
Abstract
The treatment of a patient with imminent airway obstruction caused by a malignant tumor of the larynx is an uncommon clinical problem. These cases need to be evaluated, diagnosed, and managed with care, skill, speed, and above all, appropriateness of intervention. Three methods are available to control the airway: tracheostomy, emergency laryngectomy, and controlled tracheal intubation with or without tumor debulking. Two groups of patients had their airways managed either by tracheostomy and delayed elective surgery or by emergency laryngectomy. There was no survival advantage between the groups, and no increased risk of stomal recurrence was demonstrated. If time permits, the patient is considered suitable, and adequate anesthetic and surgical instrumentation is available, it is currently recommended that the obstructing laryngeal tumor be debulked by cold-steel or, preferably, CO2 laser and that the emergency situation be stabilized and the definitive treatment of the patient be converted to an elective procedure without the need to create a tracheostomy.
Treatment of the patient with a difficult airway can be one of the most challenging problems in clinical medicine. In such cases the otolaryngologist is often involved as either the primary surgeon or as a consultant, often on an urgent or emergency basis. 1 Because no standard definition of the difficult airway was previously available in the medical literature, the ASA Task Force created a working definition whereby a difficult airway was defined as “the clinical situation in which a conventionally trained anesthesiologist experiences difficulty with mask ventilation or tracheal intubation, or both.” 2 Every year many patients admitted to the hospital die of upper airway obstruction despite our expertise because intervention is delayed. Inexperienced physicians tend to rely on blood gas analysis and other late signs of obstruction such as cyanosis and other vital-sign changes. Respiratory failure caused by pulmonary problems is far more common, and therefore treatment for upper airway obstruction incorrectly mimics lower airway obstruction with devastating results. Upper airway obstruction progresses far more rapidly and may not be controllable under less than ideal circumstances. A system of staging upper airway obstruction has been formulated 3 and as a result can determine treatment protocols. The staging system recommended is clinically based and ranges from stage I—in which there are no subjective signs of shortness of breath, respiratory rate is normal, and no stridor is present—to stage IV—in which the patient is cyanotic, has severe stridor, and may eventually have cardiac arrest.
The causes of upper airway obstruction are many and varied. A practical means of separating them is in terms of whether they present acutely (over a few hours) or chronically (over days or longer). The patient's age is also important in distinguishing the cause of obstruction: congenital airway anomalies predominate in the young child, but tumor is a much more common cause of airway obstruction in the adult, particularly in a patient with the appropriate risk factors of tobacco and alcohol use.
CLINICAL PRESENTATION OF LARYNGEAL CANCER
In the early stage of laryngeal cancer, hoarseness is the most frequent symptom. However, additional symptoms at presentation can vary from the presence of a metastatic cervical lymph node in a supraglottic carcinoma to dyspnea and stridor in an exophytic or advanced glottic or transglottic carcinoma. Other symptoms associated with the presence of a laryngeal cancer include a muffled voice, aspiration pneumonia, dysphagia, hemoptysis, and rarely a sore throat or occasionally otalgia.
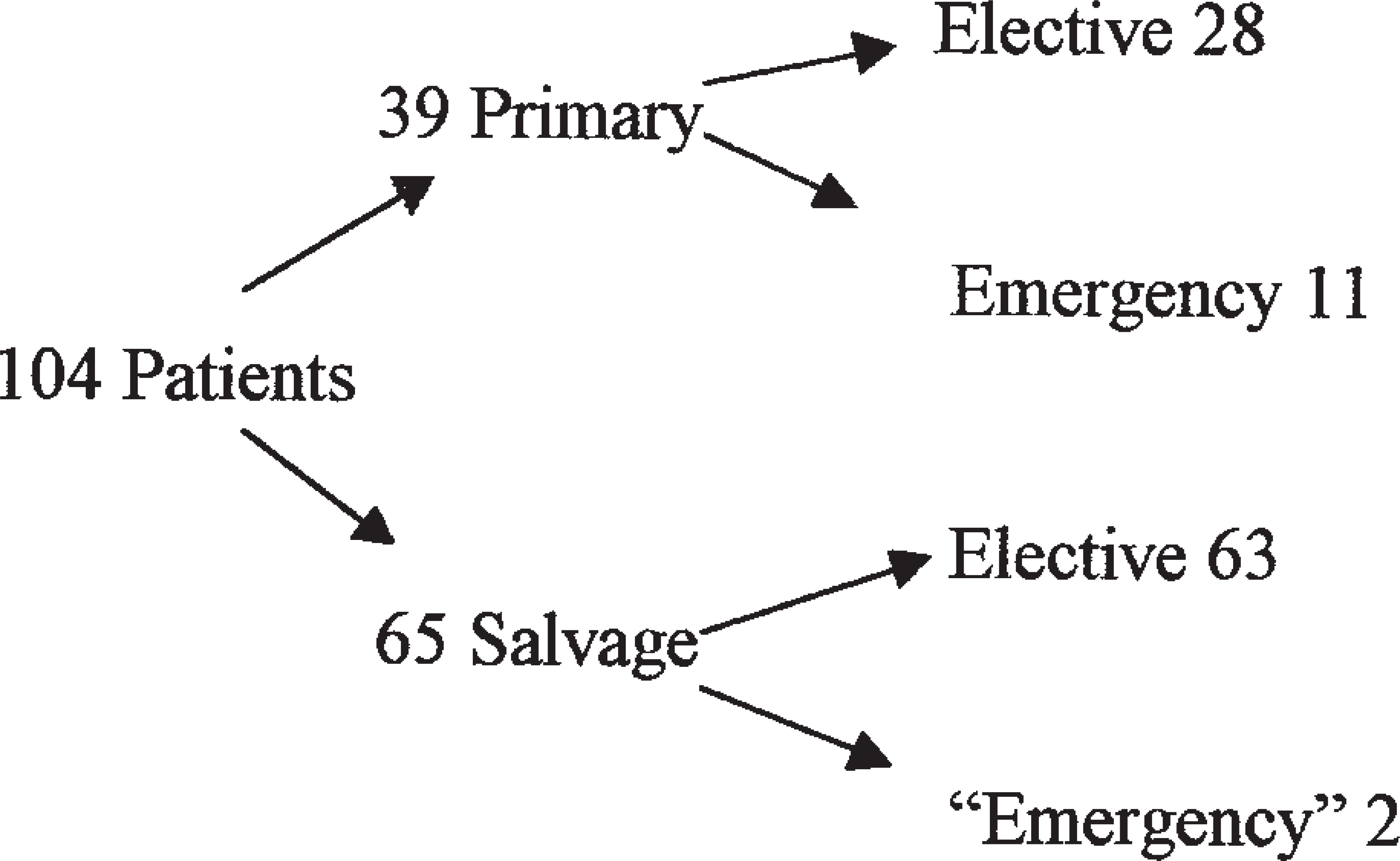
In the United Kingdom the incidence of laryngeal cancer is 40 per million per year, with a peak in the 55-to 65-year age range and a male-to-female ratio of 8:1. It is estimated that only 5% of “new” undiagnosed laryngeal cancers will present with severe dyspnea and/or stridor (Fig. 1). The management of laryngeal cancer varies depending on where the patient is treated. The consensus of opinion among European and Canadian radiotherapists and laryngologists is that most laryngeal cancer can be controlled by radical radiotherapy, surgery being reserved for recurrence or radiation failure. 4 In North America, South America, parts of Asia, and Southern Europe, the preferred treatment for laryngeal cancer irrespective of clinical stage is surgery with or without postoperative radiotherapy.
Surgical management of laryngeal cancer: Nottingham (1983-1990).
Laryngeal cancer: Management principles
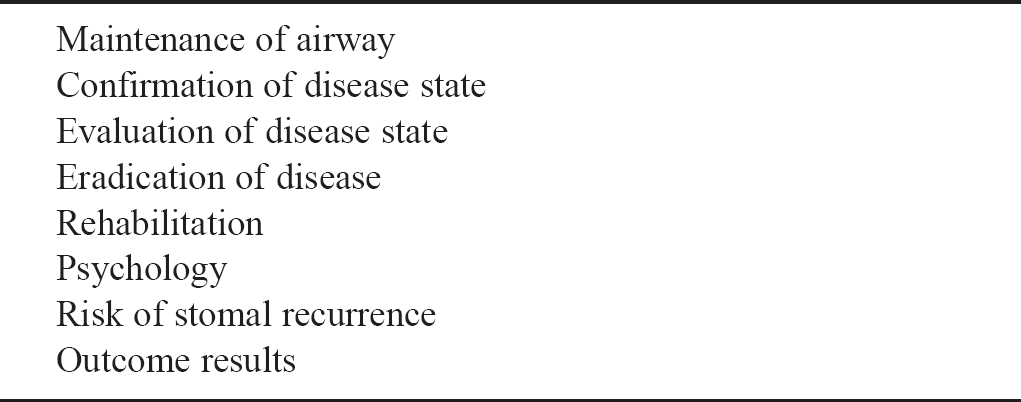
Patients who present electively for management of a laryngeal cancer should be treated along the general principles as listed in Table 1. Patients who present with imminent airway obstruction differ only in that, if the airway is lost, a semiurgent clinical situation becomes a life-and-death situation. Should this situation happen, any method used to establish an airway, depending on the caliber and grade of the medical attendee, to maintain respiration and life is the objective of patient treatment. If the patient has moderate dyspnea, stage III, temporizing measures—including the use of humidified oxygen, helium-oxygen mixture, and monitoring of the clinical situation by pulse oximeter—may be used as part of the initial treatment of the patient with laryngeal airway obstruction. Such patients need to be individually monitored so that any deterioration in the respiratory effort can be observed and “instrumental intervention” can be immediately summoned. If it is considered or known that the extent of the laryngeal tumor involves the distal trachea, other methods of patient oxygenation may need to be considered, such as cardiac bypass with conventional extracorporeal oxygenation techniques. This technique requires that the patient be heparinized, or the heparin-bonded membrane extracorporeal oxygenation system could be used to eliminate the use of a tracheostomy until after definitive surgery.
CLINICAL DILEMMA IN AIRWAY MANAGEMENT
A secure airway must be obtained immediately in those patients with imminent airway obstruction caused by laryngeal cancer. Three options have been described to achieve this objective: tracheostomy, emergency laryngectomy, and orotracheal intubation with tumor debulking.
Each of these maneuvers to secure a stable and safe airway for the dyspneic patient has evolved over time. With increasing knowledge of tumor behavior and improvements in anesthesia and surgical technology, there are arguments over why one method of airway establishment is better than another.
Tracheostomy
The indications for the formation and surgical creation of an opening into the trachea are well described and are an accepted management of acute airway obstructive upper airway in both children and adults. 5 However, the creation of an emergency tracheostomy under either a local or general anesthetic before definitive elective treatment of a patient with a laryngeal cancer is associated with a poor survival rate because of stomal tumor seeding. More immediate complications of tracheostomy include sepsis, tube obstruction, or inadvertent removal or misplacement of the tracheostomy tube. The creation of a tracheostomy with the patient under local anesthesia usually is performed in haste and often with considerable difficulty because the patient is restless and distressed. The incision and subsequent opening into the trachea may transect malignant tissue, which in extensive or advanced disease may be present in the prethyroid muscles, the prethyroid lymph nodes, and the thyroid isthmus itself. The cancer may be located in the subglottic area or may involve the trachea, which may not have been anticipated before the surgery. If the patient and the clinical situation are favorable, once the airway has been secured the patient can be anesthetized, and the extent/type of tumor can be evaluated by endoscopic biopsy. Not infrequently such an emergency situation has to be managed by inexperienced physicians, and as a result of their lack of experience, the formal evaluation of the tumor extent may be deferred to a later time, until the patient and the clinical situation have stabilized. At this point some of the patients may refuse further treatment, most likely the suggestion of total laryngectomy, because their breathing difficulty has been relieved by the formation of a tracheostomy. If the biopsy confirms malignancy, most frequently squamous cell carcinoma, and a total laryngectomy is agreed upon, the operation must of its nature be performed through a contaminated field with the additional risk of postoperative complications. Occasionally repeated biopsies may fail to confirm the suspicious likelihood of malignancy for some weeks. 6 In a review of transglottic carcinoma, 7 the patients who required a pretreatment tracheostomy had a lower prognosis than those who did not, and stomal disease developed in many of the former patients. It has been suggested that patients with airway difficulty or stridor are a self-selected group of patients, 8 usually men. These tumors are generally more advanced in stage, larger, and as a result have a higher risk of cervical nodal metastasis. A review of advanced laryngeal cancer presenting and treated by tracheostomy followed by total laryngectomy showed that there was a higher risk of stomal recurrence in patients whose tumors were located in the glottis than in those whose tumors were located in the supraglottis. 9 This observation of the importance of tumor site location and the risk of stomal recurrence has also been reported in subglottic tumors treated by tracheostomy and was considered to be the result of the presence of paratracheal metastatic glands rather than wound contamination. 10 Analysis of the creation of a preoperative emergency tracheostomy as an independent variable 11 has been found to be nonsignificant in the development of stomal recurrences; it is considered that submucosal spread and, more likely, metastatic disease to the paratracheal nodes are the most plausible pathologic explanations.
Controversy exists as to where to position the tracheostomy if it is necessary to perform such a procedure to preserve life. Baluyot et al. 12 recommend airway control with a low tracheostomy to avoid entering the tumor field, whereas other surgeons advocate a high tracheostomy through the tumor itself if necessary, because the stoma will or should be excised at the time of definitive total laryngectomy. 13 A problem arises should the patient subsequently refuse surgical treatment and accept radiotherapy as an alternative.
Emergency Laryngectomy
An emergency laryngectomy is defined as “a total laryngectomy performed within 24 hours of admission for a previously untreated and undiagnosed malignancy.” 6
Because of the perceived high risk of stomal recurrence, defined as “a diffuse infiltration of neoplastic tissue at the junction of the trachea and skin,” 13 and the associated dismal long-term patient survival, several authors proposed the concept of emergency laryngectomy to avoid or minimize tumor implantation. 7,13 The performance of a tracheostomy at the start of an emergency laryngectomy irrespective of the tumor location has been reported to be unrelated to the subsequent development of peristomal recurrence. 14,15
Emergency laryngectomy is considered conservative in the sense that preoperative tracheostomy is avoided, usually in an attempt to decrease the risk of stomal recurrence. Postoperative radiotherapy can be given, after histopathologic analysis of the resected specimen, if there is a perceived risk of subsequent stomal seeding. Criticisms of emergency laryngectomy include the reliance on frozen-section pathology to confirm malignancy, considered mandatory before proceeding to surgery, and, if the result is negative, the need to defer surgery because of the lack of prior workup of the patient for the possibility of metastatic disease, second primary disease, other malignancies, and associated respiratory or metabolic diseases. Patients may also be poorly prepared nutritionally or psychologically for surgery and as a result do not truly give informed consent. However, in studies of male patients, many authors have found that patients in respiratory distress are more accepting of an immediate surgical procedure than a prolonged, delayed hospitalization and workup. In Liverpool, McCombe and Stell 16 also noted this patient willingness, and they concluded that an emergency laryngectomy fulfilled its promise by providing symptomatic and definitive treatment and at the same time did not significantly increase perioperative or long-term mortality or the stomal recurrence rate compared with elective laryngectomy. Despite the extensive literature available, there is little evidence to suggest that an urgent tracheostomy to secure the airway—followed after a few days by a definitive laryngectomy, which should include the temporary tracheostoma wound en bloc—is any better than an emergency laryngectomy with respect to the overall long-term patient survival rate and the risk of stomal recurrence.
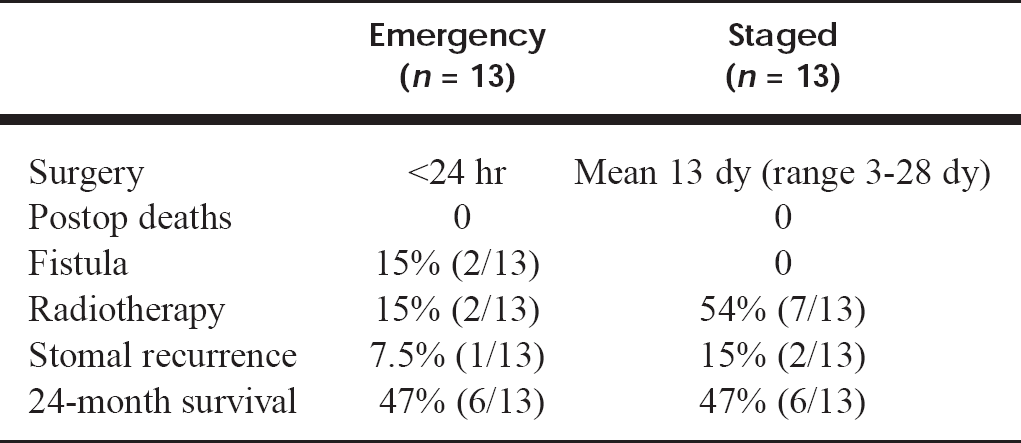
In Nottingham and Leicester during a 10-year period spanning the late 1980s and early 1990s, two groups of patients were identified who had their laryngeal cancers treated by either emergency laryngectomy 17 or emergency tracheostomy and interval laryngectomy 18 (Table 2). This suggests that patients who underwent emergency laryngectomy acquired no survival advantage compared with those who underwent emergency tracheostomy and delayed definitive tumor resection by total laryngectomy (staged laryngectomy). In the National Health Service it is increasingly difficult to schedule out-of-hours surgical time, operating room availability is limited, and senior surgical and anesthetic staff members are potentially unavailable; therefore the preferred current management technique for patients with laryngeal airway compromise has changed from emergency laryngectomy to the creation of a tracheostomy.
Emergency laryngectomy versus staged laryngectomy: Nottingham/Leicester series
Laryngeal tumor debulking: Cold-steel forceps versus laser surgery
Intubation and Debulking of Tumor
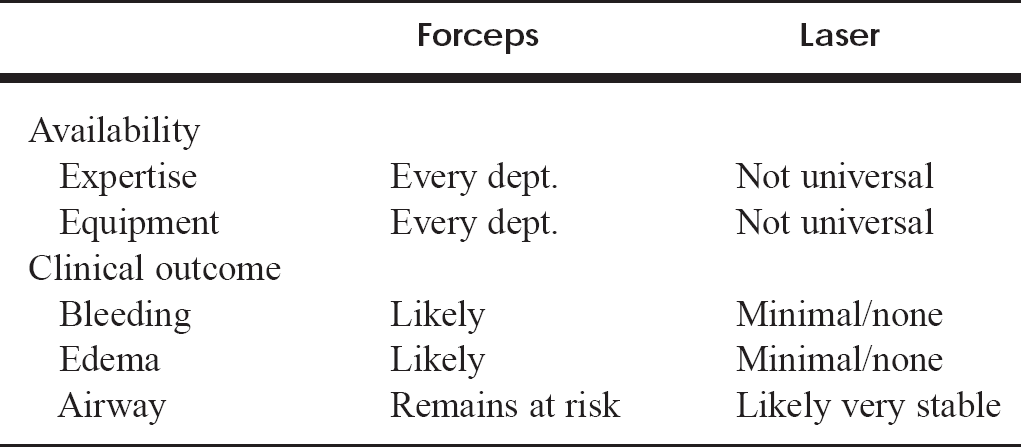
The routine or accepted evaluation of a patient with a potential diagnosis of laryngeal cancer should include evaluation of the tumor site and extent of the disease by direct laryngoscopy and other endoscopy (bronchoscopy with or without esophagoscopy) as indicated; malignancy should be confirmed by biopsy of the tumor with the patient under general anesthesia. The patient with a potential or imminent airway obstruction, considered to be caused by a malignancy of the larynx, should currently be considered suitable for such a similar clinical evaluation. The method of achieving anesthesia in these patients can be summarized as by the following five options: awake orotracheal intubation, awake nasotracheal intubation, general anesthesia with ventilation, direct laryngoscopy/bronchoscopy intubation, or tracheostomy. 19 An alternative to emergency tracheostomy and total laryngectomy is partial excision of the obstructing tumor to effect airway control before definitive therapy. When the airway can be secured by endoscopic control, the tumor can be partially excised or debulked by cold steel, scalpel, forceps, cautery, or vaporization by the CO2 laser. The advantages and disadvantages of cold-steel and laser procedures to debulk laryngeal tumors are shown in Table 3. Debulking of the tumor has a significant risk of hemorrhage and resultant edema, thereby possibly increasing the likelihood of difficulty with extubation and the necessity of creating a tracheostomy. The use of the CO2 laser is the “no-touch” technique vaporization, with less instrumentation of the tumor itself, which ensures that edema, if it occurs, is minimal. Hemostasis is secured in all vessels less than 0.5 mm in diameter. It has been shown that viable tumor cells are not spread during tumor vaporization. 20 The experience and efficiency of primary laser debulking of laryngeal tumors, which has caused airway obstruction, has resulted in the patient being able to be evaluated and allowed to give informed consent to further management. 21–25 Intubation and partial excision of the tumor offer several advantages over emergency laryngectomy. An orderly workup of the patient is possible. Medical problems can be discovered and treated, and a thorough metastatic evaluation performed. In this way, patients who would be best treated nonsurgically can be identified. If a total laryngectomy or partial surgery is necessary, the patient can be better psychologically and nutritionally prepared for surgery. Preoperative speech and swallow therapy can be explained, and a planned rehabilitation program organized. When appropriate, planned preoperative chemotherapy or radiotherapy can be given. The need to perform cancer surgery solely on the basis of frozen-section diagnosis can be eliminated.
The use of a mixture of helium and oxygen (30% helium), humidification of the inspired air, and vital-sign monitoring have been advocated to support ventilation in the compromised airway in the period before laser surgery. The preferred method recommended by Shapshay et al., 23 who recommend laser debulking of the tumor, is awake airway intubation followed by CO2 laser microsurgery with general anesthetic. The removal of the endotracheal tube, along with Venturi jet ventilation for exposure and treatment of any obstructing tumor that may remain in the subglottis and/or upper tracheal area, completes this surgical procedure. It is accepted that tracheostomy may be necessary when intubation of the airway is not possible. Experience with anesthesia given through a cricothyroidotomy and a spinal needle in the obstructing supraglottic cancer has recently been described. 25 It is imperative that the anesthetist be well experienced in this technique because, if the needle or preferably two needles are not used, there could be a buildup of airway pressure with resultant compounding of the clinical situation and development of bilateral tension pneumothoraces. This situation is likely to occur in patients who have a transglottic or glottic subglottic tumors rather than patients who have a supraglottic tumor; in the latter the tumor is a ball valve and has a tendency to impair inspiration rather than expiration of respiratory gases. Connecting an arterial pressure transducer to the second needle, thereby minimizing the risk of airway complications, can monitor the pressure of the respiratory tract. It is recognized that the surgeon and anesthetic and operating room staff must be experienced in microsurgical laser surgery using Venturi ventilation as a quick technique, and they must be confident with the equipment to avoid difficulties and minimize complications.
SUMMARY
It is currently recommended that a patient whose airway is obstructed by laryngeal cancer be evaluated carefully with a nasoendoscope to attempt to determine the location and possible extent of the obstructing tumor. If it is deemed necessary that the tumor be debulked, the preferred method is use of the carbon dioxide laser to secure a stable and safe airway. It is a simple, safe, and effective method and should be considered as a routine alternative to tracheostomy in cancer centers that provide comprehensive otorhinolaryngology-head and neck services.