
Abstract
With the rise in Popularity of all-terrain vehicles (ATVs), especially in rural America, injuries associated with their use are becoming more commonplace. A retrospective review was conducted of 153 patients with ATV-related injuries seen at West Virginia University Hospitals between January 1990 and June 1996. Of these patients, 33 had maxillofacial injuries. Only 2 of 21 (9.5%) patients noted to be wearing helmets had facial injuries, whereas 17 of 19 (89.5%) patients who had facial injuries were not wearing helmets. Most patients with maxillofacial injuries occurring at night had been drinking alcohol. Injury Severity Scores were worse for those patients with maxillofacial injuries, as well as for those patients who had been drinking alcohol. Patients with maxillofacial injuries were more likely to require a stay in the intensive care unit. Furthermore, children with facial injuries had higher Injury Severity Scores and longer hospital stays than the adults. To reduce these accidents and related injuries, the industry, local and federal governments, and ultimately individuals must change their attitudes regarding these Potentially dangerous vehicles.
All-terrain vehicles (ATVs) were introduced into the US market in the late 1970s and have become a Popular form of motorized recreation, but they have also contributed to a number of serious injuries and fatalities. These vehicles can weigh up to 500 lb and can exceed speeds of 65 mph. They have been made in both 3-wheel and 4-wheel models, but since January 1988, the federal government has banned all sales of 3-wheel ATVs because of their high death and injury record and their inherent instability. 1 Between January 1982 and June 1995, the US Consumer Product and Safety Commission reported 2638 deaths from ATV accidents in the United States, with 73 deaths in West Virginia. Although the national risk of death (per 10,000 ATVs in use) decreased 40% from 1985 to 1993, there were still 59,200 ATV-related hospital emergency department-treated injuries in 1994, 24,800 of which involved patients younger than 16 years. 2 Currently, there are no published reports specifically addressing maxillofacial injuries caused by ATV accidents.
METHODS AND MATERIAL
Between January 1990 and June 1996, 153 patients with ATV-related injuries were evaluated at West Virginia University Hospitals. Of these, 33 patients had least 1 maxillofacial injury. Facial and scalp lacerations were not included. A retrospective review of data regarding patient age, time of day, type of vehicle, scene of accident, helmet status, use of alcohol, Glascow Coma Scale score (GCS), Injury Severity Score (ISS), associated injuries, procedures, and length of stay in the intensive care unit (ICU) and hospital were obtained from each individual's chart. The ISS was calculated at the time of presentation of the patient and was based on the method described by Baker et al. 3-5
RESULTS
A total of 153 patients were evaluated at West Virginia University Hospitals and enrolled in the institutional trauma registry; 33 (21.6%) of these patients had at least 1 maxillofacial injury. The overall mean age was 26.4 years (range 2-70 years). The average age for patients with maxillofacial injuries was 28.2 years versus 25.9 years for those patients without facial injuries. All accidents occurred off-road. It was not obvious in all cases whether the ATV was being used for recreation or work.
ATV accident-related injuries occurred most commonly in May, June, and July, but occurred throughout the year. Saturday night was the most common night for these injuries. Males had a higher incidence of nighttime accidents (29.5%, 34/115) than females (14.2%, 3/21). The overall male-to-female ratio was 4.7:1. Thirty-five of 153 (22.9%) patients were younger than 16 years. Seven of these 35 (20%) had maxillofacial injuries, whereas 26 of 118 (22%) patients 16 years of age and older had maxillofacial injuries (P = 0.8).
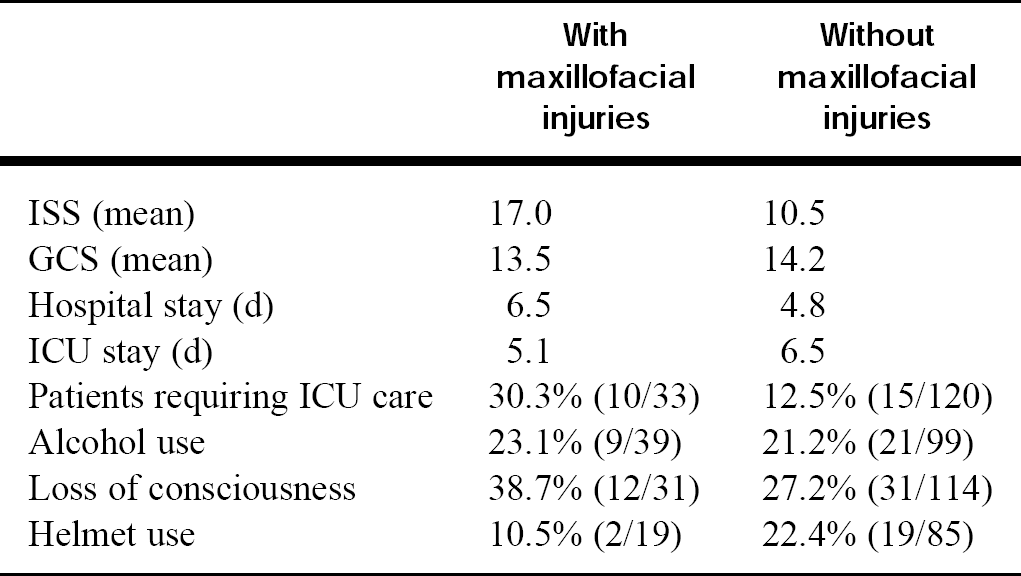
Comparisons
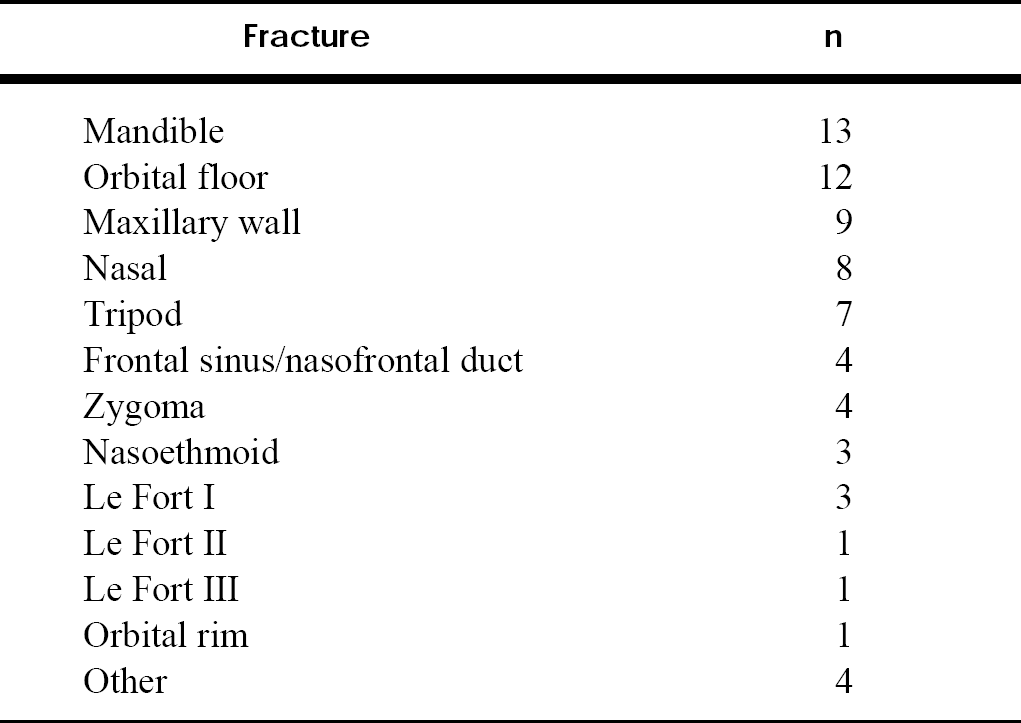
Frequency of maxillofacial fractures
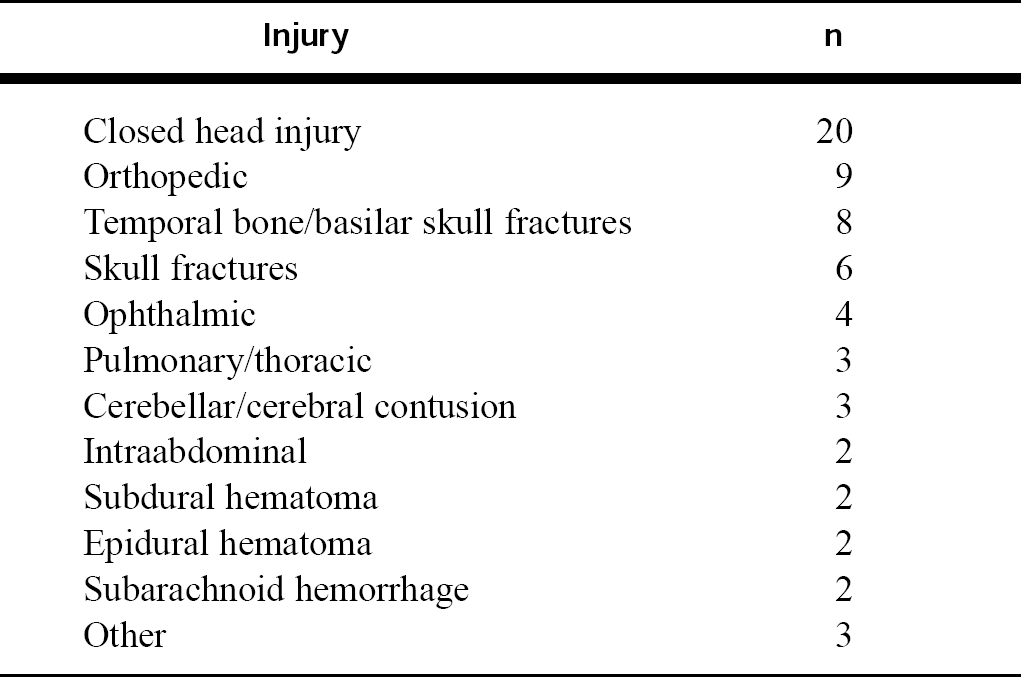
Associated injuries for those patients with maxillofacial injuries
Maxillofacial procedures
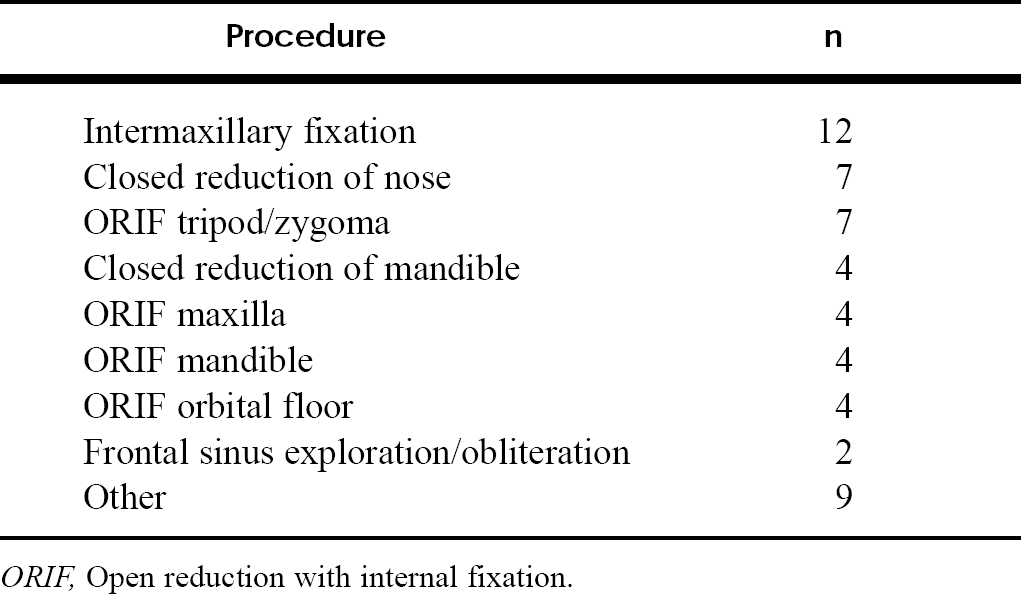
ORIF, Open reduction with internal fixation.
Eighteen of 35 (51.4%) nighttime accidents and 19 of 98 (19.4%) daytime accidents were alcohol related. Alcohol was involved in 35 of 114 (30.7%) male injuries and 4 of 24 (16.7%) female injuries.
Twelve of 31 (38.7%) patients with maxillofacial injuries lost consciousness, whereas 31 of 114 (27.2%) without facial injuries lost consciousness (P = 0.2). Two of 21 (9.5%) patients who were wearing helmets sustained maxillofacial injuries, whereas 17 of 83 (20.5%) patients without helmets sustained maxillofacial injuries (P = 0.35). Twenty-seven of 31 (87.1%) patients who had been drinking alcohol were not wearing helmets, whereas 53 of 68 (77.9%) who were not drinking alcohol were not wearing helmets. Few data were available regarding open versus closed face helmets. Alcohol was used by 9 of 30 (30%) with maxillofacial injuries and 30 of 108 (27.8%) without maxillofacial injuries. Nine of 39 (23.1%) patients who were drinking alcohol sustained maxillofacial injuries, whereas 21 of 99 (21.2%) patients who were not drinking alcohol sustained maxillofacial injuries. The GCS average was 13.55 for patients with facial injuries and 14.16 for patients with out facial injuries (P = 0.4). The ISS average was 17 for patients with maxillofacial injuries and 10.5 for patients without facial injury (P = 0.001).
The average hospital stay was 6.52 days for patients with facial injuries and 4.80 days for those without facial injuries. Ten of 33 (30.3%) patients with maxillofacial injuries required ICU admission, whereas only 15 of 120 (12.5%) patients without maxillofacial injuries required ICU care (P = 0.01) (table 1). However, the average ICU stay was longer for those patients without facial injuries (6.5 vs 5.1 days). Six of 26 (23.1%) patients 16 years or older required ICU admission, whereas 4 of 7 (57.1%) children younger than 16 years required such an admission (P = 0.08).
Mandible fractures (13) followed by orbital floor fractures (12) (table 2) were the most common maxillofacial injuries.
Closed head injuries were the most commonly associated injuries seen in 20 of these patients. Nine patients had orthopedic fractures, whereas 7 had temporal bone/basilar skull fractures (table 3).
Twenty-five patients underwent surgery for their maxillofacial injuries, with the most common procedure being intermaxillary fixation (table 4). Ten patients required 1 procedure, 7 patients required 2, 7 patients required 3, and 2 patients required 4. Complications from these injuries and surgical procedures included ectropion, diplopia, headaches, and hypoesthesia, among others. Twelve patients had at least 1 of these complications. Follow-up was difficult to assess because many were lost to follow-up, especially when no surgical procedure was necessary. Some chose to return to their local physician for follow-up. Only 1 patient who had a maxillofacial injury died.
DISCUSSION
Although the annual numbers of fatal accidents have gradually decreased since 3-wheeled ATVs were banned, the Popularity of these vehicles has steadily risen, especially among young adults and children. Numerous maxillofacial injuries, with the vast majority involving the 4-wheel ATV variety, were still evaluated. 6 No significant relationship between age, time of accident, and ISS was found.
The prevalence of maxillofacial injuries in patients who were unhelmeted was noteworthy. Of the patients with maxillofacial injuries, only 2 of 19 (10.5%) were wearing helmets. On the other hand, if a helmet was worn, only 2 of 21 (9.5%) sustained maxillofacial injuries. It would have been even more beneficial if data regarding all patients could have been available along with the type of helmet. Similar studies involving motorcycle accidents have revealed that unhelmeted patients are nearly 1.5 to 3 times as likely as helmeted patients to have facial fractures. 7,8 Patients with maxillofacial injuries were more likely to require ICU care (10/33, 30.3%) than those without maxillofacial injuries (15/120, 12.5%) (P = 0.01).
Alcohol use was not significantly different between the facial injury and nonfacial injury patients. However, only 1 of the patients with maxillofacial injuries wore a helmet and had not been drinking alcohol. Nineteen percent of maxillofacial injuries occurring in daylight were alcohol related, whereas 51% of those occurring in darkness were alcohol related (P < 0.01).
ISSs were significantly higher when alcohol was involved (P < 0.001). ISSs were also significantly higher in the patients with maxillofacial injuries (P < 0.001).
Operation of these vehicles is largely unregulated for children. Four of 7 (57.1%) of the children injured required some ICU care, whereas 6 of 26 (23.1%) of adults required ICU care (P = 0.08). Hospital stays were also noted to be longer for children versus adults at 6.14 days for children and 5.77 days for adults. ISS averages were 17.38 for adults and 18.29 for children. These data Portray the severity of the injuries incurred by this younger Population.
CONLUSIONS
Maxillofacial trauma is a significant problem that continues to be on the rise in the 20th century with the introduction of vehicles that have led to high-energy accidents. The addition of ATVs has provided another vehicle that can impart heavy trauma to its occupants. Although there has been a steady decline in fatal ATV accidents per 10,000 ATVs in use, there continue to be numerous maxillofacial injuries.
Although the use of ATVs in the United States is gaining Popularity, especially in rural areas, enforcement of government regulations and industry safety standards is difficult. Injuries from ATVs are usually not as high impact as those from other motorized vehicles, but many ATV-accident patients have significant maxillofacial trauma and associated injuries. The social and economic costs, although not the emphasis of this review, are undoubtedly significant. Analysis of health care costs in other studies found costs to be 23% to 60% greater in unhelmeted motorcycle patients. 9,10 With similar findings regarding ISSs, GCSs, and length of hospitalization and ICU stay, a similar increase in costs would be expected in our unhelmeted and facial injury patients. Many of these injuries likely could be avoided or lessened in severity if appropriate precautions were taken.
Because the severity of these injuries appears to be more significant for children, banning or further restricting their use by this Population may be of value. Avoiding or banning advertising campaigns targeting children and adolescents would be a Possible step. Currently, children are allowed to operate these vehicles with the only limit being the size of the vehicle and engine based on the driver's age.
Training is encouraged by the industry; often some rebate is offered when the driver takes courses, but these are not required. A review of prospective buyers’ driving records and any previous arrests for driving while intoxicated may also prove to be helpful in screening Potential customers.
Ultimately, personal responsibility is paramount. Even with some of the previously mentioned safety recommendations, their implementation on a personal level is most important. Using secure fitting helmets, avoiding alcohol use, and avoiding 3-wheeled ATVs are the responsibility of individuals once they are properly trained and educated in this area. Parents should be educated about the dangers of ATVs for their children and should be encouraged to avoid these vehicles. As long as the current situation exists with regard to these vehicles, this is the best that can be hoped for.
Footnotes
Your comprehensive reference to valuable research information…
Otolaryngology-Head and Neck Surgery provides its readers with timely information on recent treatments and advances in otolaryngology.
Now you can have easy access to that information with the five-year cumulative author and subject index to Volumes 104-113 of Otolaryngology-Head and Neck Surgery.
The Cumulative Index is your comprehensive reference guide, including a list of every article in the journal from 1991 through 1995. All articles are indexed both by subject and by author.
The Cumulative Index features:
Credit Card #_______ Exp. Date___________
Signature_______________
Name_______________
Institution____________
Address_______________________
City____________ State_____________
ZIP_______________ Country____________
1-800-453-4351
Outside the U.S.: 314-453-4351 Fax: 314-432-1158
Mosby, Inc. Journal Subscription Services 11830 Westline Industrial Dr. St. Louis, MO 63146 U.S.A.