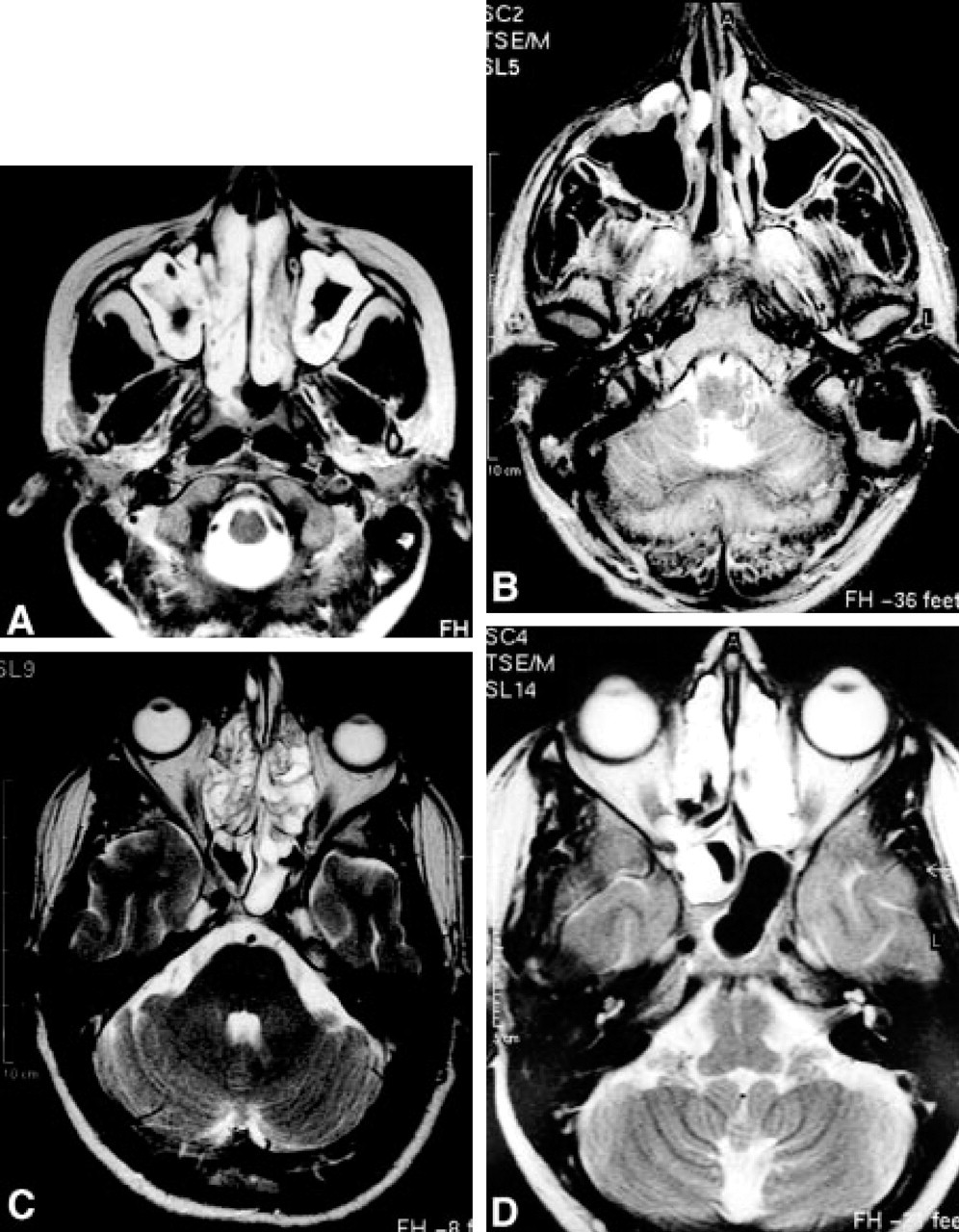
Examples of MRI findings before and after steroid treatment. Mucosal inflammation in transverse MRI scans.
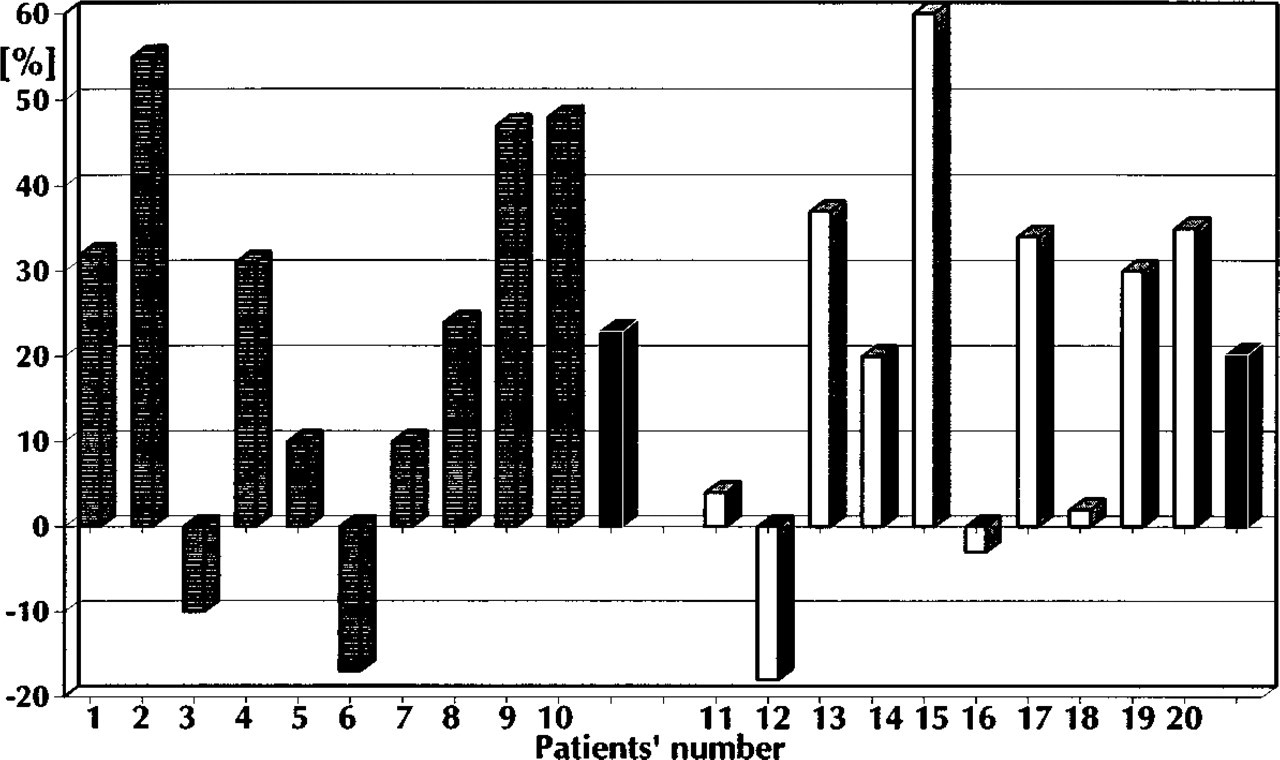
Differences between areas with mucosal inflammation in MRI before and after steroid treatment. Digital image processing of MRI scans: individual changes of areas with mucosal disease in patients after steroid treatment.
Reduction of Chronic Inflammation in the Sinuses and Nasal Cavity in MRI
The initial MRI showed total or subtotal narrowing of sinuses in all patients and nasal polyposis in 80%. Polypoid masses were seen as a high signal intensity on the T2-weighted image against the black background of air or cortical bone. Examples of reduction of mucosal inflammation in the maxillary sinus and sphenoidal sinus are shown in (Fig. 1).
Digital Image-processing of MRI Scans
The nose and paranasal sinuses were outlined as ROIs in MRI scans, and digital counts of areas were performed in the image-processing program. Total area of the nasal cavity and the paranasal sinuses was found to be a mean of 390 cm2 in group 1 and 435 cm2 in group 2. Within the ROI, the mean mucosal inflammation was computed before (group 1: 155 cm2, group 2: 151 cm2) and after (group 1: 112 cm2, group 2: 117 cm2) steroid therapy. There was no significant difference between the two treatment groups. Data of MRI image processing are summarized in Table 3.
The patients did not respond uniformly to the steroid treatment. Digital counts of the inflamed mucosa in MRI revealed a significant reduction (30% to 60%) of CPR in 50% of our patients ((Fig. 1)). A moderate improvement of CPR (10% to 24%) was revealed in MRI scans of patients 5, 7, 8, and 14. No efficacy of the steroid therapy was observed in three patients. Fifteen percent showed a moderate progression of the mucosal disease during steroid therapy. Patient outcome evaluated by MRI image processing are plotted in (Fig. 1).
The efficacy of steroid treatment was recognized in all etiologic groupings. The best improvement of the CPR in MRI was observed in patients with CPR and allergy, but small numbers of patients avoided statistical significance.
Furthermore, steroid effects on polypoid masses were heterogeneous in different anatomic areas. Best results were obtained from the sphenoid. In this region the disease was diminished completely in 10 sinuses and was partially reduced in 8 sinuses after the steroid treatment. The polypoid masses were reduced distinctly in frontal sinuses (46%) and maxillary sinuses (40%). However, sinusitis in the anterior ethmoidal cells was improved, but 80% of the cells remained without significant changes. Data of the localization of mucosal inflammation in different anatomic areas and changes of disease are condensed in Table 4.
DISCUSSION
The benefits and risks of steroid treatment on symptoms in noninfectious rhinosinusitis and in nasal polyposis are generally recognized. 12 However, investigations reporting on the efficacy of systemic or combined (systemic and local) steroid treatment in these diseases are almost lacking. 13 In this series a combined short-term steroid therapy was highly effective in CPR. In a review of the literature, we retrieved only three series reporting on effects of systemic steroids in nasal polyposis and chronic rhinosinusitis. 5,6,11 Procedures of diagnosis and treatment performed in previous studies were not uniform.
Lildholdt et al. 5,6 published two series about patients with nasal polyposis. In the first study in 1988, Lildholdt 6 randomly assigned 53 patients to either surgical removal of visible polyps with a snare or a depot injection of 2 ml betamethasone suspension. In all patients a nasal spray of beclomethasone dipropionate was administered during the 1-year study period. Both regimens caused substantial and equal increase in nasal expiratory peak flow. The sense of smell improved initially but was not maintained at the end of the 1-year observation period.
In the other study Lildholdt et al. 5 randomly assigned 33 patients who failed to respond to the initial treatment with topical budesonide powder to treatment with depot injection of steroid or polypectomy with a snare. By acoustic rhinometry the square area of the nasal passages was measured before and after the injection of the steroid deposit. They found that only 15% of all patients did not respond satisfactorily to the nonsurgical treatment given. After 1 year of continuous topical therapy, there was no difference between the two groups with regard to any effect variable. Lildholdt et al. concluded that primary treatment of nasal polyps should be medical and that surgery is recommended only in patients, resistant to medical therapy.
In our series nasal polyposis was reduced significantly in 27% and diminished completely in 39% of involved nasal cavities. No radiologic findings were considered in the series of Lildholdt et al. 5,6 to establish the reduction of sinusitis, limiting the comparability with our data.
For 16 days van Camp and Clement 11 treated 25 patients who had massive nasal polyposis and who were eligible for FESS with oral prednisolone (total dose = 570 mg). Additionally, doxycycline was added in “cases of infection.” The authors studied the reduction of sinusitis by rhinoscopy and CT scans. 11 The interval between the CT scans varied from 2 weeks to 2 months after the end of the steroid treatment.
Because no data were given about the numbers of patients treated with antibiotics, it could not be excluded that the effect on sinusitis reported by van Camp and Clement 11 depended only on steroids. However, of the 22 patients with visible polyps before steroid therapy, 45% showed a polyp-free nasal cavity and 36% showed a clear involution after the steroid treatment. Fifty-two percent of the patients showed improvement of sinusitis judged by CT scans, 48% did not respond to steroid therapy, and none deteriorated. The best results were evaluated from patients with ASA intolerance. 11
Digital counts of inflamed mucosa in MRI revealed a reduction of CPR in 70% of our patients, particularly a significant reduction of more than 30% in 10 of 20 patients. Furthermore, 15% of patients did not respond, and 15% showed moderate progression of the mucosal disease after the steroid therapy.
The differences between the results reported by van Camp and Clement 11 and our findings are perhaps the result of the steroid dose and the methods used for the data evaluation. CT scan without contrast is the current imaging method of choice for chronic sinusitis and should be available to the endoscopic surgeon for all surgical procedures. 14 Some authors use numeric scores for quantifying the radiologic findings in extensive sinus disease. 15 van Camp and Clement evaluated the findings on CT scans with a staging scheme, using a 0-3 scale for the maxillary, frontal, and sphenoidal sinus and a 0-2 scale for the ethmoidal sinus. Similar staging systems vary between interobserver and intraobserver agreement, producing unstable results. 16 Therefore a digital image-processing program was used to evaluate steroid treatment in our study. MRI scans were performed to avoid risks of radiation caused by CT. In a previous series, 17 MRI was used mainly to facilitate the diagnosis of nasal and paranasal sinus neoplasms and fungal disease. In this series, MRI scans revealed excellent details of soft tissue changes in the sinuses, suitable for digital image processing and research of drug effects in sinuses.
The efficacy of steroid treatment as determined by MRI findings was independent from the fluocortolone dose, perhaps because of the slight difference between steroid doses administered in this study. However, evaluation of systemic steroid therapy in MRI divided the patients in a group of responders and nonresponders, whereas symptoms improved in patients without objective reduction of sinusitis. Steroids have a proven effect on mediators of inflammation and on the reduction of antigen-presenting cells, T cells, epithelial mast cells, and particularly eosinophils in the airway mucosa. 13 These effects are initiated by their binding to a specific cytoplasmic glucocorticoid receptor. 18 It remains unclear which immunologic mechanism is responsible for steroid resistance. The efficacy of steroid treatment in CPR could not be explained by considering etiologic factors (i.e., allergy or ASA intolerance). Further immunologic investigations are necessary to understand the pathogenesis of CPR.
Interesting information was obtained from evaluation of steroid effects on polypoid masses in different anatomic areas. The reduction of inflamed mucosa was best in sphenoidal, frontal, and maxillary sinuses. This observation is supported by data of van Camp and Clement. 11 Messerklinger 19 and later Stammberger 20 suggested that disease in the anterior ethmoid sinus area was the cause of secondary inflammatory disease in the frontal and maxillary sinus. The better efficacy of steroids in the large sinuses may be the result of reverse evolution of inflammatory processes.
CONCLUSIONS
A combined short-term steroid therapy is highly effective in CPR. In our MRI study it reduced the chronic polypoid inflammation in the large sinuses and in the posterior ethmoid significantly in 50% of patients and subjective symptoms in 80% of patients. However, this therapy is insufficient in the anterior ethmoid and cannot replace the current surgical treatment concept of the osteomeatal complex in CPR.
FUTURE DIRECTIONS
The indication for such a short-term steroid therapy is the preoperative treatment. It facilitates FESS by reducing the extent of surgical procedures, the time, and thereby the risks of sinus surgery.
To receive the tables of contents by e-mail, send an e-mail message to
Leave the subject line blank, and type the following as the body of your message:
Subscribe oto_toc
You can also sign up through our website at http://www.mosby.com/oto.
You will receive an e-mail message confirming that you have been added to the mailing list.
Note that TOC e-mails will be sent when a new issue is posted to the website.