
Abstract
Gastroesophageal reflux (GER) plays a causative role in the development of subglottic stenosis (SGS) in children. This study examined the impact of aggressive antireflux therapy on the clinical outcomes of 35 children. Since 1994, 25 children were treated aggressively with omeprazole and cis-apride before endoscopic surgical repair of their stenoses, which ranged from Cotton grades 1 to 3. Nine patients became asymptomatic on antireflux therapy alone. Endoscopic repair was performed in 16 patients. Endoscopic repair failed in only 1, who required tracheotomy. Before 1994, all children undergoing endoscopic repair of SGS were treated perioperatively for reflux. Endoscopic repair failed in 10 of the 57 children, and all required tracheotomy. The clinical outcome of these 10 patients after aggressive antireflux therapy is described. Five of the 10 have been decannulated. The role of double pH probe testing and the importance of the pharyngeal probe for monitoring the response to antireflux medication are described. The probe data suggest that in some instances GER may be limited to perioperative stress, but in many cases, especially in premature infants with SGS, GER can persist unabated for years and is not outgrown as the patient matures.
Gastroesophageal reflux (GER) plays a causative role in subglottic stenosis (SGS). In 1985 Little et al 1 elegantly demonstrated this in the canine model. Subsequently, increasing emphasis has been placed on controlling GER before the surgical correction of SGS. Gray et al 2 described the improvement in laryngotracheoplasty results with aggressive GER treatment. Burton et al 3 described a child with a 60% SGS comprised of scar and granulation tissue whose stenosis resolved dramatically with antireflux medication after prior treatment with steroids and endoscopic surgery had failed. Given the devastating effects of GER on the larynx and the management of SGS, the impact of aggressive diagnosis and treatment of GER on the clinical course of 35 infants and children with SGS was examined.
METHODS AND MATERIAL
The clinical course of 25 children treated for SGS since 1994 was retrospectively reviewed. These children, aged 1 to 24 months, had the diagnosis of SGS initially confirmed by flexible laryngoscopy, were pH probed, and were treated aggressively for GER before endoscopic repair. After pH probe testing and initial antireflux treatment, 16 patients had their stenoses managed endoscopically and 9 with antireflux medication alone. Review of departmental outcome data revealed that, before 1994, 57 children had undergone endoscopic management of their SGS with only perioperative reflux management. Endoscopic surgery failed in 10 patients, who were then tracheotomized and further evaluated. Their ages at the time of pH probing ranged from 3 months to 7 years. Retrospective review of their clinical course is presented. Appropriate informed consent was obtained for all patients for the pH probe studies and surgeries. The study protocol was reviewed by the institutional review board of the hospital.
pH probe data were obtained for all patients. Most patients underwent double pH probe testing. Two patients, 1 in the tracheotomy-dependent and 1 in the surgery group, had pH probes at outlying hospitals, and only the overall results of the studies were available. Three patients, 2 in the medically managed and 1 in the tracheotomy-dependent group, underwent single probe testing. One patient in the surgery group was accidentally given antireflux medication 24 hours before probe placement but was included in the study because the lower probe data remained abnormal. The upper probe was positioned to be at the level of the cricopharyngeus, and the lower probe was placed above the gastroesophageal junction. Probe placement was confirmed radiographically. No normative data were available for the pharyngeal probe. The criteria used by our pediatric gastroenterologists for a positive esophageal probe are as follows: 15% of probe time less than pH 4, reflux episodes greater than 5 minutes in duration, or more than 2 episodes of reflux per hour of probe time.
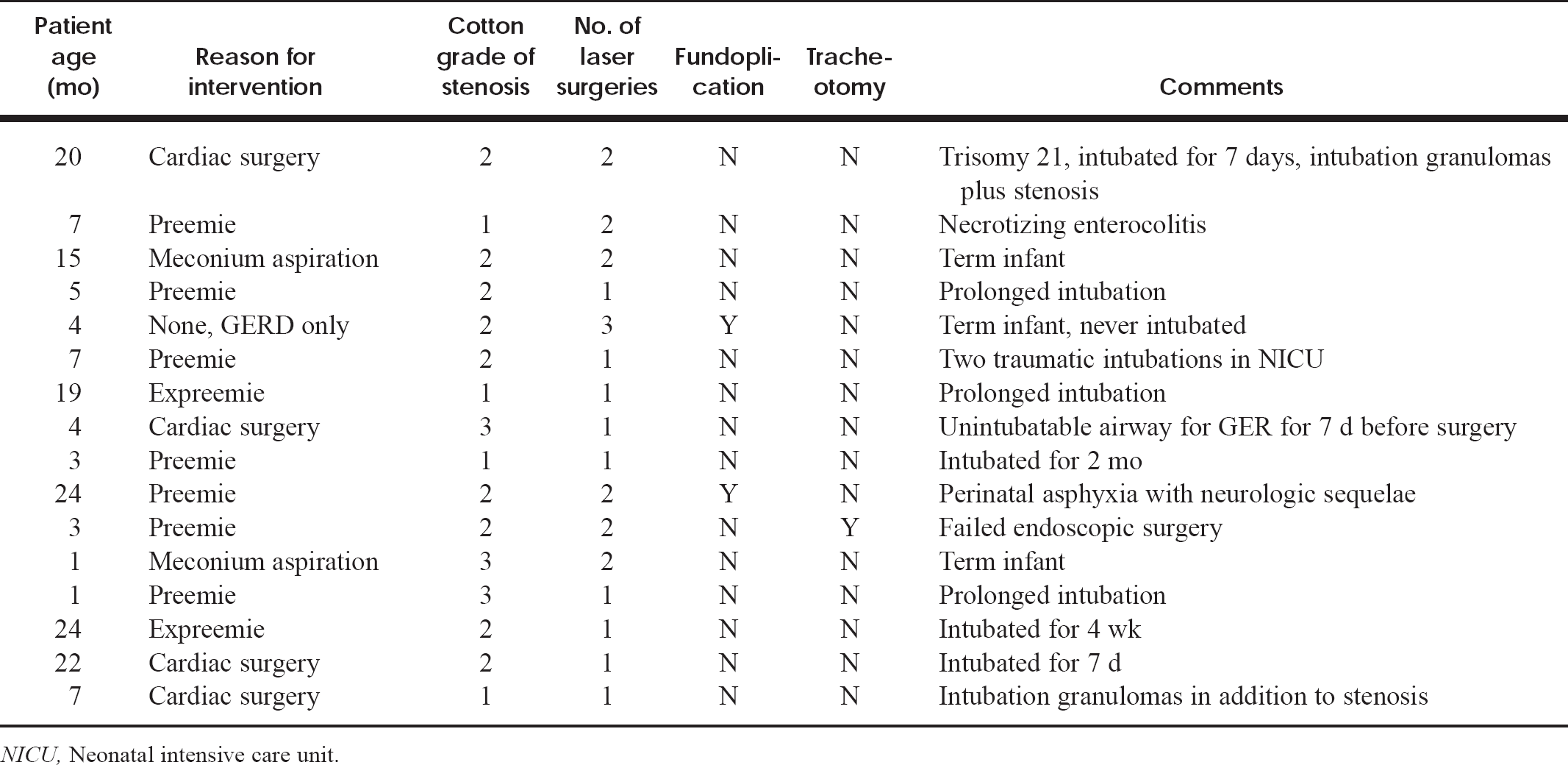
Surgical group
NICU, Neonatal intensive care unit.
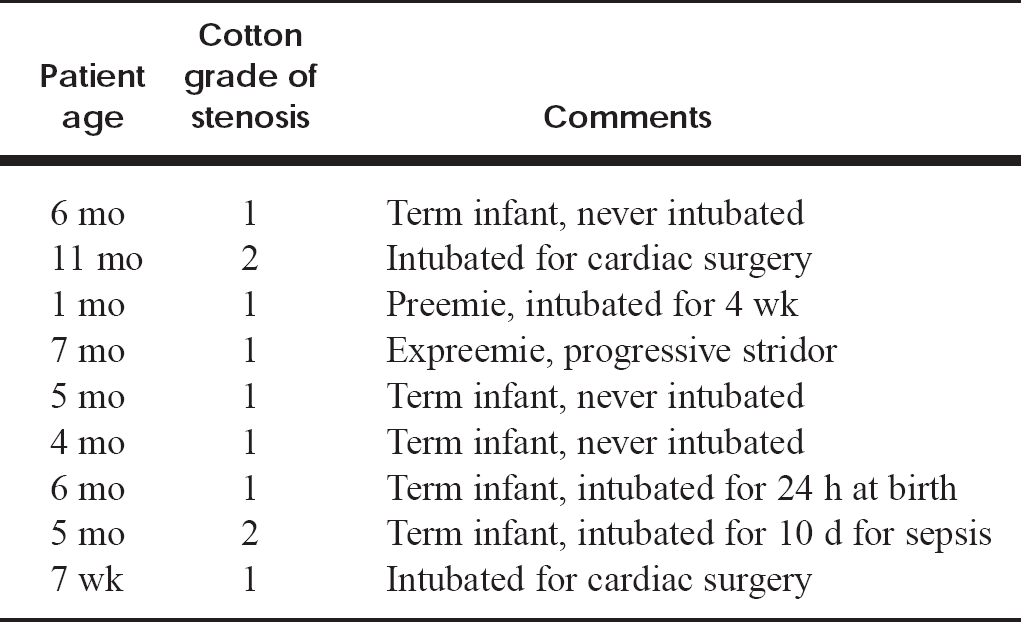
Antireflux medication only group
Suspension microlaryngoscopy with laser excision of stenosis by microflaps or radial incisions was performed in most patients. The details of the surgical repair are outside the scope of this article. Two tracheotomy-dependent patients underwent laryngotracheoplasty as part of their treatment. All stenoses were graded according to the Cotton classification. 4 Children who were treated medically had their stenoses graded on the basis of the appearance on flexible laryngoscopy.
All patients were treated with high-dose omeprazole (Prilosec), 5 to 10 mg twice daily sprinkled on applesauce, unless they could not eat from a spoon. Ranitidine (Zantac) 4 to 6 mg/kg/dose twice daily was substituted for these patients. In very refractory cases, 15 to 20 mg of Omeprazole twice daily or 4 to 6 mg/kg/dose 3 times/day of ranitidine was used. Cisapride (Propulsid) 0.2 mg/kg/dose every 6 hours in infants and at meals and before bedtime in older children was used in conjunction with the antacid medication. Fundoplication was recommended for patients who continued to have very positive probes despite high doses of antireflux medication.
RESULTS
Of the 25 children who were pH probed and treated for GER before undergoing any surgical intervention, 16 underwent endoscopic management of their SGS. Each had 1 to 3 surgeries, with endoscopic management failing in only 1 patient, who required tracheotomy. This represents a decrease in the number of patients in whom endoscopic repair failed from 1 in 5.7 patients to 1 in 25 patients. Table 1 describes their ages, presentation, grade of stenosis, and number of surgeries. Fourteen of these 16 patients' GER responded to antireflux medication alone. Two patients required fundoplication. The patients in whom stenoses developed after intubation for cardiac surgery required fewer surgeries and had GER that was easier to control than that of the rest of the group, implying that their GER may be caused by perioperative stress. Nine patients (Table 2) were treated with antireflux medication alone. Prior steroidal treatment, often in conjunction with antibiotics, had failed in these patients. Their stenoses were visualized by flexible laryngoscopy. Most were transferred from other hospitals with radiographs confirming the diagnosis. Four patients, 1 in the surgery group and 3 in the medically treated group, had never been intubated, implying that pathologic GER alone was the cause of their airway stenosis.
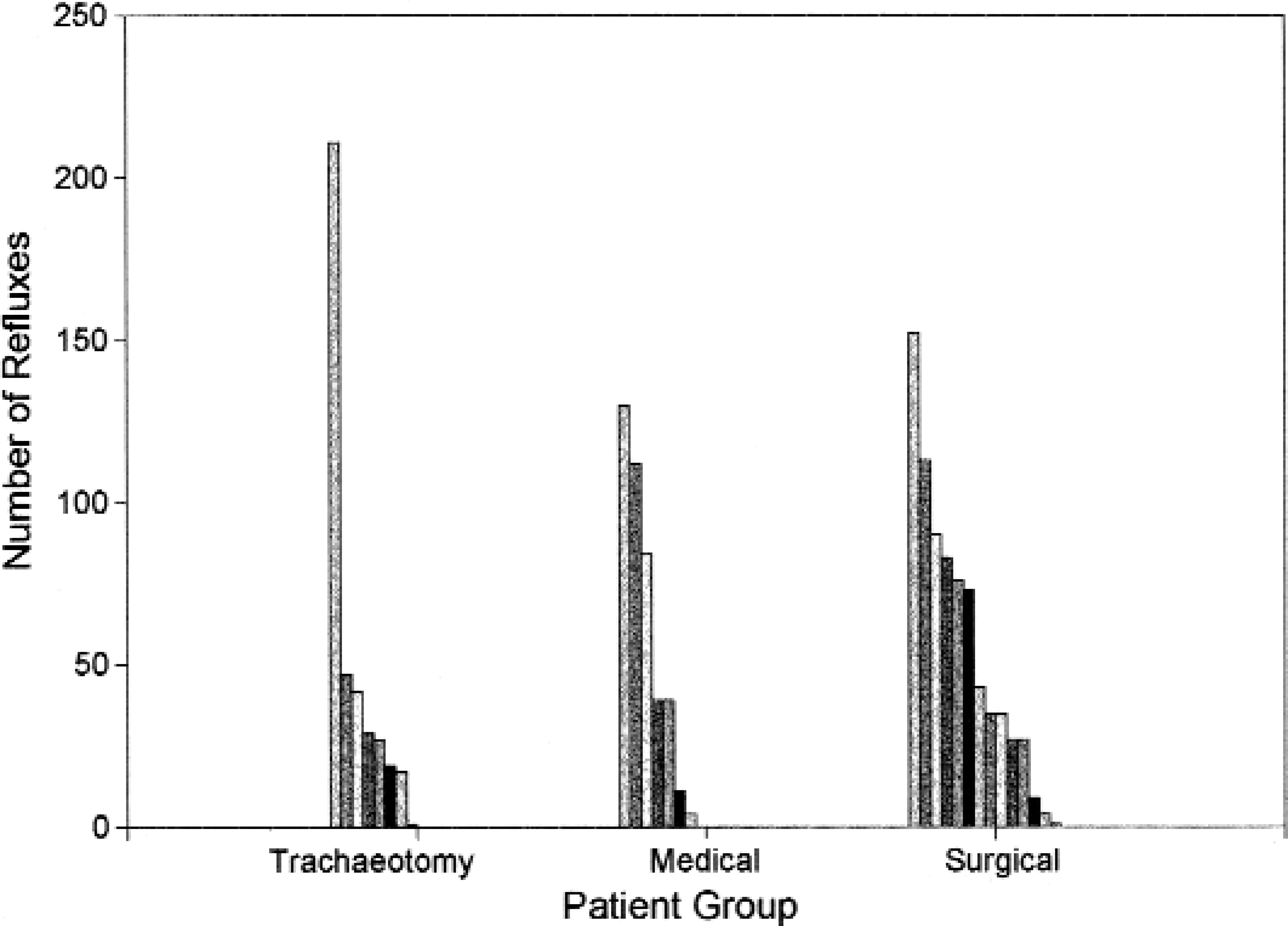
Pharyngeal pH probe data.
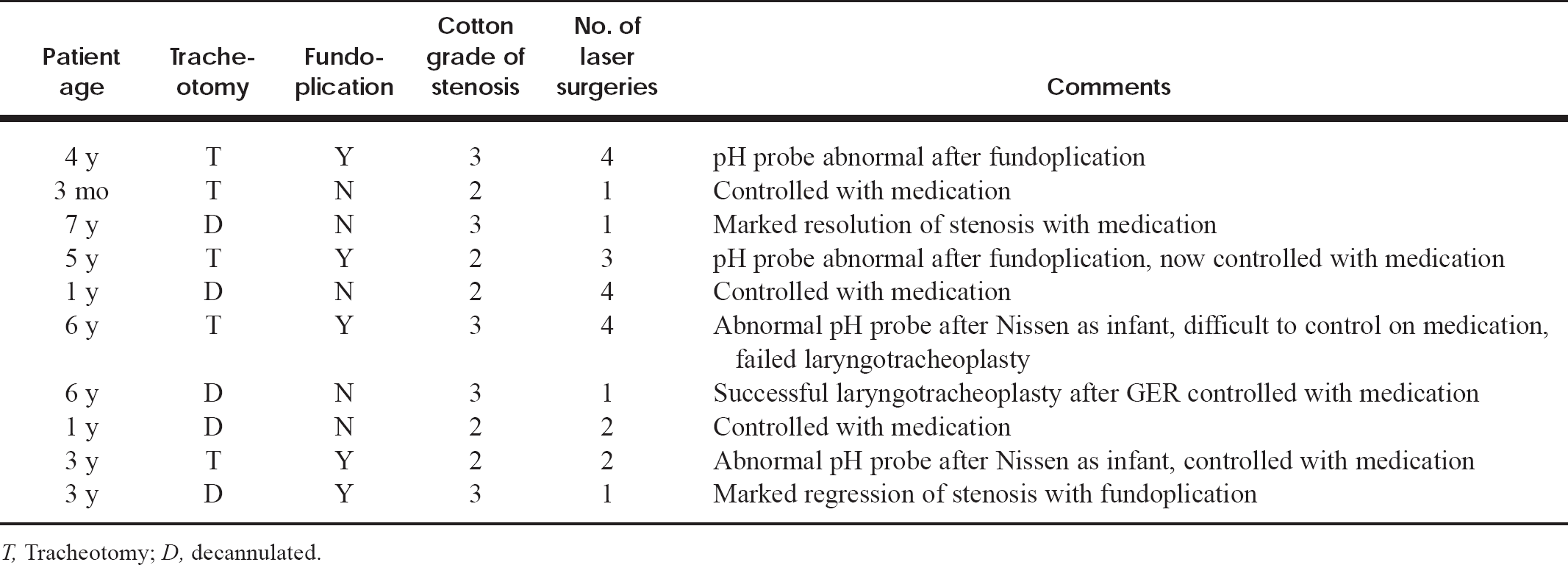
Tracheotomy-dependent group
T, Tracheotomy; D, decannulated.
The 10 patients who underwent pH probing and aggressive reflux management after tracheotomy are shown in Table 3. Nine of 10 were premature infants. One child underwent tracheotomy after failure of upper airway surgery for morbid obesity and congestive heart failure. Five patients have been decannulated. Three of 5 were decannulated after medical management of their GER and endoscopic surgery. One patient taking antireflux medications required laryngotracheoplasty and endoscopic surgery for decannulation. The fifth patient demonstrated marked regression of his SGS after fundoplication and required only 1 surgery for decannulation. Four patients had fundoplications to aid in the control of their GER. Three of the 4 still have positive pH probes, although greatly improved. Endoscopically, they continue to have very erythematous and edematous larynges.
The results of pH probe testing are shown in Figs 1 through 4. The number of pharyngeal refluxes ranged from 0 to 211 (Fig 1). There appeared to be no correlation with the number of refluxes and the patient's response to antireflux medication. The patient in the surgery group with only 1 pharyngeal reflux and 351 esophageal refluxes was the patient who required tracheotomy. Also, the patients in the tracheotomy-dependent group had fewer total numbers of refluxes in the pharyngeal probe but were very difficult to suppress medically (Fig 2). Patients older than 1 year were considered to have positive pharyngeal probes if they had 1 or more episodes of pharyngeal reflux because data exist showing that their reflux patterns should be the same as those of adults. 5,6 For children younger than 1 year, 4 to 5 pharyngeal refluxes were considered positive. The esophageal probe data were positive in 8 of 9 patients treated with medication only, 9 of 10 patients in the tracheotomy-dependent group, and 15 of 16 in the surgery group, by the criteria used by our pediatric gastroenterologists. The total number of refluxes did not vary significantly between the groups (Figs 3 and 4). Only 1 patient had a borderline probe. This patient, who was treated medically, had 4 pharyngeal refluxes and 13 esophageal refluxes with no episodes of reflux longer than 5 minutes. Steroid therapy failed; she was given antireflux medications before surgery and became asymptomatic.
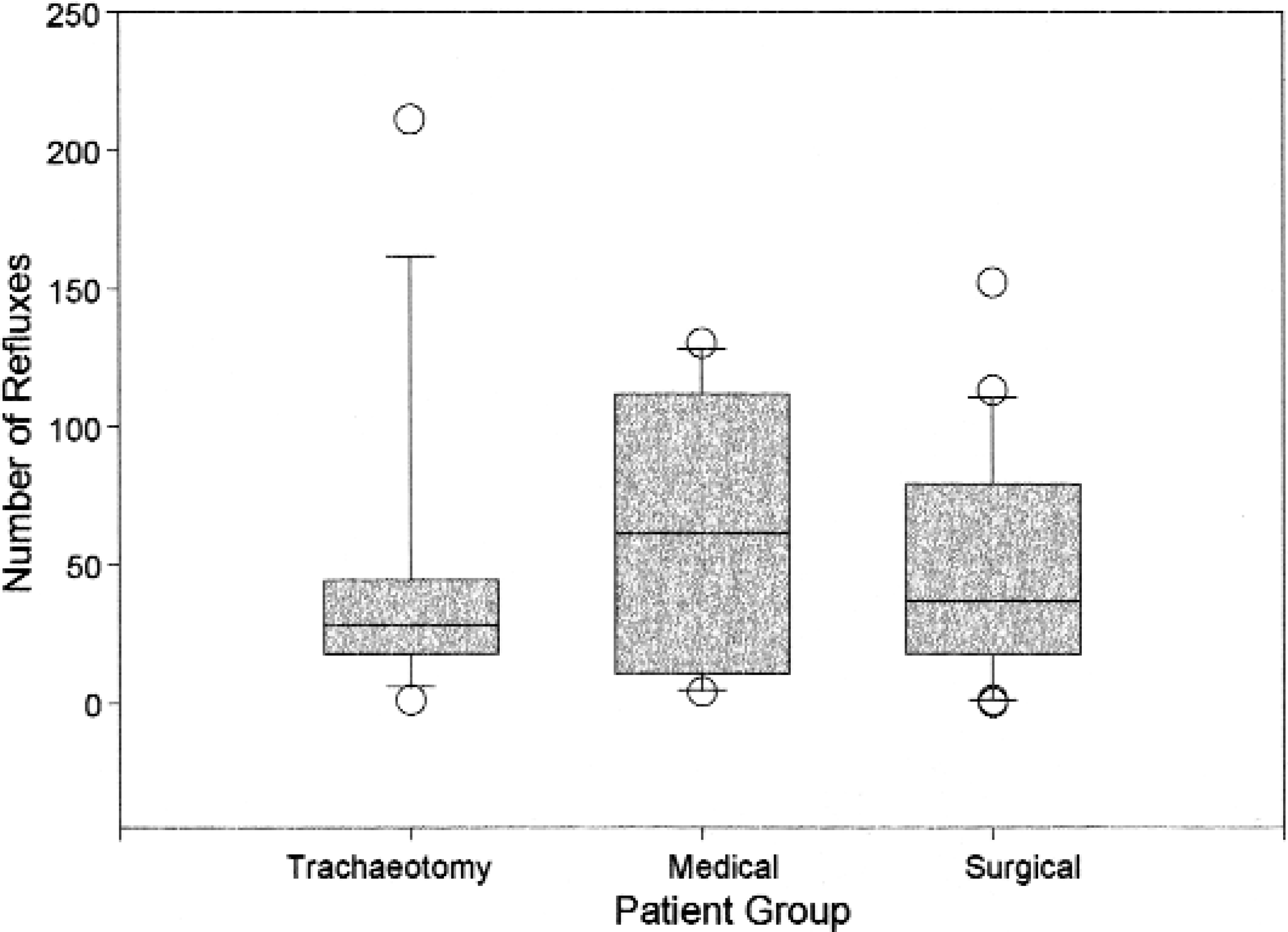
Box plot of pharyngeal pH probe data.
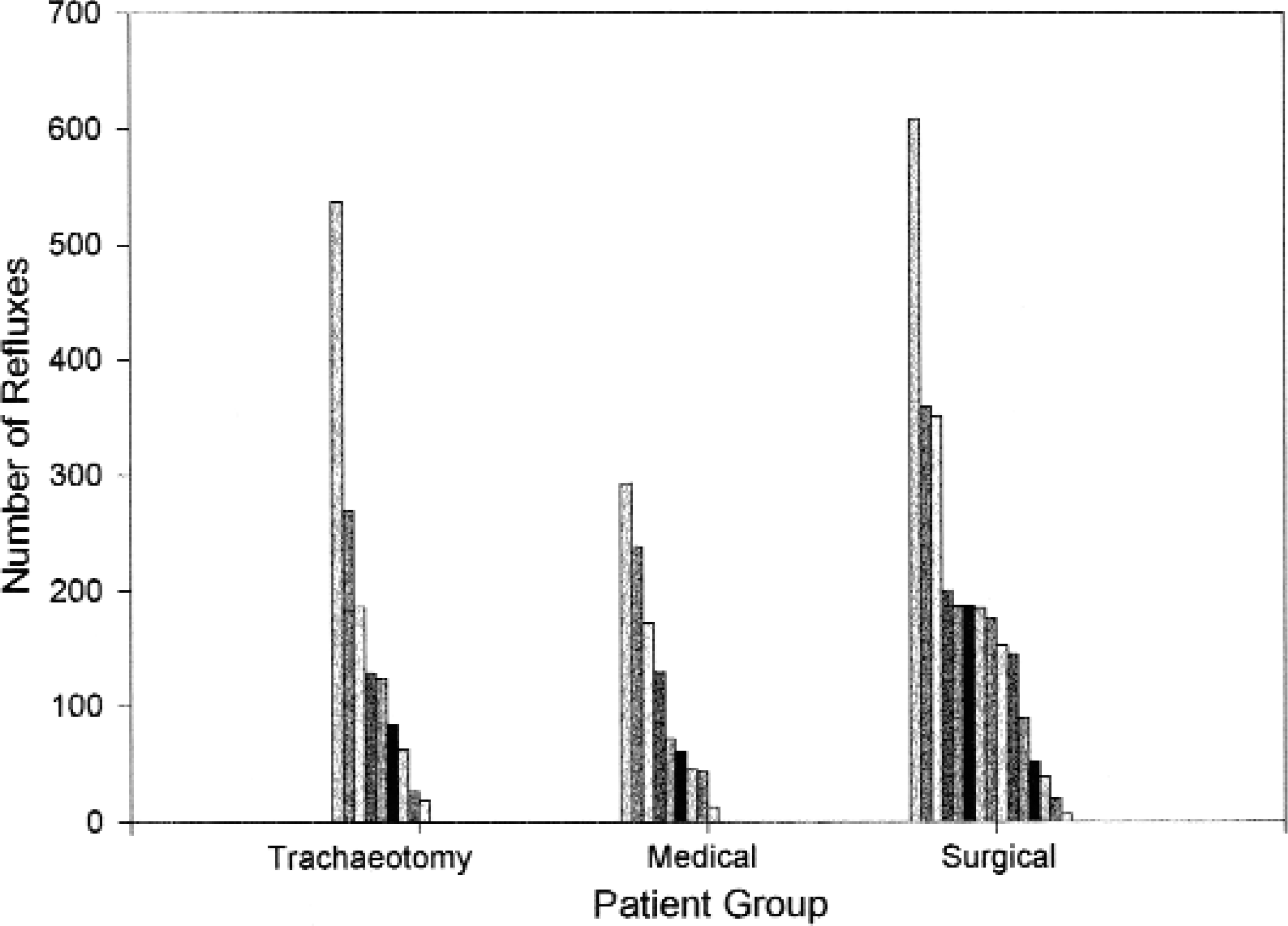
Esophageal pH probe data.
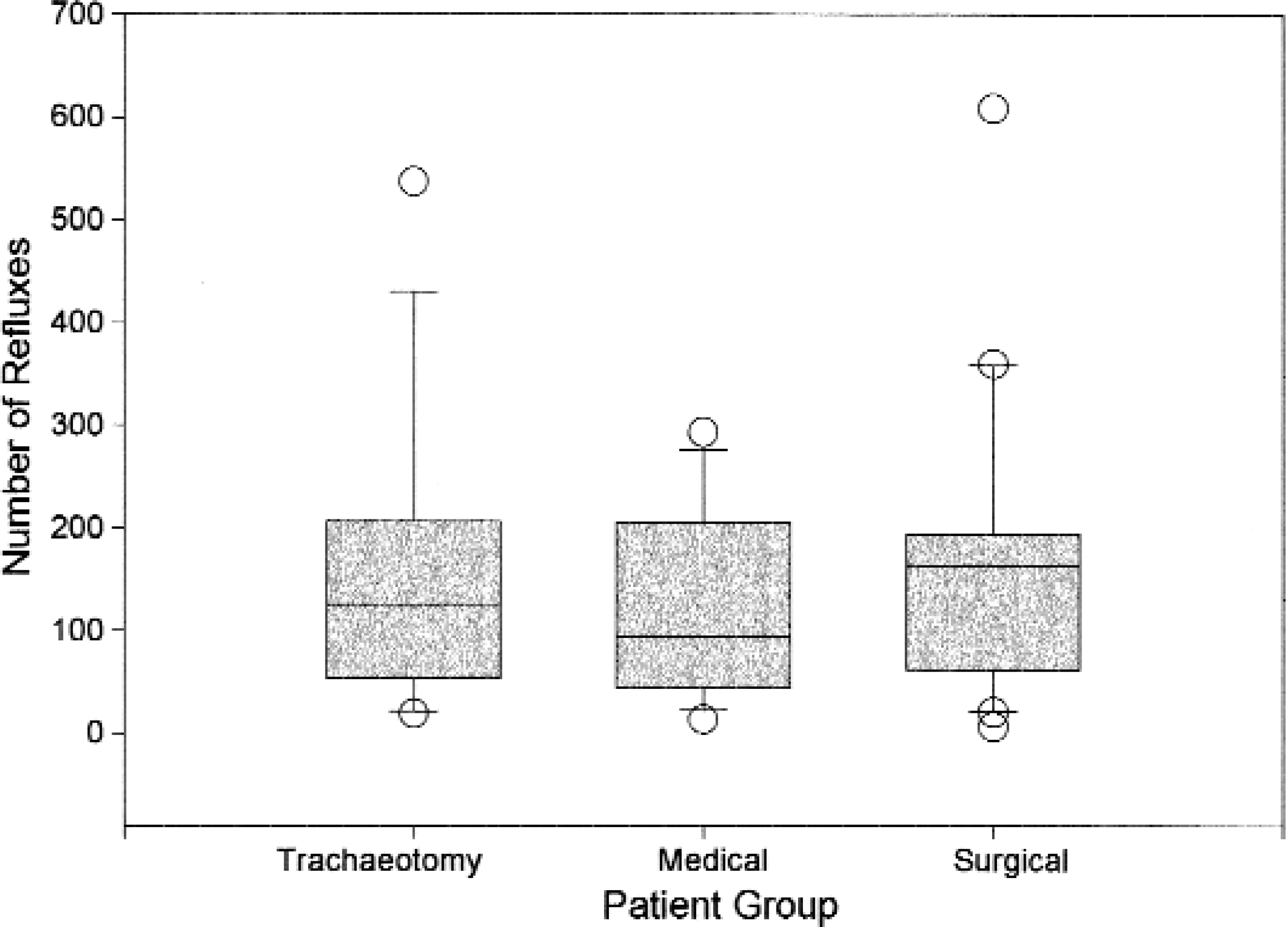
Box plot of esophageal pH probe data.
DISCUSSION
This study confirms the importance of diagnosing and aggressively treating GER for as long as possible before surgical intervention. With aggressive management, the number of patients in whom endoscopic repair failed went from 1 in 5.7 to 1 in 25. Additionally, 9 of 26 (35%) avoided surgery. By eliminating gastric acid and allowing the inflammation to resolve as much as possible with medical treatment, any reversible component of the stenosis will regress and the fixed scar that remains will not be bathed in acid, allowing further granulation tissue to develop after surgery. It seems that many of our medically treated patients did well because they remained uninstrumented and their stenoses were allowed to resolve. All of these patients had been given steroids, which are refluxogenic, and surgery without acid suppression would have undoubtedly created fixed scarring and granulation tissue similar to that in the case described by Burton et al. 3 Treating these patients medically can be stressful for the surgeon because, initially, they all have moderate respiratory distress. The dramatic increase in success of endoscopic management supports the observations of Gray et al 2 as to the importance of controlling GER regardless of the method chosen for repair of the stenosis. Endoscopic repair is chosen initially at this institution for its ability to preserve voice. The difficulty in achieving good control of GER in tracheotomy-dependent children who were born prematurely and their overall poor outcomes—increased number of endoscopic procedures, less satisfactory surgical results, and necessity of fundoplication—indicate that GER can persist in pathologic form for years and that it cannot be assumed that the infants with a history of prematurity plus SGS will outgrow their reflux. Review of the clinical courses and pH probe data of these patients does not yield any indicators that might be predictive of poor response to reflux therapy and surgery. Future investigations may reveal them.
The importance of the pharyngeal probe in ascertaining the presence of pathologic GER has been described by Koufman 6 and Little et al. 7 In their studies the diagnosis of GER would have been missed in at least 33% of their patients by single-channel probing because their esophageal probe data were normal by the criteria used at their institution. The criteria for a positive esophageal probe are much broader at this institution, which accounts for the fact that virtually all the pH probes were positive in both channels, with the exception of 1 probe study mentioned above. The pharyngeal probe data are also important because they monitor the response to antireflux medication. Typically, a repeat probe in a well-suppressed patient will show no refluxes in the pharyngeal probe or several episodes of reflux, each lasting 1 or 2 seconds, so that the total time below pH 4 in the pharyngeal probe is zero.
At this time, no normative data exist for the pharyngeal probe in children. Vandenplas et al 8 placed singlechannel pH probes in 509 healthy infants as part of a screening program for sudden infant death syndrome. They found that the reflux pattern in children older than 12 months resembled that of adults. Infants younger than 12 months had increased episodes of reflux. Previous double pH probe data on children with upper airway problems at this institution suggested that 10 or fewer episodes of reflux may be normal in the pharyngeal probe for infants younger than 1 year. 9 This figure was based on the finding of 10 or more episodes of reflux in the pharyngeal probe in all patients and on the premise that infants reflux each time they posset and burp. This may not be the case. We have observed that several neonates with apnea/bradycardia have had no episodes of reflux in their upper probes; however, all these infants would posset after eating. Their apnea/bradycardia appeared to be caused by stimulation of lower esophageal chemoreceptors as described by Bauman et al. 10 Thus the pathologic number of pharyngeal refluxes in infants younger than 12 months could be quite low, even 4 or fewer, as seen in the single child with a seemingly normal probe study and the child with only 1 pharyngeal reflux who required tracheotomy.
Initial management of GER can be done conservatively with positioning and dietary modifications as described by Burton et al 3 and Hanson et al 11 or aggressively as described by Little et al 7 and Koufman. 6 It is the practice at this institution to begin treatment with high-dose antireflux medication, omeprazole, because our patients are in respiratory distress. Eventually treatment is tapered to H2 blockers or behavioral management after the airway has been treated.
CONCLUSION
Aggressive treatment of GER in infants and children before surgical intervention significantly improved their clinical outcome. The number of patients in whom endoscopic repair failed dropped dramatically. Thirty-five percent avoided surgical intervention, and those requiring surgery required fewer procedures. pH probe testing, although not predictive of those children in whom endoscopic surgery would fail, was essential to the antireflux treatment of these patients. It demonstrates that in certain cases, such as cardiac surgery, reflux may be caused by perioperative stress and that GER may persist unabated for years in certain premature infants with SGS.