
Abstract
Diplophonia is the production by the voice of 2 separate tones through quasiperiodic variations in the vocal fold vibration (Ward PH, Moore GP. Ann Otol Rhinol Laryngol 1969;78:771-7). Clinically, diplophonia can be observed in patients with unilateral vocal fold paralysis with incomplete glottal closure and a mass lesion of the vocal fold, intracordal cyst, and granuloma (Kiritani S, et al. Ann Bull RILP 1991; 25:55-62; Hirano M, et al. Ann Otol Rhinol Laryngol 1989;98:791-5). In this study we report 16 subjects with unilateral vocal cord paralysis or an intracordal cyst characterized perceptually by diplophonia. Diplophonia during tension imbalance may occur after surgery and is characterized by an improved perceptual score, a reduced number of vibratory cycles in each quasiperiodic waveform, and a reduced occurrence rate of the diplophonic waveform. During mass imbalance, no diplophonia occurred after surgery. Regarding the relationship of diplophonia with glottal condition at production of stops, in our study diplophonia varied significantly according to the different phonologic environments of stops during tension imbalance. We presume that there is a close relationship between the occurrence of diplophonia and the glottal conditions in tension imbalance, but not in mass imbalance.
The tensed vocal folds, which vibrate asymmetrically in different phases, can produce diplophonia. This condition depends largely, but not entirely, on the presence or absence of a glottal gap when the folds are in the resting Position. Isshiki et al 1 reported that the vibratory patterns of tension imbalance in vocal fold paralysis depend partly on the resting Position of the vocal folds: type I, the 2 folds vibrate at the same frequency, with glottal closure every period, for a resting Position at or near closure; type II, the 2 folds vibrate differently for wider resting Positions and can produce a phase shift resulting in diplophonia; and type III, the glottis never closes, and the vibrations become more periodic with reduced amplitude.
Theoretically, the mechanical effect of unilateral vocal fold paralysis (UVFP) should be to produce an imbalance in the tension and the level applied to the vocal folds during phonation. Such an asymmetry should produce some changes in the vibratory pattern of the vocal folds and in the resulting voice quality. Also, the mechanical effect of the mass imbalance, especially seen with an intracordal cyst (ICC), should produce a change in vibratory pattern. The ICC is usually filled with caseous contents, and a part of the cysts occasionally enters the vocal ligament and might interfere with the vibratory pattern. 2
In Korean stops, there is a 3-way distinction in manner of articulation classified as glottalized, lenis, and aspirated stops. The same manner of classification also applies to affricates, whereas fricatives are classified as either glottalized or lenis. Stops and affricates must occur in the word-initial Position to be realized as voiceless, whereas in the word-medial Position, the lenis type is usually manifested by voiced allophones. 3 Kagaya 4 reported on the fiberscopic and acoustic studies of the Korean stops. Kagaya determined that the glottalized type may be characterized by the completely adducted state of the vocal folds, the stiffened vocal folds and the abrupt decreasing of the stiffness near the voice onset, and the increasing subglottal pressure; the aspirated type may be characterized by the extensively abducted state of the vocal folds and the heightened subglottal pressure, but a lesser degree of abduction is observed for the lenis type.
On the basis of vibratory characteristics of diplophonia and glottal conditions of stops in tension imbalance, it is Possible to suggest that the vibratory pattern may be significantly related to the condition of glottal width in different phonologic situations. The purpose of this study was to investigate acoustically the relationship between the occurrence of diplophonia and the glottal condition during explosion of a stop before voice onset for a vowel during tension imbalance and mass imbalance.
Subject characteristics
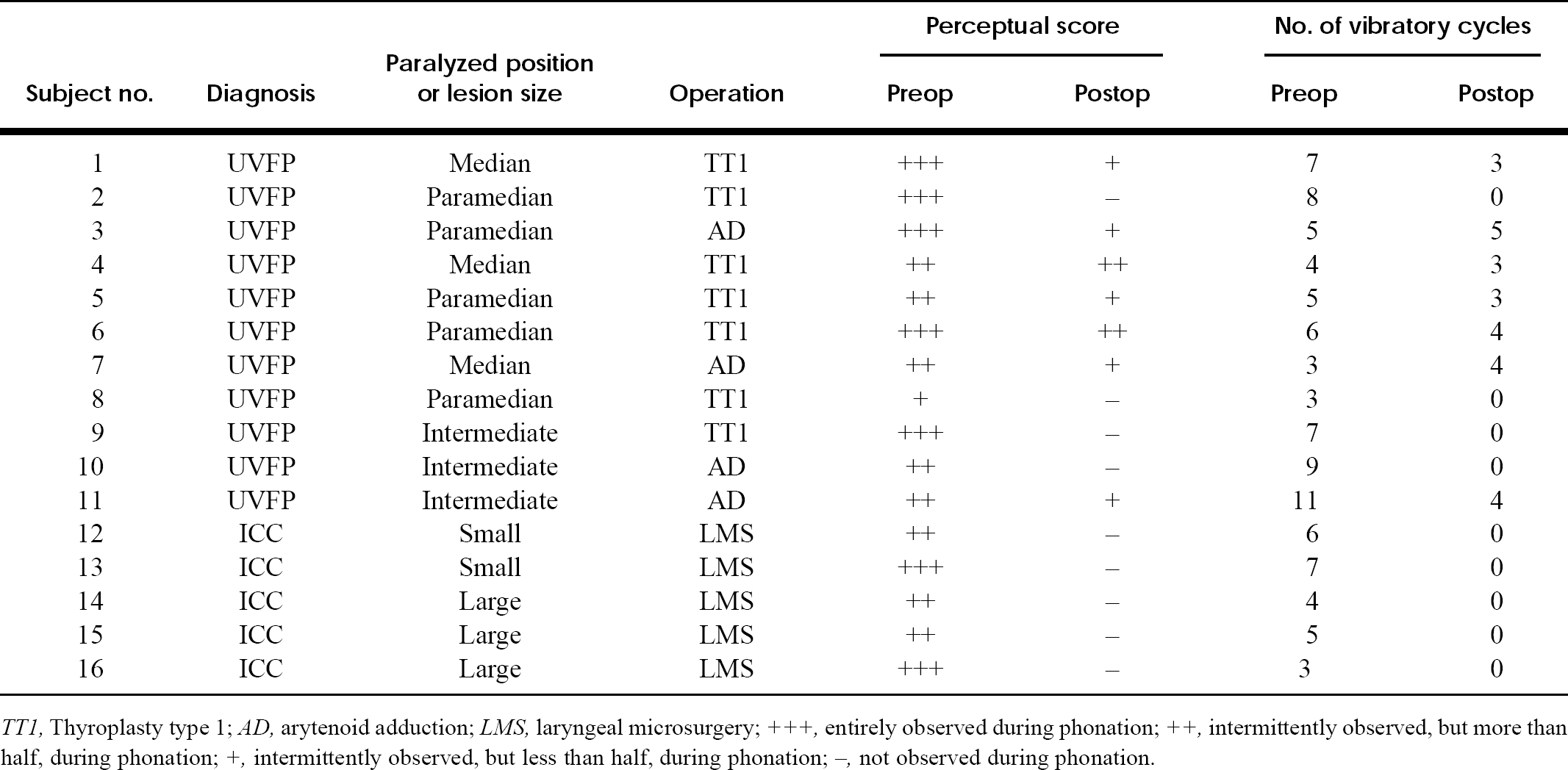
TT1, Thyroplasty type 1; AD, arytenoid adduction; LMS, laryngeal microsurgery;
+++entirely observed during phonation;
++intermittently observed, but more than half, during phonation;
+intermittently observed, but less than half, during phonation;
-not observed during phonation.
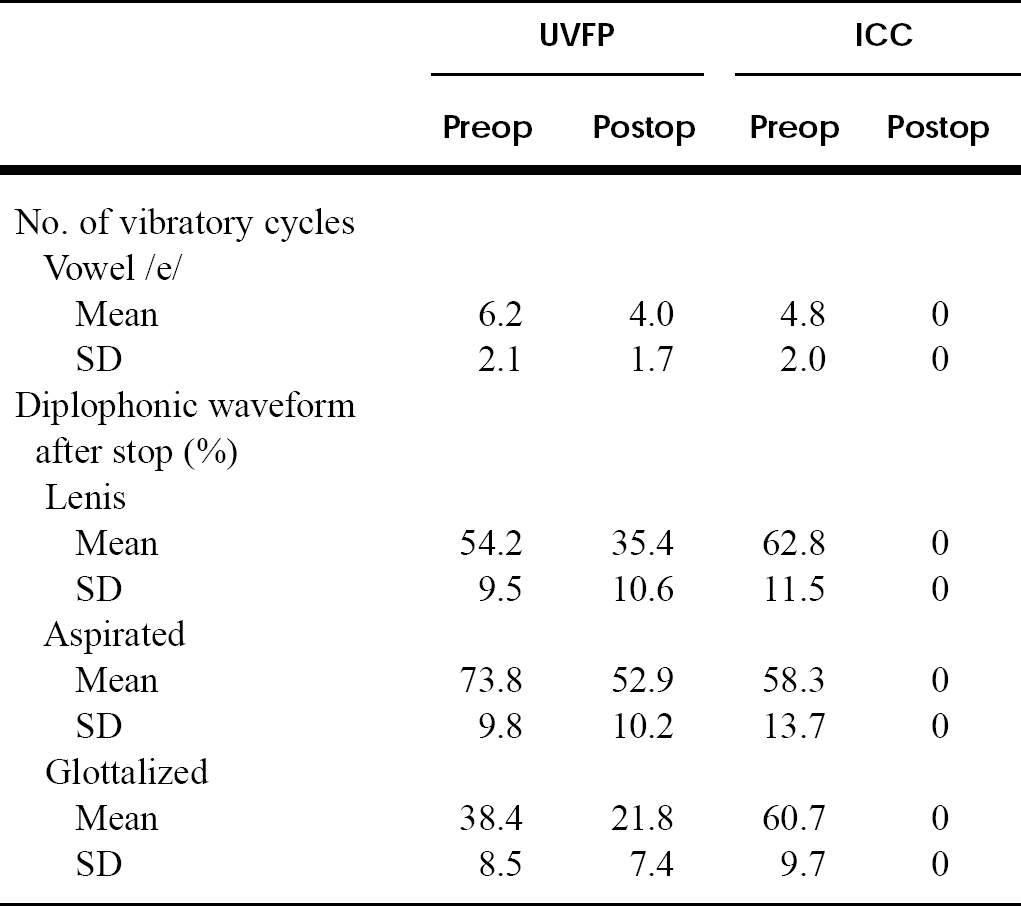
Mean values of vibratory cycles and occurrence of diplophonic waveform
METHODS AND MATERIAL
Subject and Speech Materials
We studied patients with UVFP and ICC who had diplophonia during sustained vowel production. A total of 16 patients with unilateral vocal cord paralysis (11 cases) or ICCs (5 cases), all native Korean speakers of the Chonbuk dialect, were the subjects of this experiment (table 1). Patients with UVFP underwent thyroplasty type I (7 cases) or arytenoid adduction (4 cases) for medialization of the paralyzed vocal fold based on Isshiki's 5 model. Patients who had ICCs underwent excision of their cysts by laryngeal microsurgery with the suspension laryngoscope (Hirano's 2 method).
For the perceptual and acoustic measures, the patients were asked to produce the sustained vowel /e/ and test words composed of stops and vowels (/CVCV/) as comfortably as Possible. The test words were prepared so as to place the stops in different phonologic environments: the dental stops, the aspirated stop /thethe/, the lenis stop /tete/, and the glottalized stop /t'et'e/.
Voice Recording
The subjects were placed in a sound-treated booth and were asked to utter the above speech materials 10 times repeatedly at a comfortable pitch and loudness level. Care was taken to keep pitch and speed at as constant a level as Possible. The mouth-to-microphone distance was approximately 20 cm. The voice recordings were made through a digital tape recorder and high-fidelity microphone before surgery and 3 weeks after surgery.
Perceptual Score of Diplophonia During Phonation of Sustained Vowel
Listeners were 3 healthy adults who were familiar with diplophonic voice and experienced in speech evaluation. The listeners were instructed to select the score of diplophonia voice during phonation with the recorded sustained vowel /e/.
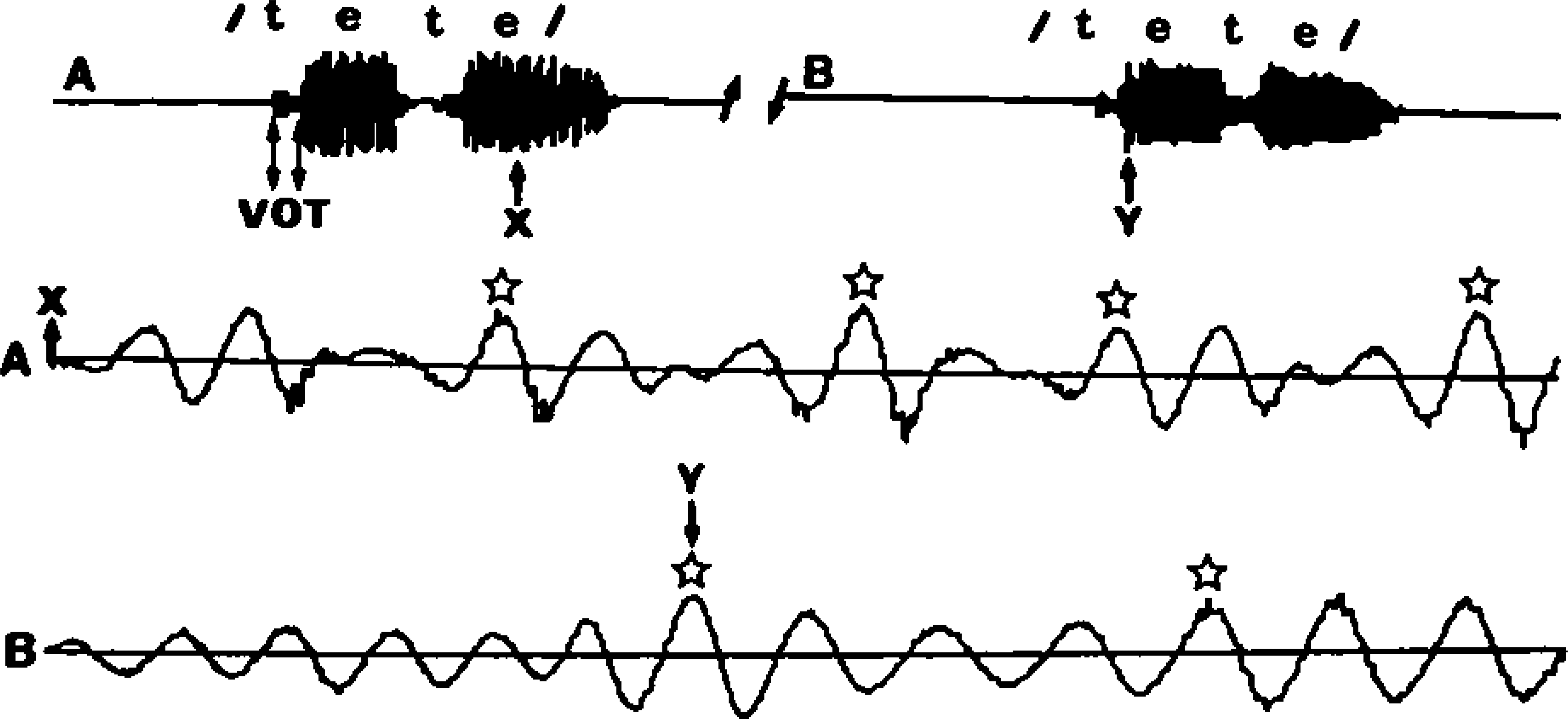
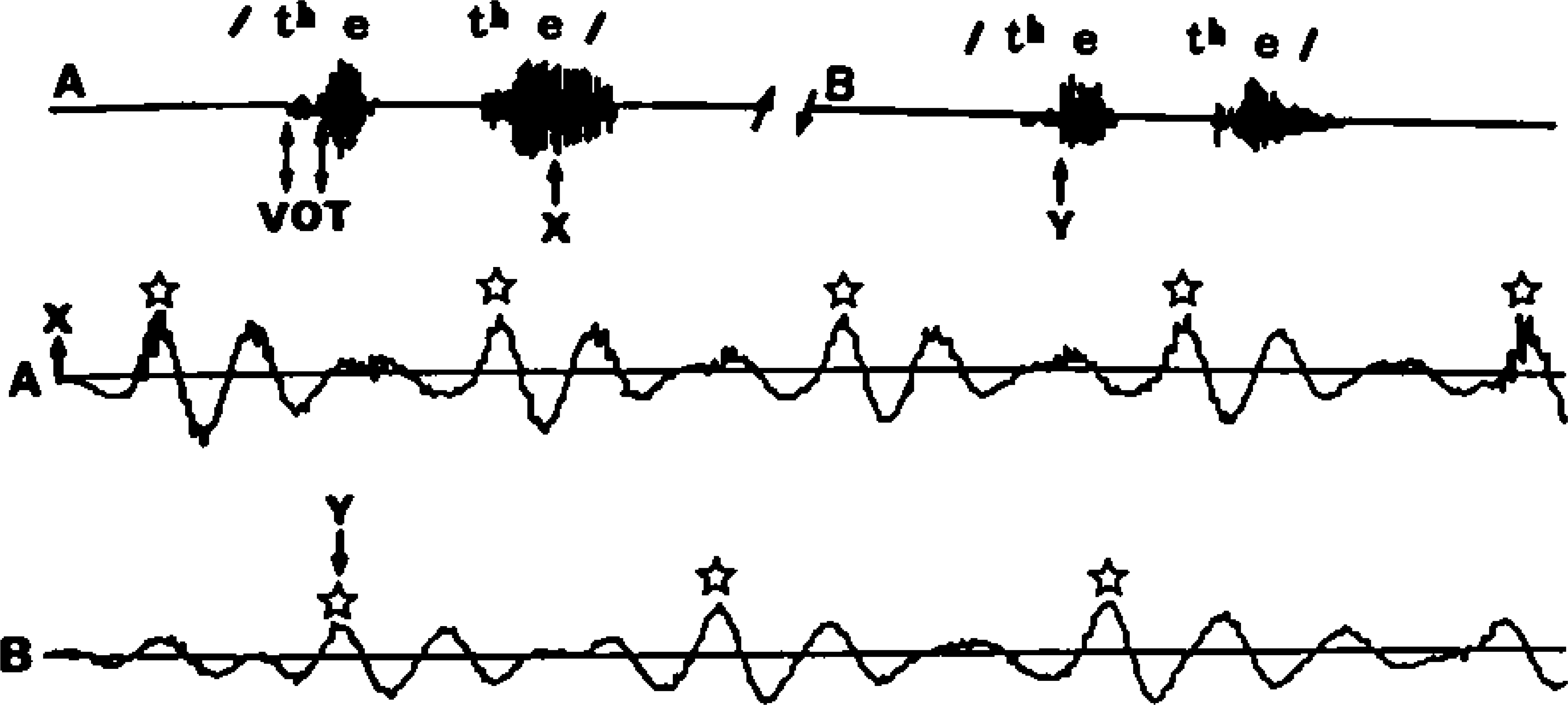
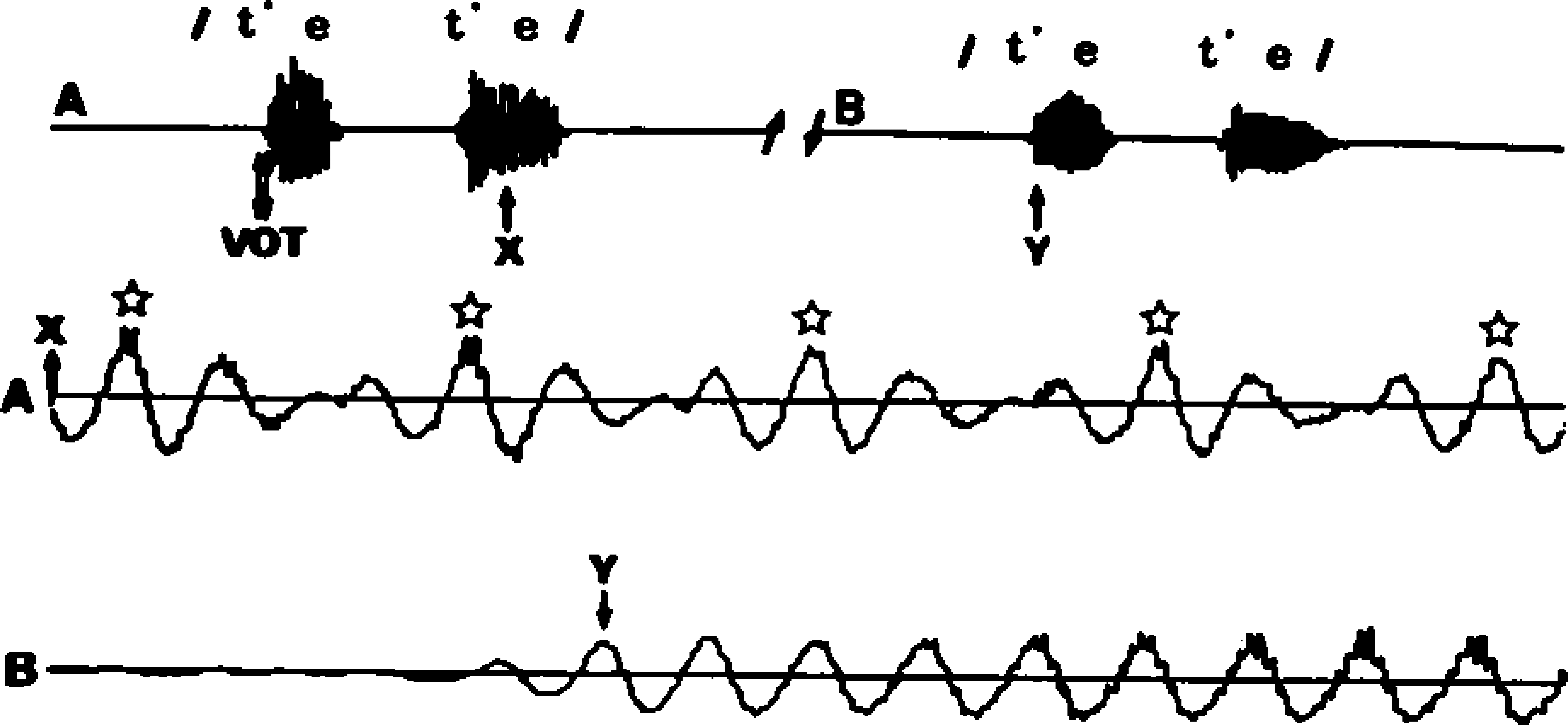
Time-scaled speech waveforms for the sustained vowel /e/. Top, Original waveform with regular variations of amplitude. Bottom, Expanded waveforms with quasi-periodic variation of vibratory cycles. A-B, One quasiperiodic waveform; numerals, number of vibratory cycles in 1 quasiperiodic waveform. Speech waveforms for the lenis stop consonant in /tete/ before (A) and after (B) surgery. Top, Original waveform; middle and bottom, expanded waveforms. VOT, Voice onset time. Diplophonic waveforms are well documented before (middle) and after (bottom) surgery but are not very distinct. X, Midpoint of vowel; Y, beginning of vowel; stars, peaks of quasiperiodic cycles. Speech waveforms for the aspirated stop in /thethe/ before (A) and after (B) surgery. Top, Original waveform; middle and bottom, expanded waveforms. VOT, Voice onset time. Diplophonic waveforms are well documented before (middle) and after (bottom) surgery. Speech waveforms for the glottalized stop consonant in /t'et'e/ before (A) and after (B) surgery. Top, Original waveform; middle and bottom, expanded waveforms. VOT, Voice onset time. Diplophonic waveforms are well documented before surgery (middle) but not after surgery (bottom). X, Midpoint of vowel; Y, beginning of vowel; stars, peaks of quasiperiodic cycles.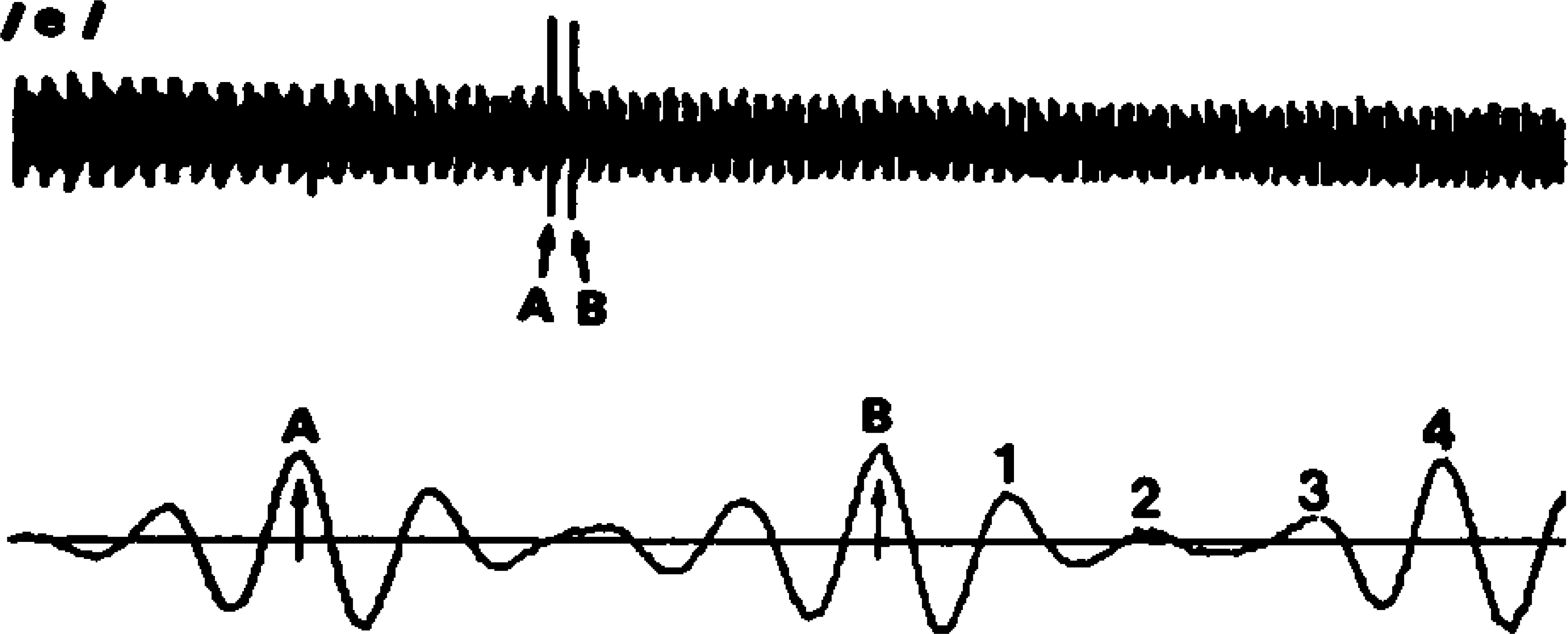
Acoustic Analysis
We used the computerized speech analysis system introduced by Imagawa and Kiritani. 6 This computer has a 640-kilobyte main memory, and the DSP board contains a 32-bit floating-Point DSP chip and 32 kilobytes of external RAM. For extraction of the diplophonic waveform with acoustic analysis, the speech signals were sampled through an A/D converter, and the amplitude envelope of the speech wave were displayed. The time scale-expanded speech wave was displayed at the bottom of the screen, and we could see easily whether the quasiperiodic waveform for diplophonia occurred. We measured the number of vibratory cycles in each quasi-periodic waveform for the sustained vowel /e/ and calculated the occurrence rate of the diplophonic waveform related to the 3 types of Korean stops during repeated utterances before and after operation. The number of vibratory cycles in each quasi-periodic waveform were measured for the sustained vowel /e/ with the time scale-expanded speech waveform (Figures 1). Before and after surgery, the diplophonic waveforms after explosion of the aspirated stop (Figures 2), the glottalized stop (Figures 3), and the lenis stop (Figures 4) were shown in patients with UVFP.
RESULTS
Perceptual Findings and Number of Vibratory Cycles with Sustained Vowel
Perceptual scores showed various degrees before surgery (table 1). Perceptually, in those with UVFP, diplophonic voice was decreased (subjects 1, 3, 5, 7, and 11), absent (subject 2, 8, 9, 10), or unchanged (subject 4) after surgery. However, no cases of ICC showed diplophonic voice after surgery. This difference was particularly significant. The type of surgery used for UVFP did not affect the perceptual score, even though the sample size was too small for statistical analysis.
The number of vibratory cycles in each quasiperiodic waveform varied inconsistently among subjects (table 2) and was not statistically significant (P > 0.05) between patients with vocal fold paralysis and ICCs before surgery. After surgery, among 7 patients with UVFP showing diplophonia, 6 patients had a decreased number of vibratory cycles, whereas 1 subject had an increased number. However, no patients with ICCs had diplophonia after surgery.
Occurrence Rate of the Diplophonic Waveform in the Stop Consonants in /CVCV/
Table 2 illustrates the occurrence rate of the diplophonic waveform according to 3 types of stop consonants. Before surgery the mean rate of occurrence of the diplophonic waveform was 54.2% for the lenis, 73.8% for the aspirated, and 38.4% for the glottalized stops in patients with UVFP, and 62.8% for the lenis, 58.3% for the aspirated, and 60.7% for the glottalized stops in patients with ICCs (table 2). For UVFP, the differences between stops were statistically significant between the aspirated and the glottalized (P < 0.01), between the aspirated and the lenis (P < 0.01), and between the lenis and the glottalized stops (P < 0.05). For ICCs there was no significance between the types of stops. Two groups, including those with UVFP and those with ICCs, showed statistically significant results in the aspirated (P < 0.01) and the glottalized (P < 0.01), but not in the lenis (P > 0.01), stops by the Student t test. After surgery the mean rate of occurrence of the diplophonic waveform was 35.2% for the lenis, 52.9% for the aspirated, and 21.8% for the glottalized stops in patients of the UVFP; this difference was also statistically significant among 3 types of stops (P < 0.01) by the Student t test. However, there was no diplophonia in the group of patients with ICCs after surgery.
DISCUSSION
Diplophonia is the simultaneous production by the voice of the frequency difference between the vocal folds and the temporal alternation between the vibratory patterns with and without a closure period. 7 In diplophonia 2 sources of tone are usually similar in quality and loudness but distinctly different in pitch and can be distressing to the speaker.
There is a series of papers concerning the physiologic conditions underlying irregular vocal fold vibration. Isshiki et al 1 have investigated the effect of asymmetric vocal fold tension on vibration through high-speed motion pictures of the excised larynx as well as through computer simulation based on Ishizaka-Flangan's 2-mass model. 8 Isshiki et al 1 and Kiritani et al 9 reported that the pattern of abnormal vibration varies depending on the glottal area at rest and that irregular vibrations are brought about only when the glottal area at rest is set at some intermediate value. Tanabe 10 noted that simple tension imbalance did not cause a difference in the vibratory frequency between the vocal folds in the excised larynx experiment and that an additional perturbation of the laryngeal conditions such as the difference in the level of the vocal folds was necessary to bring about the frequency difference. However, Ishizaka and Isshiki 8 reported the results of computer simulation, which suggest that a tension imbalance can cause a frequency difference under certain conditions of the glottal area at rest and the subglottal pressure. The mechanism of the phase shift caused by frequency difference seems most likely to be attributable to the faster movement of the stiffer vocal fold, resulting from its higher characteristic frequency. The phase shift between the 2 cords is the most important sign of the tension imbalance but does not always mean a tension imbalance exists. It also occurs in the case of a mass imbalance between the 2 cords in which a vocal cord with the massive mass of the cyst usually vibrates with a noticeably reduced amplitude. 1
In this study diplophonia definitely developed in the case of tension imbalance with incomplete glottal closure and mass imbalance without incomplete glottal closure. Perceptual evaluations of the diplophonic voice with sustained vowels showed various scores and were not different between the 2 groups before surgery. The patients in whom laryngoplastic phonosurgery did not resolve the diplophonia were composed of 3 of the 4 cases of arytenoid adduction and 4 of the 7 cases of type I thyroplasty, but most cases showed reduced perceptual scores and a reduced number of vibratory cycles after surgery.
The diplophonia did not resolve in 3 of 4 patients with arytenoid adduction because of the differential viscoelastic properties of the musculomembranous vocal folds and the resulting differential susceptibility to Bernoulli's forces. In 4 of 7 patients who underwent medialization without arytenoid adduction, the diplophonia also related to persistent Posterior aerodynamic glottal incompetence and associated elevated subglottic driving pressures.
Recently the arytenoid adduction was done with implant medialization laryngoplasty. We expect that this combined arytenoid adduction resolved persistent Posterior glottal incompetence and led to elevated subglottic driving pressures and, in turn, diplophonia. Unfortunately, we did not perform the combined laryngoplastic phonosurgery in this study. If we had performed this combined laryngoplastic phonosurgery, better results might have been expected. However, the diplophonia may not be absolutely correlated with glottal incompetence. Patients who showed no glottal incompetence still have diplophonia because of reduced tension of the paralyzed vocal fold.
This study reveals that the diplophonia in the UVFP occurred differently according to the types of Korean stops, which means glottal conditions differed according to the stops. The degree and timing of glottal gesture for the production of Korean stops are controlled by a reciprocal activity pattern of the adductor and abductor muscle groups of the larynx 3 ; the stops have been studied and observed by electromyographic patterns of the adductor muscle and by fiberscopic study revealing that the glottal opening is smaller for glottalized than for the other 2 Korean stop stops. 4,11 The occurrence rate of the diplophonic waveform during production of stops did not show statistical significance between patients with UVFP and those with ICCs before surgery but did show a significant increase in the aspirated compared with the lenis and the glottalized stops in UVFP. This difference means that the diplophonia may depend on the wide glottal width at the time of explosion. After surgery in the UVFP group, the stops showed the same order of frequency—higher in the aspirated followed by the lenis and glottalized—but the occurrence rate was lower than before surgery. This means that the occurrence of the diplophonic waveform has a relationship with 3 types of Korean stops, in other words, with glottal condition at the explosion of the stops after surgery. The wider glottal gap at the production of an aspirated stop resulted in a higher occurrence rate of diplophonia during tension imbalance, but the smaller glottal gap at the glottalized stop produced the low occurrence rate of diplophonia. The occurrence of the diplophonic waveform for the patients with ICCs was not present after surgery.
In summary, diplophonia may occur during the tension imbalance caused by sustained paralysis after laryngoplastic phonosurgery. During the mass imbalance, the diplophonia was not present after surgery. Diplophonia depends more on the glottal condition at the production of stops during tension imbalance before and after surgery, but not during mass imbalance. The larger glottal gap at the explosion of stop results in a higher occurrence rate of diplophonia during production of vowels, and the small glottal gap has a low occurrence rate.