
Abstract

The cornerstone of diagnosis of squamous cell carcinoma (SCC) of the larynx is direct laryngoscopy with the patient under general anaesthesia, which allows biopsy of the mucosal lesion. This procedure also allows tumour staging according to American Joint Committee on Cancer guidelines. 1 A small proportion of laryngeal SCCs are submucosal with no mucosal abnormality present. This leads to difficulties in both diagnosis and staging. The first reported case of primary subglottic submucosal SCC is presented.
CASE REPORT
A 46-year-old unemployed man presented with a 2-month history of hoarseness. He smoked 40 cigarettes a day and drank more than 30 units of alcohol per week. There was no other history of note.
On examination the oral cavity and oropharynx were normal. Indirect laryngoscopy and nasoendoscopy were not possible because of an overhanging epiglottis and a sensitive gag reflex. He underwent microlaryngoscopy while under general anaesthesia. He had minimal Reinke's edema of both vocal cords, but thorough examination of the supraglottis and subglottis revealed no abnormality. Postoperative speech therapy and outpatient follow-up were arranged, but the patient failed to attend.
Six months later the patient returned in extremis with marked stridor and laryngeal pain. CT with intravenous contrast demonstrated a large subglottic mass almost occluding the airway (Fig 1A). No lymphadenopathy was seen. However, invasion of the right side of the thyroid cartilage was shown.
The patient was given a local anesthetic and underwent urgent tracheostomy to secure the airway. Rigid endoscopy with the patient under general anesthesia revealed a large, smooth mass in the right subglottis with no mucosal ulceration. Frozen-section histology of a deep biopsy confirmed SCC; therefore a total laryngectomy was performed.
Examination of the laryngectomy specimen showed a large subglottic SCC that was entirely submucosal; this finding was confirmed on histologic analysis (Fig 1B). Histologic analysis also confirmed invasion of the right thyroid cartilage. There was no dysplasia in the epithelium overlying the tumor. The tumor was therefore staged as T4N0M0, with a staging at first presentation of T0N0M0.
The patient underwent a course of radiotherapy after surgery and remains disease free 6 years after his surgery.
DISCUSSION
Subglottic SCC of the larynx is an uncommon disease representing less than 5% of all laryngeal malignancies. 2 It often presents as an annular mass causing stridor. It is also associated with a high incidence of metastases to neck nodes at presentation (20%). 2
Review of the literature suggests that this is the first report of a submucosal subglottic SCC. There have been a number of reports of laryngeal submucosal SCC, but these have all arisen in the supraglottis (24 cases in total). 3–8 Submucosal SCC has also been documented at other sites in the upper aerodigestive tract, including the nasopharynx, tongue base, and tonsil. 6
It is not clear how submucosal SCC arises, and theories include the involution of small mucosal tumors 6 and origin in the ducts of minor salivary glands. 3 The occurrence of submucosal tumors may also explain presentation with metastases in neck nodes and an occult primary tumor. 6
Diagnosis of laryngeal submucosal SCC may be delayed for a significant length of time despite direct laryngoscopy. This delay has been as long as 24 months from first laryngoscopy for symptoms suggestive of malignancy that were eventually diagnosed as supra-glottic SCC. 3,4 In the case presented, the delay from presentation to diagnosis was 6 months, during which time there was considerable tumor growth, with the T stage progressing from T0 to T4 and necessitating emergency laryngectomy on second presentation.
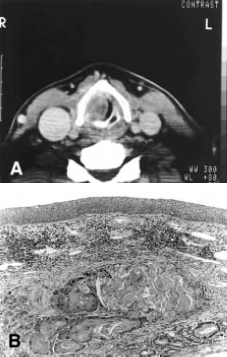
A, Axial CT scan with intravenous contrast at the level of the junction of the glottis and subglottis, showing large right-sided subglottic mass. B, Histologic sectioning demonstrating SCC beneath intact stratified squamous epithelium. (Hematoxylin and eosin stain, original magnification x40.)
Failure of diagnosis occurs because no lesion is seen or because biopsy fails to include malignant tissue. When suspicion of malignancy persists despite normal laryngoscopy and biopsy, CT or MRI may delineate submucosal lesions. CT is useful in aiding diagnosis in the presence of submucosal SCC of the supraglottis. 3,4 In particular, CT demonstrates abnormalities when laryngoscopy is normal and guides deep or wedge biopsy of these lesions. MRI is probably at least as good at demonstrating submucosal lesions, but no studies regarding this have been reported. When tumor is apparent at laryngoscopy, CT or MRI in combination with clinical and direct laryngoscopic examination significantly improves the accuracy of laryngeal tumor staging when compared with clinical and direct laryngoscopic staging only. 9,10 This would suggest that CT and MRI are probably the most important investigational tools when suspicions of a laryngeal malignancy persist despite normal direct laryngoscopy or biopsy. Zbären et al 9 believed that both CT and MRI are particularly useful in demonstrating submucosal extension into the subglottis of primarily glottic tumors because the main tumor mass tends to obscure direct laryngoscopic assessment of the subglottis. CT can demonstrate laryngeal cartilage invasion, although this is not always reliable because there may be variable calcification of the laryngeal cartilages. 10,11 CT detection of cartilaginous invasion is improved by taking fine cuts, but overall, CT tends to underestimate cartilaginous invasion. 9 Saleh et al 12 have recommended routine CT of subglottic tumors because this area is difficult to assess at direct laryngoscopy and there is frequently relatively minimal mucosal evidence of extensive deep tumor volume. MRI tends to overestimate tumor extent because it is particularly sensitive in demonstrating edema and fibrosis associated with the margins of the tumor. 9
Therefore, when the index of suspicion of malignancy of the larynx is high but no lesion is seen on laryngoscopy, CT or MRI assists in confirming the presence of a lesion and guiding the positioning of subsequent biopsies. We have found that the use of Hopkins rod endoscopes at direct laryngoscopy is useful in assessing the subglottis more closely.
We are grateful to Mr R. Tranter for allowing us to present this case.