
Abstract
METHODS: Two studies of psychosocial interventions in head and neck cancer patients at different stages of their disease were performed. We explored the feasibility and effectiveness of different approaches, offered for the first time to this population. The first study concerned long-term group psychological therapy for patients with newly diagnosed head and neck cancer. Quality of life was measured longitudinally for 1 year and compared with that of a control group. The second study comprised a short-term psychoeducational program 1 year after treatment for head and neck cancer. Quality-of-life assessments were made repeatedly from diagnosis until 1 month after the intervention. RESULTS: Thirteen patients started the psychological group therapy, and 8 of them completed both the intervention and evaluation procedure. The quality of life of the therapy group improved more than that of a control group in most areas measured during the study year, in particular psychiatric morbidity, social functioning, emotional functioning, and global quality of life. The results indicate benefits from the therapy, although the therapy group scored worse than the control group at diagnosis. Most of the variables representing functioning and symptoms improved after the 1-week psychoeducational program, especially items reflecting “trouble eating” and “problems enjoying your meals.” Patients' judgments of the intervention quality indicated satisfaction with all separate elements, mostly education, about cancer and the opportunity to socialize with the other guests.
CONCLUSION: These pilot studies suggest that head and neck cancer patients can benefit from different psychosocial interventions. Quality-of-life questionnaires were well accepted and sensitive to changes during the studies. Thus our early findings seem promising and would justify confirmation in larger studies. (Otolaryngol Head Neck Surg 1999;120:507-16.)
About 1100 new cases of head and neck (H&N) cancer are diagnosed each year in Sweden. The tumor location often affects appearance as well as vital functions such as eating, talking, and breathing. Usually patients receive combined treatment with irradiation (external or local) and surgery, and in some cases also chemotherapy. The treatment can aggravate symptoms because of local tissue reactions and mutilating surgery. Despite new treatment strategies, the survival rate has remained almost unchanged for several decades. Therefore, quality-of-life (QL) research has been introduced because a thorough knowledge of QL can be important when considering the optimal treatment, care, and rehabilitation of these patients. So far, few prospective QL studies have been published, 1 but existing data indicate frequent problems with nutrition, pain, and communication. Furthermore, a high degree of psychiatric morbidity has been found, both during treatment and after several years. 2–9
During the last 2 decades increasing interest has focused on social, emotional, and behavioral factors and their potential influence on cancer morbidity and mortality.
Psycho-oncology has become a subspeciality of oncology, and a research agenda for the future has been outlined. 10,11 One research domain concerns different interventions of a psychosocial character and how to reduce affective disorders among cancer patients and improve their QL, because approximately 25% of all cancer patients develop an affective disorder within 2 years of diagnosis. 12 Several studies have been performed, but to our knowledge no study has been published evaluating any psychosocial intervention specifically designed for H&N cancer patients. 13–16
Two pilot studies were designed to explore both the feasibility and efficiency of 2 different intervention approaches. The first study evaluates the effect of group psychological therapy, led by a psychologist, in newly diagnosed H&N cancer patients. QL, including psychiatric morbidity, was measured longitudinally for 1 year and compared with that of a control group. The second study examines the effect of a 1-week psychoeducational program for H&N cancer patients 1 year after diagnosis, and their QLs were followed up longitudinally from the time of diagnosis.
The same standardized QL questionnaires were used in both pilot studies: the European Organisation of Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), a preliminary version of the EORTC H&N cancer module (QLQ-H&N37), and the Hospital Anxiety and Depression (HAD) scale. The QL assessment was performed before, during, and after treatment and, in the second study, also before and after the rehabilitation program. In both studies an evaluation of the intervention included patient judgments of therapy quality through a standardized personal interview.
INTERVENTION I: SUPPORTIVE PSYCHOLOGICAL GROUP THERAPY
Design
Patients in the western part of Sweden with primary H&N cancer are referred to a weekly H&N cancer conference at the university hospital. At this conference all patients living within 40 km of the hospital were invited to participate in the group therapy and answer QL questionnaires 6 times during 1 year. Patients who lived further away were asked to answer only the QL questionnaires and served as the control group. Patients considered unable to answer the QL questionnaires were excluded from both study groups. The QL questionnaires were answered 6 times during 1 year: at the time of diagnosis and 1, 2, 3, 6, and 12 months after the treatment had started. All but the first questionnaire were mailed to the patients. Patients who did not return the questionnaire within 10 days were reminded once.
The including physician also collected data about other relevant diseases, weight, height, weight loss (during the previous 3 months), and time of onset of tumor-related symptoms and evaluated Karnofsky Performance Status. 17 Tumor location according to ICD-9, TNM classification (UICC-1987), and SNO-med code for histopathology were also recorded.
The group therapy was also evaluated by an interview with open-ended questions, performed 2 months after the end of therapy.
A completed questionnaire at diagnosis was a prerequisite for inclusion and was regarded as the patients' informed consent. The study was approved by the local ethics committee on November 9, 1994.
Method
Individual tumor, treatment, and patient characteristics of participants in the group therapy
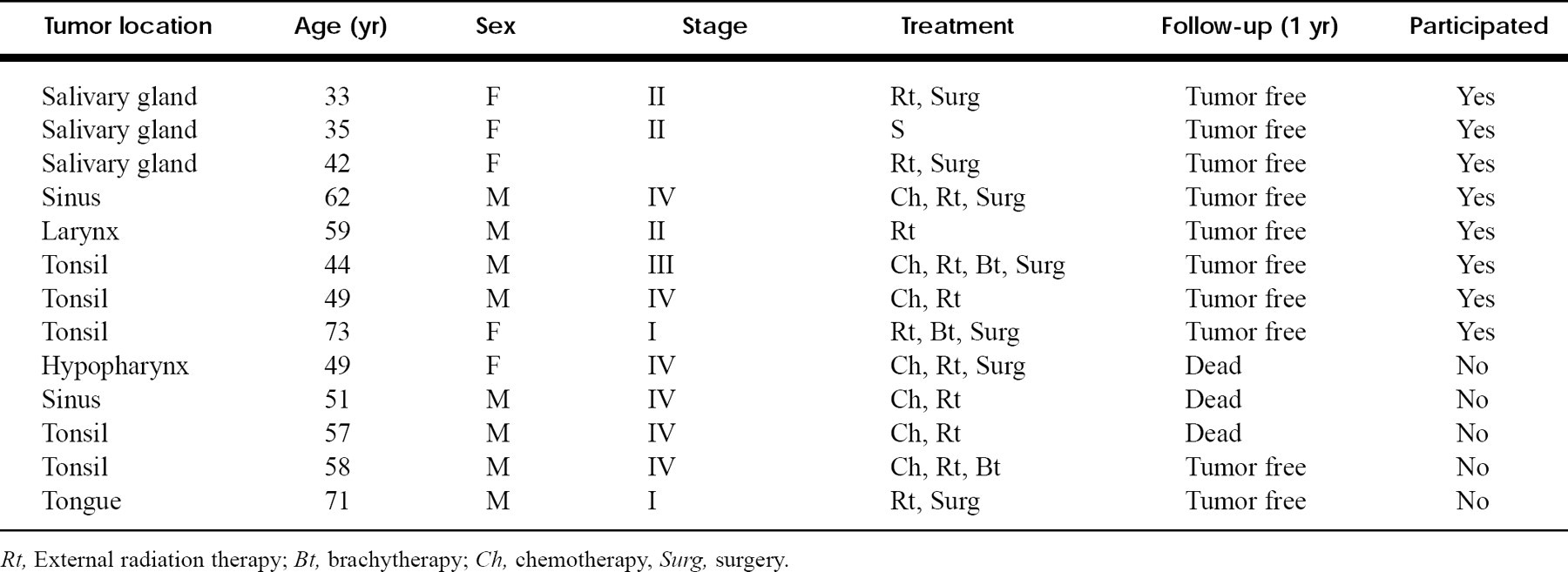
Rt, External radiation therapy; Bt, brachytherapy; Ch, chemotherapy, Surg, surgery.
Patients
At the 1-year follow-up 26 patients (76%) were alive without tumor, 1 patient had been treated for a recurrence, 6 patients were dead, and 1 patient was missing-for unknown reasons.
Results from the EORTC QLQ-C30 and QLQ-H&N37 for patients participating in the group therapy and completing the study
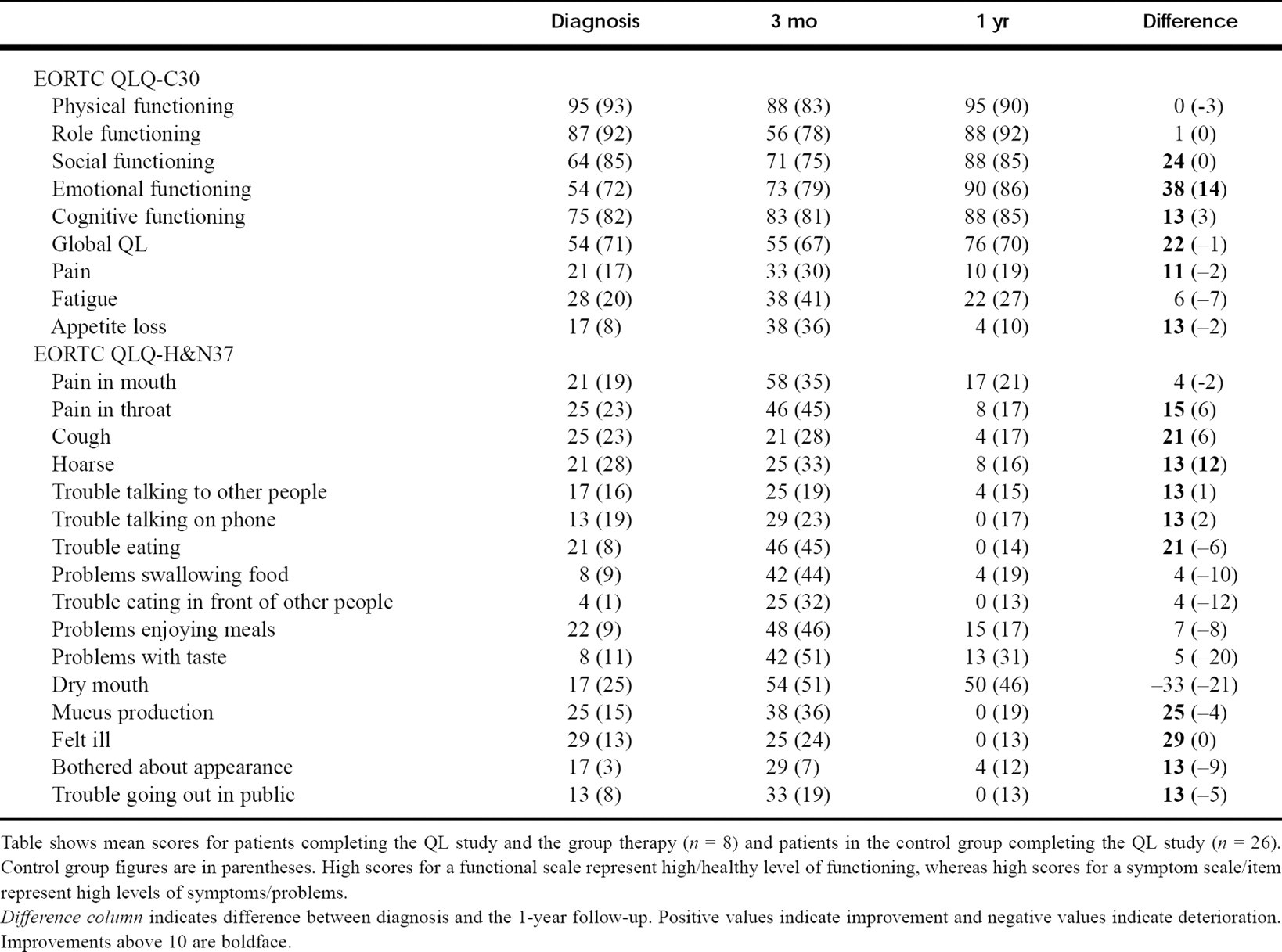
Table shows mean scores for patients completing the QL study and the group therapy (n = 8) and patients in the control group completing the QL study (n = 26). Control group figures are in parentheses. High scores for a functional scale represent high/healthy level of functioning, whereas high scores for a symptom scale/item represent high levels of symptoms/problems.
Difference column indicates difference between diagnosis and the 1-year follow-up. Positive values indicate improvement and negative values indicate deterioration. Improvements above 10 are boldface.
Statistics
For management of data and calculation of the statistics, StatView (Abascus Concepts, Inc., Berkeley, CA) for the Macintosh system of personal computers was used. For descriptive purposes we used means and standard deviations.
Results
Of the 34 control study patients, 31 (91%) answered the second questionnaire, 27 (79%) answered the third and fourth, 25 (74%) answered the fifth, and 26 (76%) completed all 6.
Eight of the invited 42 control patients did not answer the first QL questionnaire and were therefore excluded from the study. The excluded patients were older and had more advanced disease.
To compare the 2 groups over time, only results for patients completing the study are displayed. We tentatively consider a Δ score of 10 or more as a possibly clinically relevant change. Patients participating in the group therapy scored worse at diagnosis for a majority of the questions in both questionnaires (25 of 35 scales or items). At the 1-year follow-up, however, the group had improved in most areas compared with the control group. The improvement (ie, the difference between diagnosis and the 1-year follow-up) was 10 points or more for 6 of 15 of the functions and symptoms in the EORTC QLQ-C30 in the intervention group, compared with 1 of 15 in the control group. The greatest benefit in the intervention group concerned emotional functioning (38 Δ points), followed by social functioning (24 points) and global QL (22 points) ((Fig. 1)). The improvement was more than 10 points for 10 of the 20 symptoms/problems in the EORTC QLQ-H&N37; “felt ill” improved most (29 Δ points), followed by “mucus production” (25 Δ points) and “hoarseness” (21 Δ points) together with “trouble eating” (21 Δ points). Only 1 item improved more than 10 points (“hoarseness,” 12 Δ points) in the control group. Problems with a dry mouth increased in both groups during the study and represented the problem with the highest score at the 1-year follow-up.
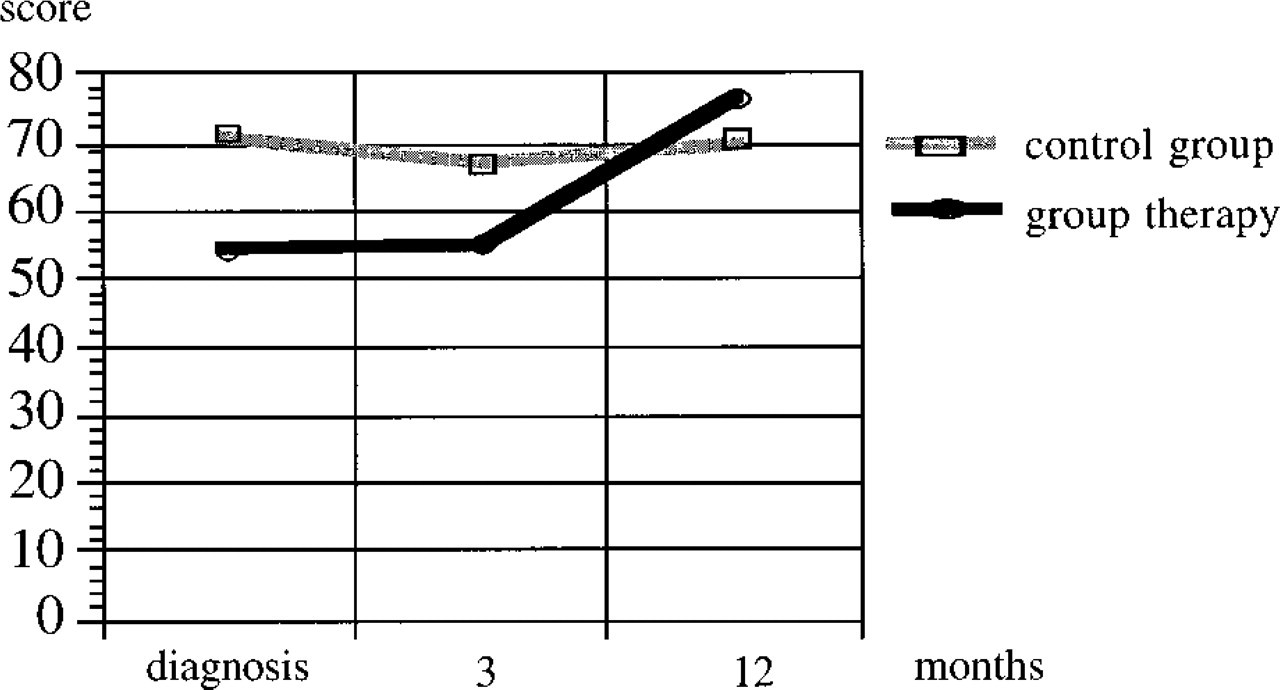
Results, over time, for the therapy and control groups for global QL, a scale from the EORTC QLQ-C30. The higher the value, the better the QL
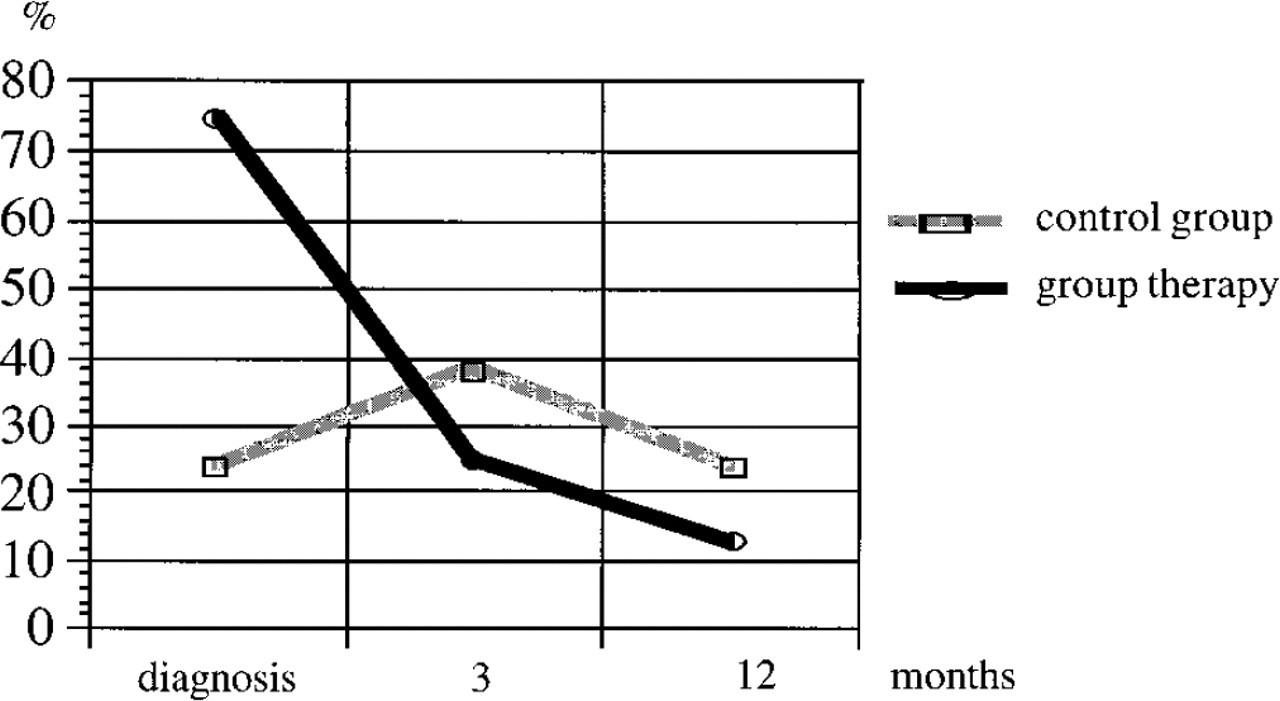
Results, over time, from the HAD scale for the therapy and control groups. Patients scoring above 7 on either the anxiety or depression scale are illustrated as a percent of the total number of patients. Patients are counted only once even if their scores exceed 7 on both scales
INTERVENTION II: SHORT-TERM PSYCHOEDUCATIONAL INTERVENTION
Design
Together with their spouses, patients with oropharyngeal and laryngeal cancer who participated in an earlier longitudinal QL study were invited to a rehabilitation center, Lydiagården, for a 1-week psychoeducational program. Fourteen patients and their spouses could be admitted. Patients were asked in the same order as they had been diagnosed and included in the previous QL study. About one third of the invited patients wanted to participate. For evaluation of the program, QL was measured before and 4 weeks after the intervention. We used the EORTC QLQ-C30, QLQ-H&N37, and HAD scale at both measurement points. The same 3 questionnaires had also been used in a previous QL study, which enabled us to compare QL longitudinally, before, during, and 1 year after treatment with QL before and after the rehabilitation week. A standardized telephone interview was performed for further evaluation of the program. The interview was conducted by a research nurse 3 weeks after the intervention.
Results from the HAD scale for patients participating in the group therapy and the control group who completed the study
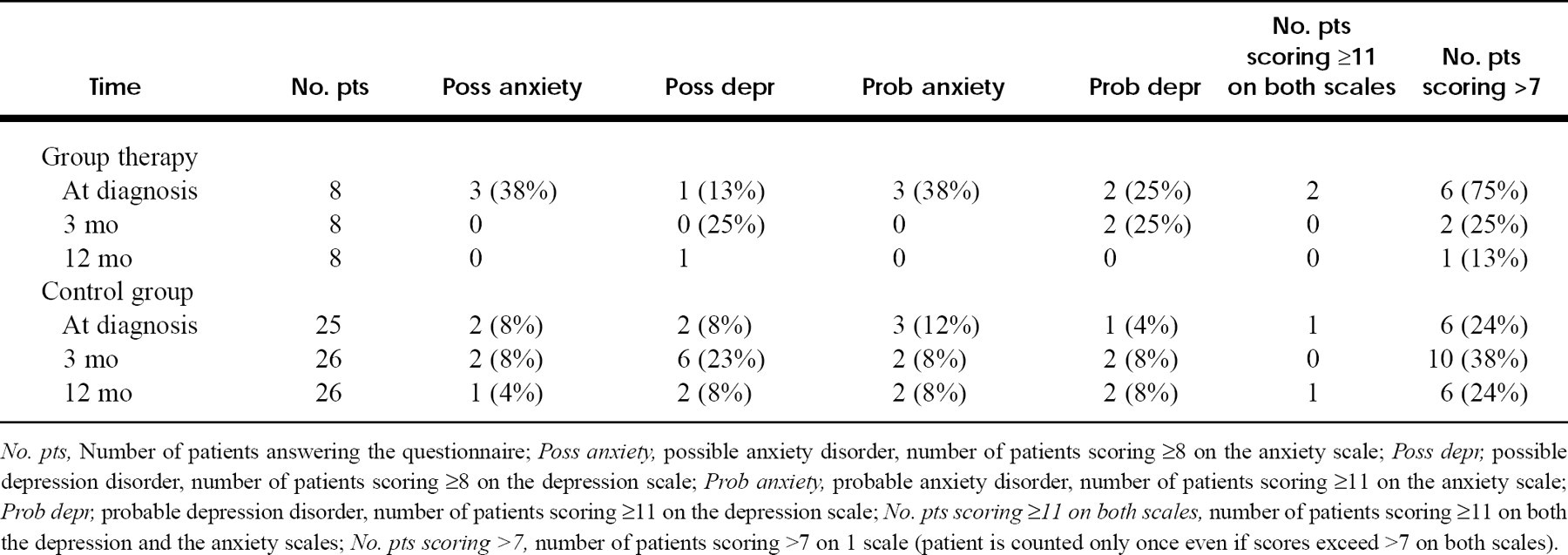
No. pts, Number of patients answering the questionnaire; Poss anxiety, possible anxiety disorder, number of patients scoring ≥8 on the anxiety scale; Poss depr, possible depression disorder, number of patients scoring ≥8 on the depression scale; Prob anxiety, probable anxiety disorder, number of patients scoring ≥11 on the anxiety scale; Prob depr, probable depression disorder, number of patients scoring ≥11 on the depression scale; No. pts scoring ≥11 on both scales, number of patients scoring ≥11 on both the depression and the anxiety scales; No. pts scoring >7, number of patients scoring >7 on 1 scale (patient is counted only once even if scores exceed >7 on both scales).
Results from the interviews evaluating the supportive group therapy.

Method
Lydiagården is a comprehensive rehabilitation center for cancer patients. Together with their spouses, patients are welcome after primary cancer treatment or during a relapse. An intense 1-week program is offered, which is adapted depending on the attendant patients. During the study week only H&N cancer patients were admitted. The program includes an individual appointment with a physician (an oncologist), an educational program about cancer given by a physician, separate group sessions for patients and their spouses led by specially trained nurses, individual and group education by a physiotherapist, and leisure activities such as painting, walking, music, and dancing. A “home-like” environment with good food is emphasized. A report is sent to the patient's ordinary physician after the rehabilitation.
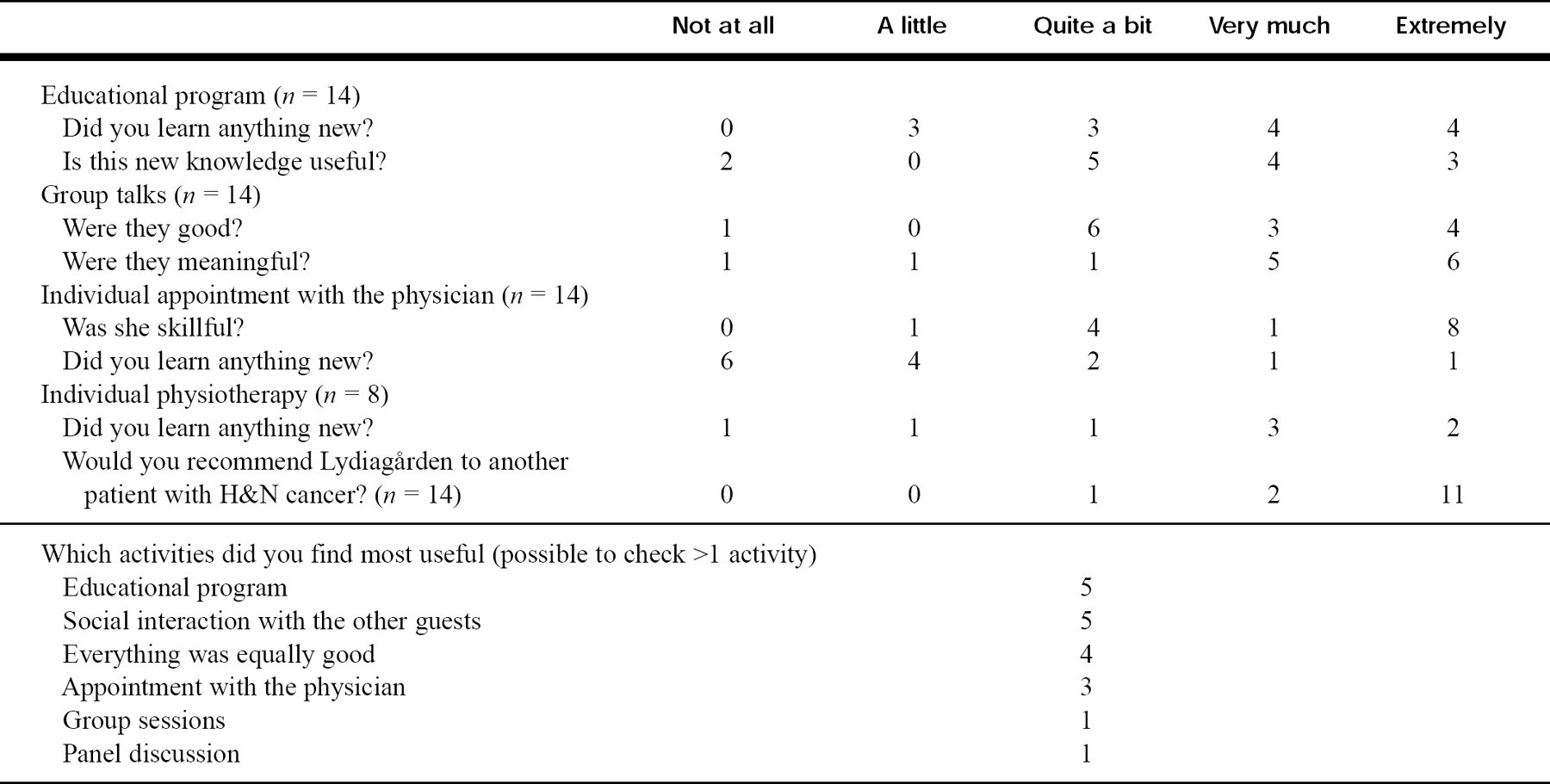
Results from debriefing interview performed 3 weeks after short-term psychoeducational program
Patients
Eleven men and 3 women comprised the study group. The mean age was 57 years (range 21 to 71 years). There were 3 patients with laryngeal carcinoma (stage I), 3 with tonsillar carcinoma (stage III-IV), 7 with oral cavity carcinoma (stage I-IV), and 1 with hypopharyngeal carcinoma (stage III). Most patients had received a combined treatment. The mean time between diagnosis and the rehabilitation program was 16 months, range 12 to 22 months. Thirteen of the patients were living with someone else, and 8 of them brought their spouses. At the time of rehabilitation 2 patients were working, 1 was studying, and the rest were retired.
Results
The results from the telephone interview of all 14 patients are shown in Table 5. The patients appreciated all activities, learned new things, and considered this knowledge useful. Five of the patients mentioned spontaneously that the opportunity to socialize with other guests meant a lot to them. All patients would recommend a week of rehabilitation in this format to other cancer patients. Four of 5 spouses considered the rehabilitation week to be “very good” and 1 “acceptable.” Some of the patients thought they would have benefited more from the activities if they had been given the opportunity to go earlier (ie, 2 to 3 months after finishing the treatment).
The most important results from the EORTC QLQ-C30 and QLQ-H&N37 are shown in Table 6, which includes 3 of the measurement points during the QL study: at diagnosis, just after the end of treatment (3 months after the start of therapy), and at the 1-year follow-up. The mean interval between the 1-year follow-up and the rehabilitation was 4 months. The lowest value for functioning and the highest value for problems/symptoms occurred after the end of treatment. Between the 1-year follow-up and the start of rehabilitation the figures for the EORTC QLQ-C30 were almost unchanged. For the H&N module there were changes, even though half of the problems showed constant values. For most questions no great differences were found between values before and after the rehabilitation. However, the majority of variables reflecting functioning and symptom burden improved somewhat after the rehabilitation (26 of 34 variables). Only 6 variables scored worse, and 3 were unchanged. The greatest improvement was noted for “trouble eating” (17 Δ points), “problems enjoying your meals” (12 Δ points), dry mouth (10 Δ points), and emotional functioning (8 Δ points). Another 5 variables showed improvement of more than 5 points. The only question showing a deterioration by 5 points or more concerned financial problems (7 Δ points).
According to the HAD scale, Table 7, the number of probable clinical cases of anxiety and depression was almost constant throughout the study. The number of possible cases decreased slowly. The number of patients scoring more than 7 on one of the scales decreased after the rehabilitation week.
Results from the EORTC QLQ-C30 and EORTC QLQ-H&N37 for patients participating in the psychoeducational program
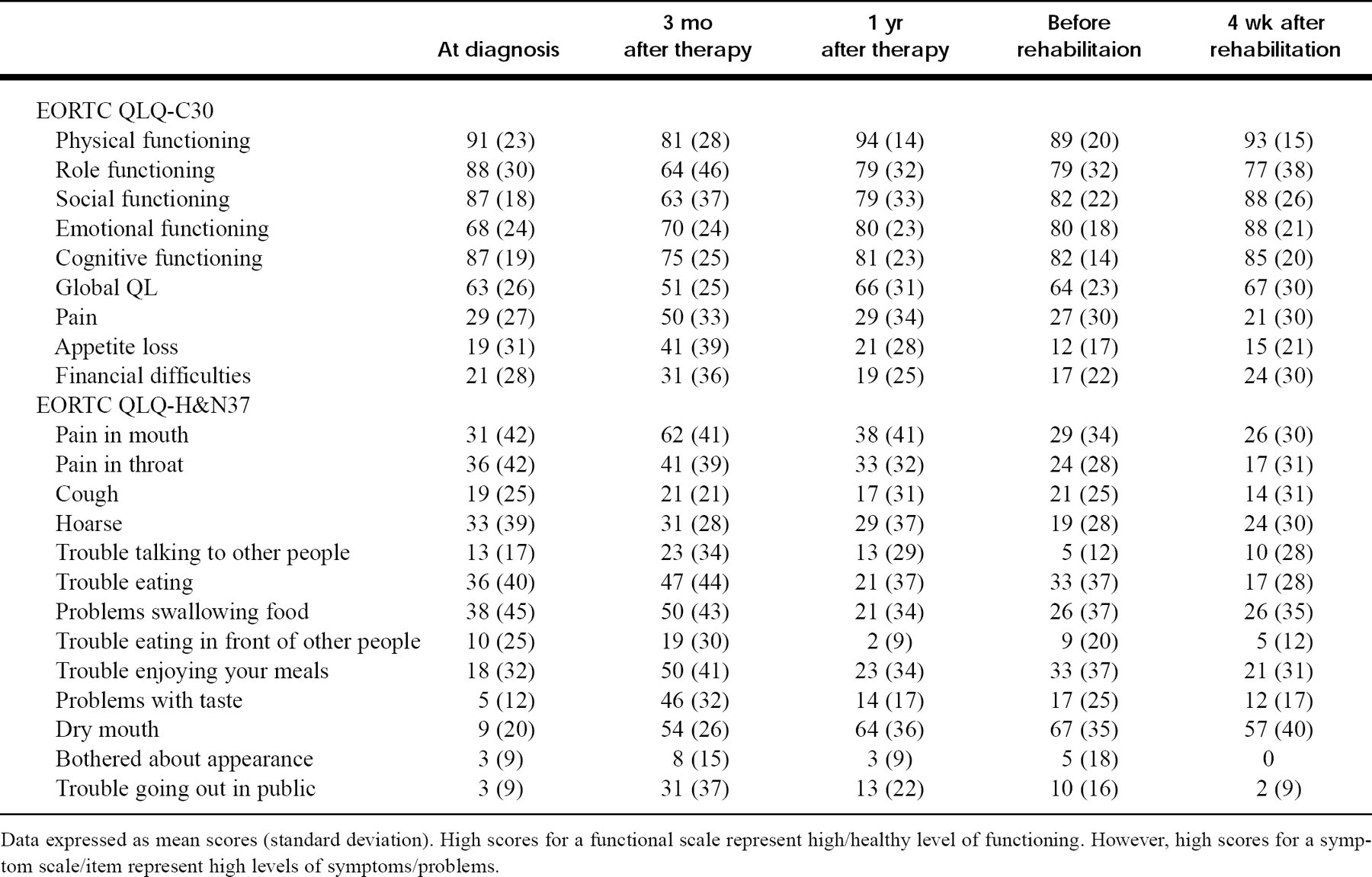
Data expressed as mean scores (standard deviation). High scores for a functional scale represent high/healthy level of functioning. However, high scores for a symptom scale/item represent high levels of symptoms/problems.
Results from the HAD scale for patients participating in the psychoeducational program
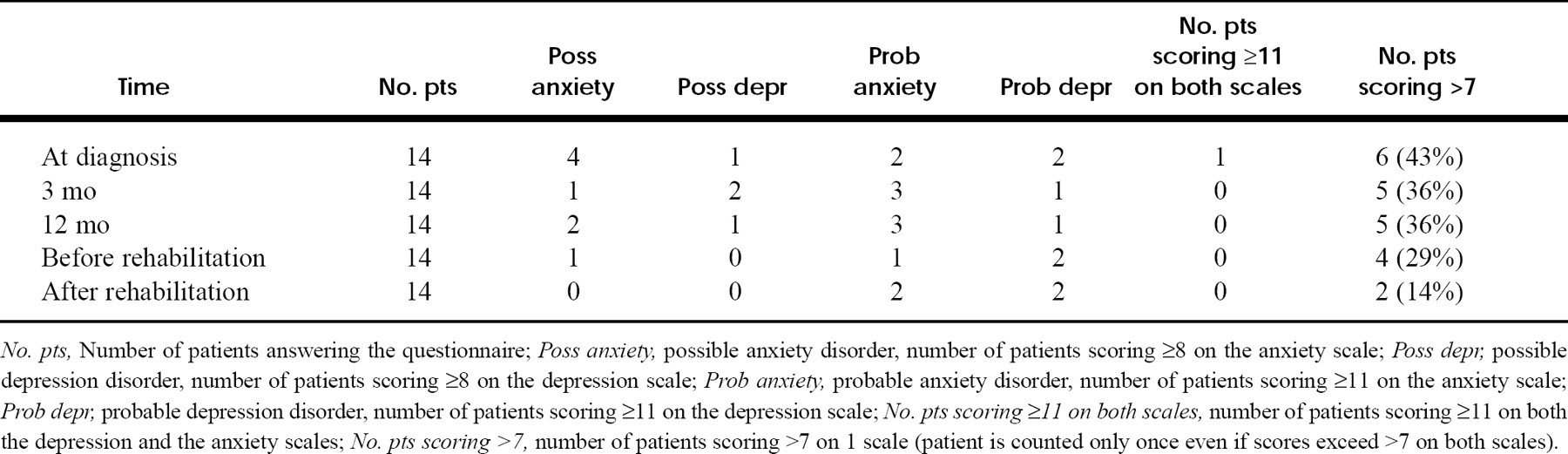
No. pts, Number of patients answering the questionnaire; Poss anxiety, possible anxiety disorder, number of patients scoring ≥8 on the anxiety scale; Poss depr, possible depression disorder, number of patients scoring ≥8 on the depression scale; Prob anxiety, probable anxiety disorder, number of patients scoring ≥11 on the anxiety scale; Prob depr, probable depression disorder, number of patients scoring ≥11 on the depression scale; No. pts scoring ≥11 on both scales, number of patients scoring ≥11 on both the depression and the anxiety scales; No. pts scoring >7, number of patients scoring >7 on 1 scale (patient is counted only once even if scores exceed >7 on both scales).
Discussion
Most studies of psychological support relate to breast cancer patients. The “typical” H&N cancer patient has a different profile because two thirds of the patients are male, the mean age is 67 years, and a large number have alcoholic problems and inadequate social support. The pilot studies presented here aimed to explore the effect of supportive intervention because we had found a high degree of psychiatric morbidity in our previous QL studies when screening with the HAD scale, along with lasting problems caused by the tumor location and treatment. 8,9 The first study related to supportive group therapy, starting at diagnosis, with the aim of reducing the above-mentioned problems during and after treatment. The second study focused on a different period in the course of the disease (the rehabilitation phase) and a different type of intervention (a psychoeducational program). Because both studies were pilot studies and were limited in scope, we refrained from significance testing.
Two groups began the supportive group therapy, a total of 13 patients. These patients were younger and included more women than the control group. As many as 5 patients dropped out at different stages, thereby making it more difficult to create a group atmosphere, something the remaining participants commented on. Compliance in other similar studies varies. 14–16 Perhaps patients are too busy, too weak, and/or too depressed during treatment to feel highly motivated to take part in this kind of therapeutic program. Should the meetings have started after the treatment had finished or does the reaction indicate that the activity is more optional than, for example, the medical treatment?
According to the HAD scale psychiatric morbidity was more common in the therapy group at diagnosis than in the control group ((Fig. 1)). We did not screen for psychiatric morbidity before offering the intervention (ie, all patients were invited to participate consecutively). The group's mean scores for neuroticism and extroversion did not differ from those of the general population. The lack of personality differences between the therapy group and the controls also excluded a selection bias in these respects. It therefore seems likely that the patients who accepted the invitation were more anxious and depressed at diagnosis than the control group. At the 1-year follow-up, however, the therapy group had improved greatly, whereas the number of patients with psychiatric morbidity in the control group was unchanged. The same pattern was found when analyzing the EORTC QLQ-C30 and QLQ-H&N37, especially data representing social and emotional functioning and global QL ((Fig. 1)). The corresponding results from 3 different QL questionnaires support the conclusion that the patients benefited from participating in the group therapy even though the limited number of patients and differences between the 2 groups suggest that cautious conclusions should be drawn. To confirm this, we created a matched control group from our database of 300 H&N cancer patients, previously examined according to the same study design. Two patients were matched for each of the 8 patients completing the therapy. The matched controls had the same tumor location, tumor stage, treatment, sex, and age (±10 years), and they had all completed the study and were tumor-free at the 1-year follow-up. The change in QL score between diagnosis and the 1-year follow-up corresponded numerically between the matched controls and the study control group for the social and emotional functioning, the global QL scores, and the HAD scale. This supports the hypothesis that the group therapy did affect the QL of the patients.
From the second pilot study, we learned that the patients would have preferred to participate at an earlier stage of their disease, preferably 2 to 3 months after finishing their treatment. Nevertheless, when analyzing the QL questionnaire data, we found a pattern of improvement in the majority of functions and symptoms after the intensive short-term psychoeducational program. The greatest improvement was noted for “trouble eating” and “problems enjoying your meals.” This might have been the first time after diagnosis and treatment for cancer that the patients left from their homes. Being with other people with similar problems in a new environment and finding out that eating with other people was not only possible but a pleasure could explain these results. The number of patients scoring above 7 on either the depression or anxiety scale decreased slowly during the study and was in line with the improvement in emotional functioning. It seems likely that the result reflects a true improvement, although it has not yet been established when to regard a change in score on the QLQ-C30 or the QLQ-H&N37 as clinically significant. Deciding when a change in score corresponds to a clinical improvement is an important task, and data of this kind will facilitate the interpretation of changes, especially when the questionnaires are used repeatedly.
CONCLUSION
Patients participating in these pilot studies benefited from the supportive group therapy and the short-term educational program, and the standardized questionnaires were of value in assessing their QLs. It seems worthwhile to replicate the findings in larger studies of psychological support for H&N cancer patients.
We are grateful to psychologist Millevi Tholstrup for leading the group meetings, to oncologist Ingrid Terje, head of Lydiagården, and to research nurse Lena Hörnestam and psychologist Magnus Lundgren for patient interviews. Special thanks to Marita Hellqvist for secretarial help.
The AO/ASIF Distraction Osteogenesis course will be held May 22-23, 1999, in Louisville, KY. It is intended to provide a forum through which attendees may gain a clear understanding of the principles of distraction osteogenesis, as applied in the craniomaxillofacial skeleton, according to AO/ASIF principles and techniques. The chairman is Joseph E. Van Sickels, DDS, and it is accredited by the AO North America. Credit: 12 AMA category 1 CME credits.
For further information, contact the AO/ASIF Continuing Education Office, 1690 Russell Rd, PO Box 1766, Paoli, PA 19301; phone, 800-769-1391; fax, 610-251-5039.