
Abstract
Adherent bacterial biofilms have been implicated in the irreversible contamination of implanted medical devices. We evaluated the resistance of various tympanostomy (pressure equalization [PE]) tube materials to biofilm formation using an in vivo model. PE tubes of silicone, silver oxide-impregnated silicone, fluoroplastic, silver oxide-impregnated fluoroplastic, and ion-bombarded silicone were inserted into the tympanic membranes of 18 Hartley guinea pigs. Staphylococcus aureus was then inoculated into the middle ears. An additional 8 guinea pigs were used as controls; the PE tubes were inserted without middle ear inoculation. All PE tubes were removed on day 10 and analyzed for bacterial contamination using culture, immunofluorescence, and scanning electron microscopy (SEM). All infected ears developed otitis media with otorrhea, but none of the animal control ears drained. Fluorescence imaging of the animal control tubes showed large cellular components consistent with inflammation. The infected tubes showed heavy DNA fluorescence consistent with bacteria and inflammatory cells. All animal control tubes except the ion-bombarded silicone tubes showed adherent inflammatory film on SEM. Also, all tubes placed in infected ears except the ion-bombarded silicone tubes showed adherent bacterial and inflammatory films on SEM. Nonadherent surface properties such as the ion-bombarded silicone may be helpful in preventing chronic PE tube contamination.
Adherent bacterial biofilms have been implicated in the irreversible contamination of implanted devices such as vascular catheters, artificial joints, urinary catheters, and scleral buckling elements. 1–4 Bacteria that grows on material in vivo in the form of a biofilm are coated in a slime of hydrated bacterial exopolymers and macromolecules. 5 This organization renders the bacteria relatively resistant to antibiotics and contributes to the development of persistent infections. 4,6
Otitis media with effusion in the presence of pressure equalization (PE) tubes can be persistent and recalcitrant to therapy. PE tubes act as a foreign body that may harbor bacteria once contaminated. An ideal PE tube material would be one that is well tolerated and resists bacterial adhesion. The tube-surface properties may play an important role in resisting bacterial colonization and biofilm formation. We evaluated the resistance of various PE tube materials to biofilm formation using an in vivo model in guinea pigs.
METHODS
The 5 types of PE tube tested were (1) silicone (Armstrong; Smith & Nephew, Bartlett, TN), (2) silver oxide-impregnated silicone (Armstrong-Activent; Xomed, Jacksonville, FL), (3) fluoroplastic (Armstrong; Smith & Nephew), (4) silver oxide-impregnated fluoroplastic (Straight Shank-Activent; Xomed), and (5) ion-bombarded silicone (T-tube-Ultrasil; Smith & Nephew).
All animal experimentation was approved by the institutional review board on the use of animals and complied with the standards set by the NIH for the care and use of laboratory animals. Twenty-six Hartley guinea pigs weighing 450 to 500g were anesthetized with ketamine (100 mg/kg intramuscularly), and their external ear canals were cleaned with povidoneiodine (Betadine). With an operating microscope, myringotomy was performed, and a PE tube was inserted (10 from each tube type). At the time of tube insertion, the middle ears of experimental animals (18 guinea pigs, 7 tubes from each type in a randomized selection) were inoculated with 0.1 mL of >10 9 colony-forming units of a Staphylococcus aureus broth. The animal controls consisted of the 8 other guinea pigs in which PE tubes were inserted into the tympanic membranes (3 tubes of each type in a randomized selection) without inoculation. The experimental and control groups were housed separately. Staphylococcus was chosen because it is a common cause of chronic otitis media and can be easily visualized by scanning electron microscopy (SEM).
Example of red fluorescence seen on the animal control tubes showing weakly fluorescent large cellular forms characteristic of inflammatory cells.

Example of red fluorescence seen on the infected tubes. Both weakly fluorescent large cellular forms (characteristic of inflammatory cells) and smaller, denser fluorescent bodies (characteristic of bacteria) are present.
All experimental and control animals were examined for otorrhea on days 3 and 10. A swab was used to culture the external ear canal of each animal on day 10, and the PE tubes were removed and rinsed with 10 mL of sterile saline solution to remove any free planktonic bacteria. With a sterile technique, a section of each tube was cut and placed in a mixture of formaldehyde and gluteraldehyde in preparation of SEM. A second section was cut and placed in glutaraldehyde (0.5%) for immunofluorescent examination. The remaining section was swabbed on an agar medium for culture. Sections of sterile (straight from the box) PE tubes of each type, referred to as sterile controls, were also prepared for immunofluorescence and SEM.
Tube sections placed in glutaraldehyde for immunofluorescence scanning were rinsed with 10 mL sterile water and immersed in a commercial 2-color fluorescence nucleic acid stain for 15 minutes (LIVE/DEAD BacLight Bacterial Viability Kits; Molecular Probes, Eugene, OR). The commercially available BacLight system stains nucleic acids in bacteria with intact cell membranes fluorescent green, and it stains bacteria with damaged cell membranes fluorescent red. Fluorescence microscopy was used to observe green and red fluorescence of the nucleic acids on each tube surface with fluorescein and rhodamine optical filters, respectively. A representative image of each tube fluorescence was captured.
PE tube sections fixed in 4F1G were prepared for SEM. The surface of each tube was scanned, and representative images were recorded at magnifications of x200, x1000, and x4000. Attempts to illustrate individual bacteria with TEM were unsuccessful because of the soft PE tube material, which prevented adequate sectioning. Attempts at double embedding with a PolyBed 880 resin were also unsuccessful.
RESULTS
All experimental ears inoculated at the time of PE tube placement showed purulent drainage on days 3 and 10. None of the animal control ears (with PE tubes but without bacterial inoculation) had drainage. Cultures obtained of the external auditory canal and of the PE tubes in the experimental ears all grew heavy S aureus and Proteus vulgaris 48 hours after culturing. Cultures of the external auditory canals and PE tubes in control ears all had no growth or scant S aureus growth (<4 colonies/plate).
Fluorescence Microscopy
Immunofluorescence microscopy with the previously described BacLight system was used in an attempt to demonstrate bacterial adhesion on the tube materials. Green fluorescence (illuminated by fluorescein-filtered light) signifies cells with intact cell walls, whereas red fluorescence (illuminated by rhodamine filtered light) signifies damaged cell walls.
Unfortunately, fluorescence microscopy of the sterile control, animal control, and experimental PE tube materials illuminated with the fluorescein-filtered light all showed a large amount of green autofluorescence. Therefore the fluorescence seen on the animal control and experimental tubes was noninformative because of the heavy autofluorescence background. However, the sterile tubes did not have any red autofluorescence (when illuminated by the rhodamine-filtered light). Any red fluorescence seen on the animal control and experimental tubes was attributed to nucleic acids of inflammatory cells and bacteria.
On the animal control tubes, the red fluorescence was very sensitive to any nucleic acids present on the tube surfaces. All the animal control tubes showed some added fluorescence composed primarily of weakly fluorescent large cellular forms characteristic of inflammatory cells. There was no consistent difference in the fluorescence seen on the different tube surfaces. An example of this fluorescence is shown in Fig 1.
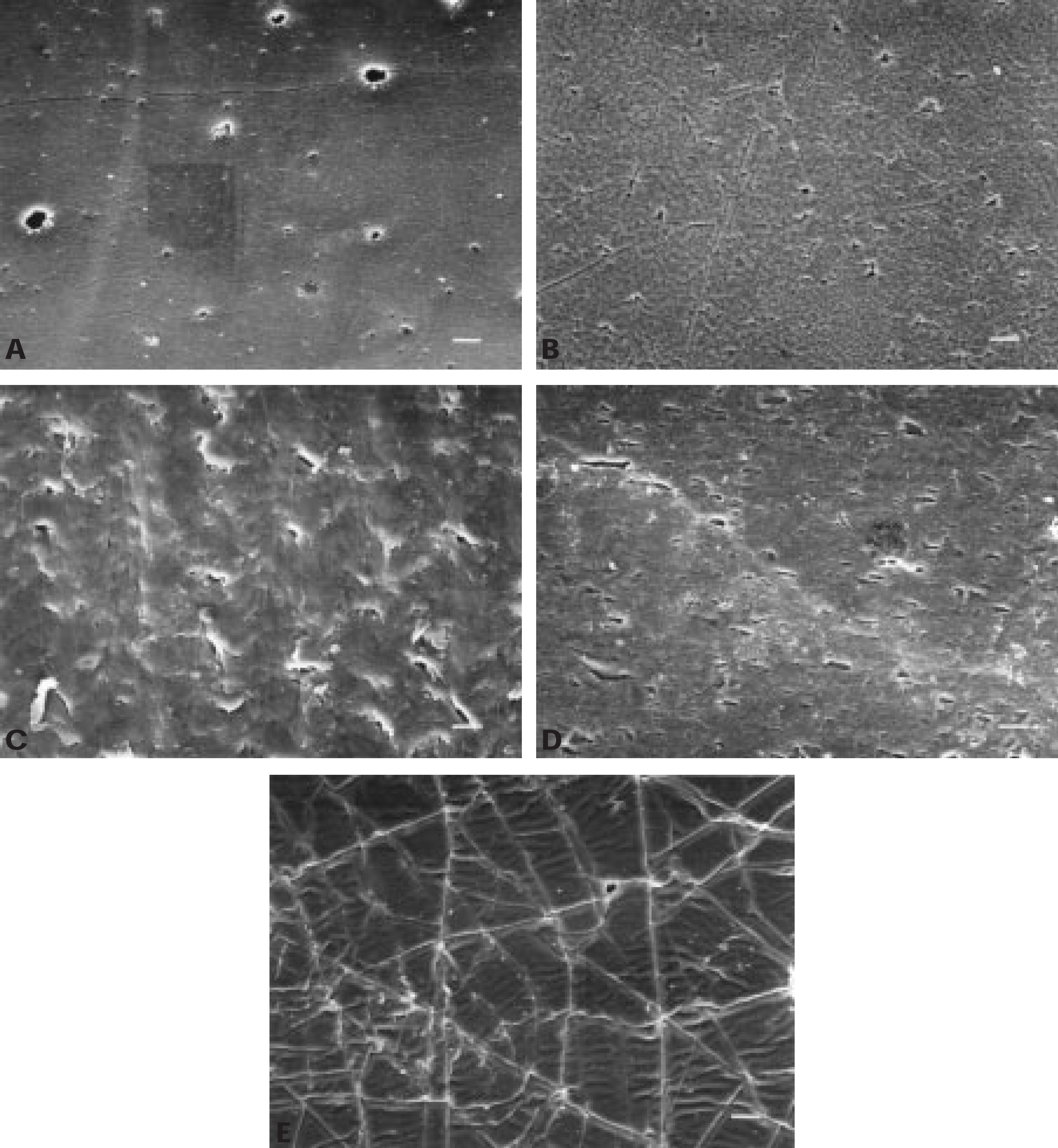
Representative SEM at x1000 magnification (bar = 10μm) of sterile silicone (A), silver oxide-impregnated silicone (B), fluoroplastic (C), silver oxide-impregnated fluoroplastic (D), and ion-bombarded silicone (E).
On the infected tubes, the fluorescence took 2 forms. The first involved large low-intensity fluorescence of inflammatory cells, similar to those of the animal control tubes. Additionally, there was also a high-intensity emittance from smaller, denser conglomerations of cellular components, characteristic of bacteria. The high sensitivity of nucleic acid fluorescence revealed a heavy concentration of nucleic acids on all tube types in the experimental group, but no consistent differences were realized between the different tube materials. Figure 2 shows an example of such a fluorescence image.
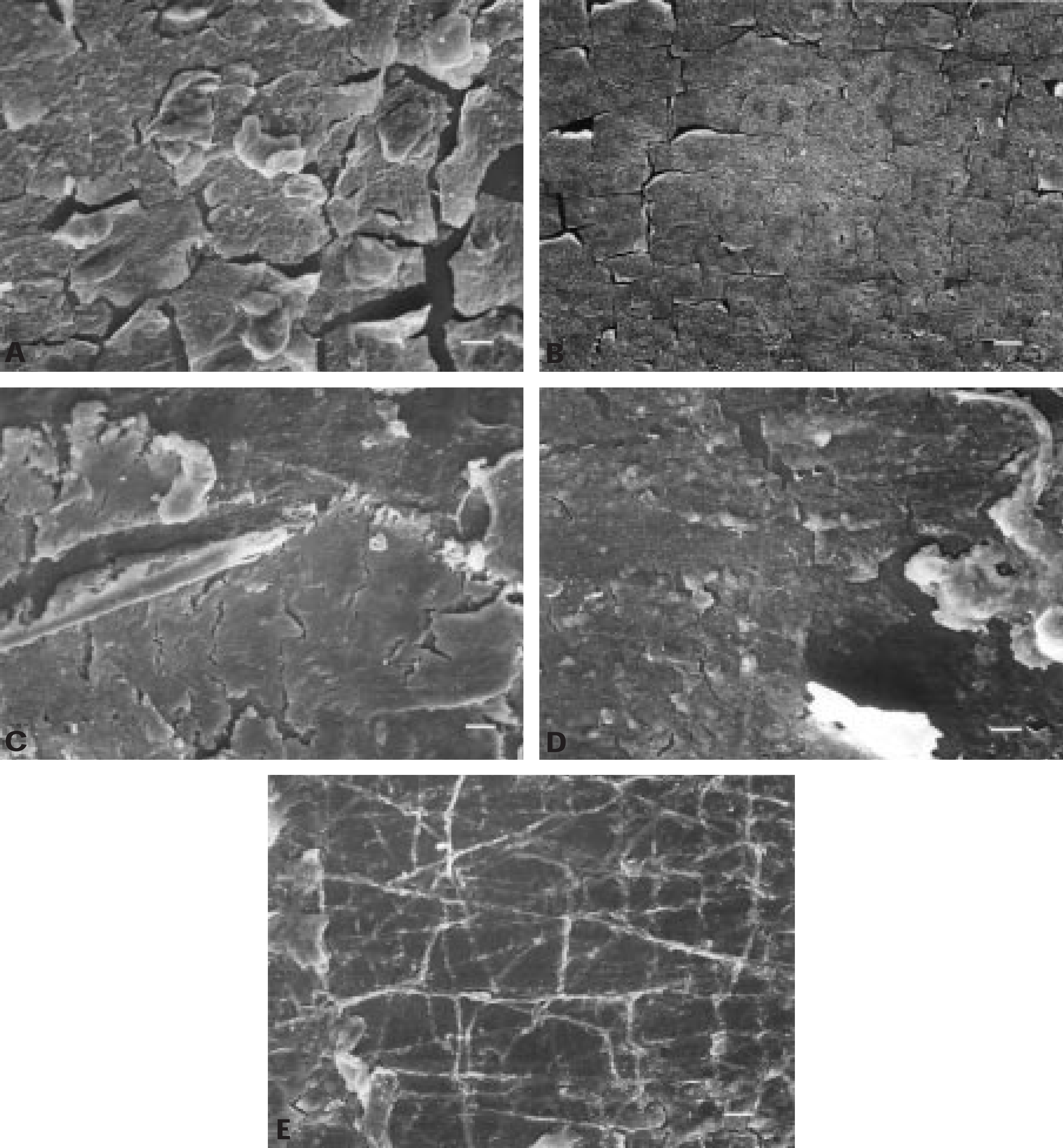
Representative SEM images at x1000 magnification (bar= 10μm) of the PE tubes retrieved from the animal control ears: silicone (A), silver oxide-impregnated silicone (B), fluoroplastic (C), silver oxide-impregnated fluoroplastic (D), and ion-bombarded silicone (E). A-D, Underlying tube material is unidentifiable as a result of the inflammatory film that appears adherent to the tube surface. E, Overall tube surface is clearly identifiable despite the cellular debris that is present in the crevices of the ion-bombarded tube.
The immunofluorescence microscopy was informative in revealing the presence of cellular nucleic acids on the tube surfaces. However, because of the autofluorescence signal and high sensitivity of the test, we were unable to show or quantitate the presence of biofilms on the tube surfaces with this method.
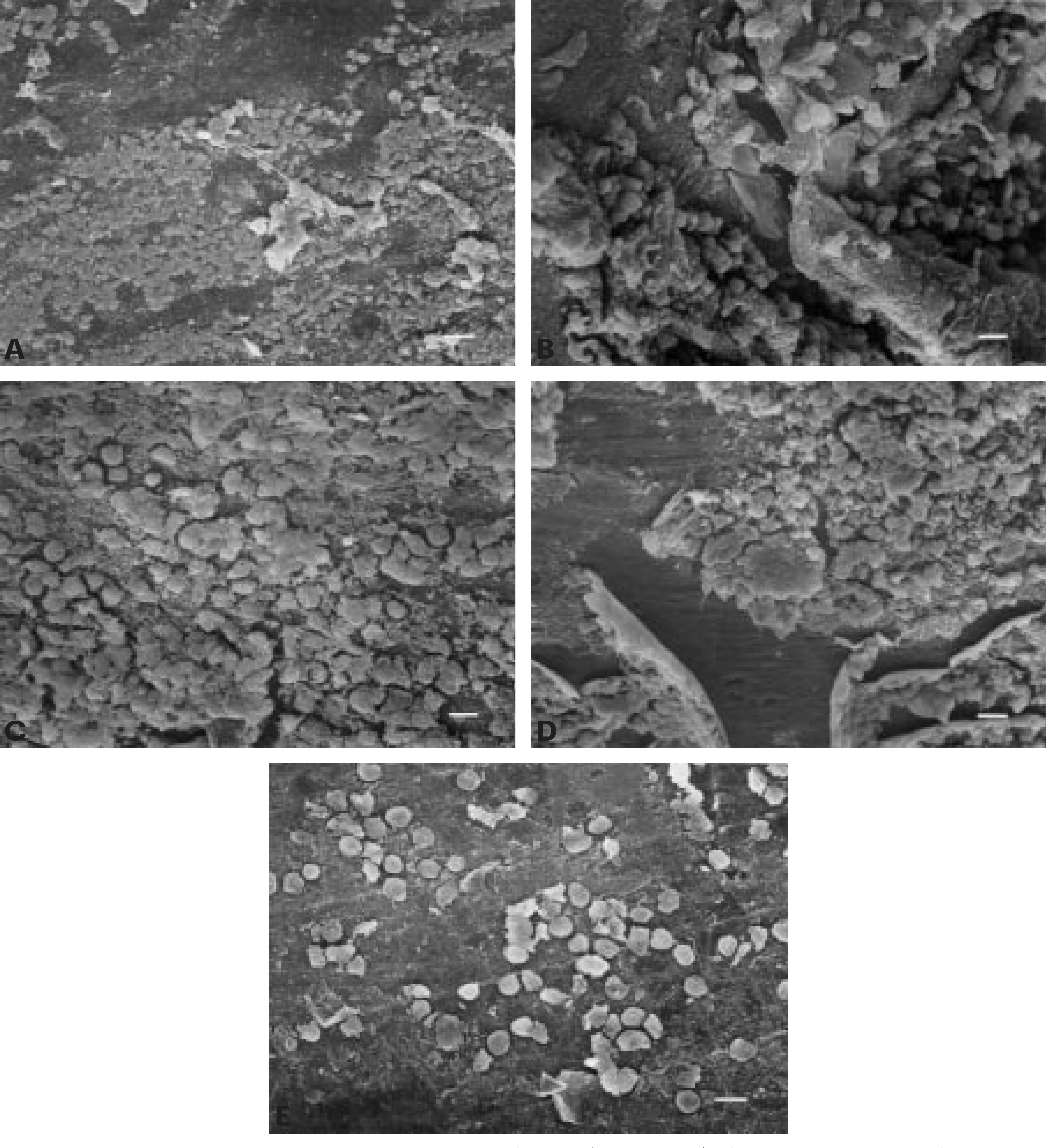
Representative SEM images at x1000 magnification (bar = 10μm) of the PE tubes retrieved from the ears of the infected group: silicone (A), silver oxide-impregnated silicone (B), fluoroplastic (C), silver oxide-impregnated fluoroplastic (D), and ion-bombarded silicone (E). A-D, A film is adherent to the surface on each tube type, and bacteria is superimposed over the film material. E, Ion-bombarded tube shows some isolated bacteria that were not congruent and did not meet the description of bacterial biofilms.
SEM
Each PE tube material had a characteristic SEM appearance. Figure 3 shows the SEM images of the sterile tubes at x1000 magnification. The SEM image of the surface of the sterile tubes was consistent across the entire tube. The surface of the silicone tube and the silver oxide-impregnated silicone tubes contained undulations or microfissures throughout (Fig 3A and B). The fluoroplastic tubes contained a systematic pattern of ridges that ran perpendicular to the tube shaft (Fig 3C). The silver oxide-impregnated fluoroplastic had pits widely distributed over the entire surface (Fig 3D). The silver oxide could be seen on the silver oxide-impregnated silicone and fluoroplastic tubes in the form of particles or pellets on the surface (Fig 3B and D). The ion-bombarded silicone resembled plates that adjoined in crevices (Fig 3E).
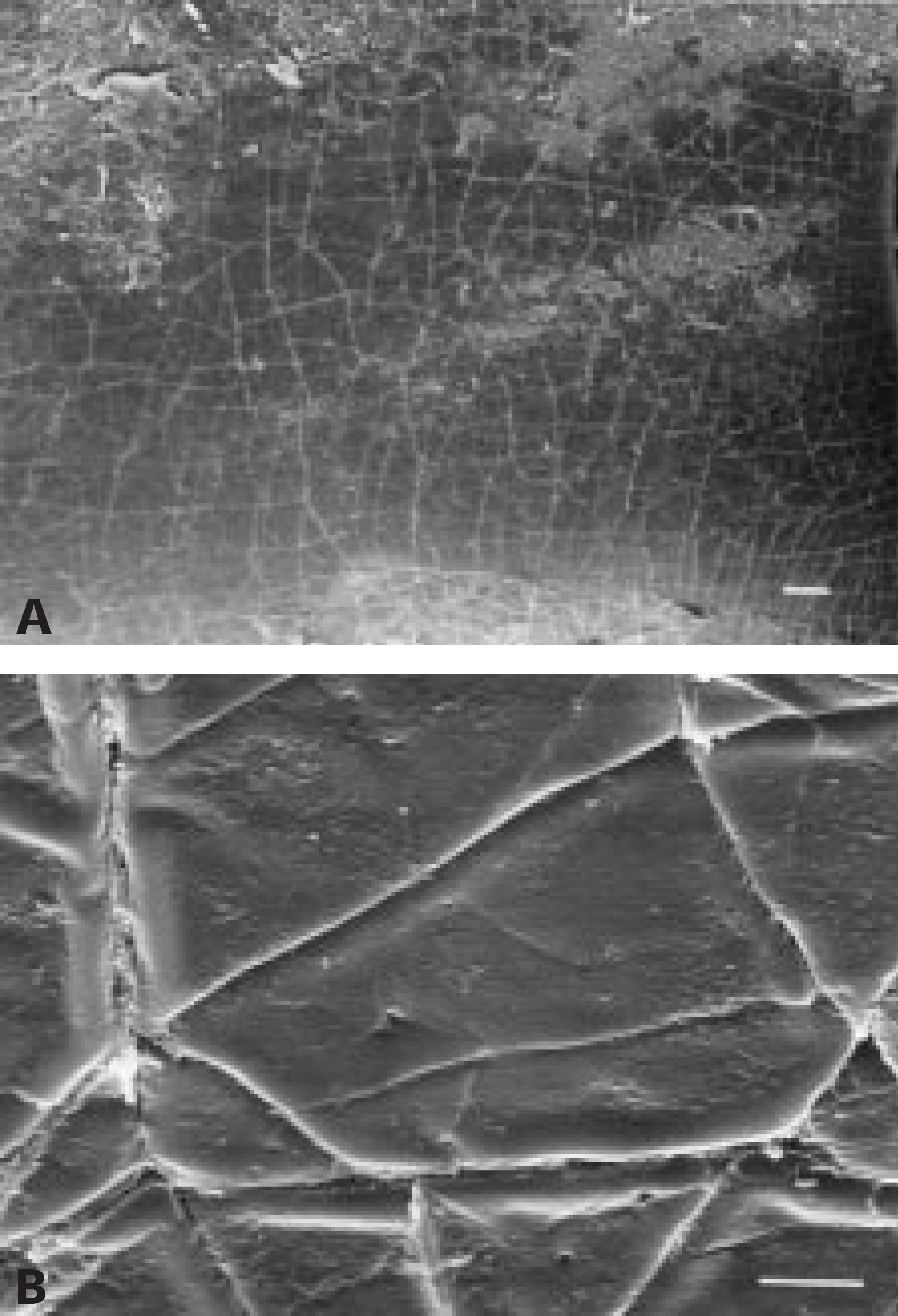
Representative x200 and x4000 magnification SEM of the infected ion-bombarded tube. A, Patch of inflammatory film is present on the bottom of the image, whereas the predominant tube surface areas are free of film and bacteria (bar = 50 μm). B, Some debris is seen in the crevices of the ion-bombarded silicone tube, whereas the surface is predominantly free of crust or bacteria (bar = 5 μm).
Representative SEM images at x1000 magnification of the PE tubes retrieved from the animal control ears are shown in Fig 4. A film is evident on the surface of all the tubes except for the ion-bombarded silicone tubes. Each of the tube surfaces, except the ion-implanted silicone photographed in Fig 4, were unidentifiable as a result of this inflammatory film. Also appreciated from these figures is the presence of a continuous film or exudate that appears to peel off of the tube surface at irregular breakpoints. The silver oxide particles were not visible on the exposed surfaces of these animal control tubes (Fig 4B and D). The plates that constitute the surface of the ion-bombarded silicone tubes appear to resist adherence of this inflammatory film (Fig 4E), with cellular debris adherent to the crevices between the plates.
Figure 5 shows the representative SEM images at x1000 magnification of the PE tubes retrieved from the ears of the infected group. A film is again adherent to the surface on each tube type except the ion-bombarded silicone tube. Bacteria are also seen superimposed over the film material. The images portrayed are typical of the findings found on all similar tubes from each group. The thick films present on most tube surfaces (Fig 5A-D) were dense conglomerations with no intervening spaces, consistent with biofilms. These were similar to biofilms previously identified by SEM in other studies. 3,4,7,8 Again, the concentration of silver oxide particles seen on the exposed surface of the tubes was markedly decreased compared with the sterile silver oxide-impregnated tubes (compare Fig 5B and D with Fig 3B and D). The ion-bombarded tubes showed a resistance to bacterial adhesion and biofilm formation (Fig 5E). Although the predominant pattern on the ion-bombarded tubes was relatively free of bacteria and inflammatory film, isolated bacteria were identified that were not congruent and did not meet the description of bacterial biofilms. The ion-bombarded tube is shown at magnifications of x200 and x4000 in Fig 6. On the low magnification a patch of inflammatory film is seen on the bottom of the image, whereas the predominant tube surface areas are seen to be free of film and bacteria. Figure 6B illustrates that although some debris is seen in the crevices of the ion-bombarded silicone tube, the surface is predominantly free of inflammatory film and bacteria.
DISCUSSION
The effect of implant material on susceptibility to bacterial and thrombus attachment has previously been studied. 9–12 Once a surface becomes contaminated, the susceptibility of bacterial biofilms to antibiotics is also markedly decreased compared with that of the planktonic forms of the same bacteria species. 6,13
Karlan et al 12,14 showed that different tube materials had different surface topographies by SEM examination. This difference was believed to be important in the tubes' differential susceptibilities to infections. In a clinical study Karlan et al compared silicone and fluoroplastic myringotomy tubes and found a significantly lower rate of infections in the fluoroplastic tubes. In addition to the surface structure, antibiotic impregnation of myringotomy tubes has been studied as a mechanism against infection. Silver coating of indwelling urinary catheters has been shown to reduce the incidence of bacteruria. 15,16 In an in vitro study, a hydrogel/silver-coated catheter was found to have reduced adherence of bacteria relative to silicone catheters. This was primarily because of the hydrogel hydrophilicity followed by secondary biocidal activity of the silver coating. 11 PE tubes impregnated with silver oxide are commercially available, and in a clinical study the incidence of otorrhea was noted to be decreased in the silver oxide-impregnated PE tubes compared with pure silicone. 17 In our study, when purposely infected with a large bacterial load, no tube was found to resist otorrhea. The relative importance of surface adherence properties versus antibacterial properties in preventing bacterial adherence and infection is unclear. The SEM images of the silver oxide-impregnated tubes retrieved from the animal control and infected ears (Fig 4B and D and Fig 5B and D) suggest that the silver oxide particles may dissolve into solution, leaving behind the basic tube material.
Recently, in an in vitro study Biedlingmaier et al 10 showed the development of bacterial biofilms on PE tubes composed of silicone, fluoroplastic, and silver oxide-impregnated silicone. In that in vitro study and in the present in vivo study, the ion-bombarded silicone appeared to resist bacterial adherence. The present study determined that this relative resistance to adherence extended to the in vivo situation where bacteria is functionally different and is accompanied by an inflammatory component.
The question arises whether after the onset of infection the relative resistance to biofilm contamination results in preventing chronic infection of the tube. Future work may include quantifying the extent of biofilm formation, studying different bacteria types, and determining what other factors, such as topical antibiotics at time of tube insertion, affect susceptibility to biofilm formation.
CONCLUSION
An in vivo model was used to study the adherence of biofilms on 5 PE tube materials. No tube prevented otitis media with drainage. All tubes except the ion-implanted silicone tube showed dense inflammatory film adhesion after 10 days' incubation in the guinea pig model ear. With inoculation of the middle ear by S aureus, heavy bacterial biofilms developed on all PE tube materials except the ion-implanted silicone tubes. The ion-implanted silicone tubes showed only rare isolated clusters of individual bacteria, leaving the distinctive surface characteristics still visible. This in vivo model suggests that the adherence properties of the tube may be more important than antibacterial coatings in the prevention of persistent otorrhea.