
Abstract
PURPOSE: To ascertain the characteristics unique to malignant schneiderian papilloma (MSP).
METHODS: A case-control study of all schneiderian papilloma (SP) patients treated between 1978 and 1997 was conducted. Comparison was made between patients with MSP and patients with benign SP (BSP).
RESULTS: A diagnosis of SP was made in 72 patients. Malignant changes, all of them the inverted papilloma subtype, were found in 8 of these patients. Three were diagnosed carcinoma in situ, and 5 were defined as invasive squamous cell carcinoma. At presentation, the MSP patients had significantly larger tumor spread into the ethmoid and sphenoid sinuses. The recurrence rate was significantly lower in SP patients treated with extensive surgical procedures. An association was found between the presence of malignant lesions and Positive smoking history, subjective awareness of a nasal mass, and ethmoid and sphenoid sinus involvement. Also, histologic multicentricity was a feature more often seen in MSP than BSP and was a significant correlate with malignancy.
CONCLUSION: The physician evaluating a patient with SP should be aware of the features described and of their Possible association with a malignant lesion.
Schneiderian papilloma (SP) is an uncommon tumor of the nose and paranasal sinuses, representing 0.5% to 4% of all primary nasal neoplasms. 1 First described by Ward 2 in 1854, these benign tumors derive their name from the involution of the surface epithelium that lines the nasal cavity and nasal sinuses, also known as the schneiderian mucosa, into the underlying stroma. 3,4
There are 3 primary types of SP: inverting, cylindrical, and fungiform. Both the inverting and cylindrical forms have been associated with malignancy, whereas the fungiform variety has rarely been associated with malignancy.
Although the cause of SP remains undetermined, evidence Points to a viral cause. 5 SP patients typically have some degree of nasal obstruction, as well as the presence of a nasal mass and sinusitis. 6-8 Clinically, these tumors act locally aggressive, most often involving the lateral nasal wall, with extension into the maxillary or ethmoid sinuses with variable degrees of bony erosion. 9,10 Potential malignant transformation, as well as the coexistence of carcinoma within the tumor, has been described. 9,11-13
The purpose of this study was to identify and define the characteristics unique to malignant lesions associated with SP (MSP).
METHODS
A chart review of all patients found to have SP at our institution between 1978 and 1997 was undertaken. Those defined as having malignant changes were identified and defined as the study group.
Pathologic Examination
A single pathologist performed the histologic analysis. Epithelial alterations—including dysplasia, carcinoma in situ, and invasive carcinoma—were assessed according to standard criteria. 14 Cases with atypia only and mild dysplasia were not included in the study group. Architectural patterns—namely, inverted, fungiform, or cylindrical—and multicentricity of the tumor were also noted.
Data Collection
The following variables were evaluated in the study group: age, sex, presenting symptoms, smoking and alcohol consumption history, primary site of tumor involvement, surgical intervention, disease recurrence, and long-term follow-up. The results were compared with data from benign SP (BSP) patients, who served as the control group.
Statistical Analysis
The χ2-test was used for an expected frequency of 5 or more per cell. In cases of smaller numbers, the Fisher exact test was used. We accepted P < 0.05 as statistically significant.

MSP with carcinoma in situ (bottom) evolving to well-differentiated squamous cell carcinoma (top). (Hematoxylin-eosin stain; original magnification x125.)
One focus of squamous cell carcinoma with frank invasion, found in the same specimen shown in Fig 1. (Hematoxylin-eosin stain; original magnification x125.)
RESULTS
At our hospital, SP was diagnosed in 72 patients between 1978 and 1997. Among these, 8 cases of MSP were identified and included in the study group, and 64 cases of BSP were included in the control group. The follow-up time for all 72 patients was between 11 and 227 months, with a median of 124.5 months. No significant difference in the follow-up time was found between the 2 groups. The MSP group consisted of 3 cases of carcinoma in situ and 5 cases of invasive squamous cell carcinoma. Figures 1 demonstrates both carcinoma in situ and well-differentiated squamous cell carcinoma. Figures 2 shows invasion of the tumor in the same specimen.
Seven of the MSP patients were men, and 1 was a woman, ranging in age from 49 to 77 years at the time of diagnosis. There was no difference in patient age between the groups. The mean age ± SD in the MSP group was 62 ± 10 years, and in the BSP group it was 54 ± 11 years.
Smoking rate was significantly higher in the MSP group than in the control group (75% vs 16.2%, P = 0.000). There was no significant difference of history for alcohol abuse or exposure to environmental carcinogens between the groups.
The presenting symptoms of the patients in the study and the control groups are summarized in table 1, the most common in both groups being unilateral nasal obstruction. Report of a nasal mass was significantly higher at presentation in MSP patients, 87.5% compared with 12.5% in BSP patients (P = 0.000). Nasal discharge was a common symptom (21%) in the BSP group but was not evident in the MSP group. In 5 patients of the MSP group, the nasal masses found were defined as Polyps, and the diagnosis was done after nasal Polypectomy.
The extent of spread of the disease, on the basis of histologic findings in the surgical specimens, is summarized in table 2. Lateral nasal wall involvement was detected in 5 patients, ethmoid involvement in 6, and sphenoid involvement in 4. Infiltration of the ethmoid or sphenoid sinuses by tumor was significantly more frequent in the MSP group than in the BSP group (P = 0.013 for ethmoid, 0.009 for sphenoid).
A summary of the histologic features in the 72 SP patients is presented in table 3. No significant difference in the rate of histologic subtypes was found between the groups. Histologic evidence of multicentric lesions was found in 4 (50%) patients in the investigation group but only 1 patient (1.6%) in the control group, which was significant (P = 0.002).
Surgical management consisted of either conservative or radical surgery. Conservative management involved the Caldwell-Luc procedure with or without external ethmoidectomy, endoscopic excision, or local excision with adequate margin attainment. Radical surgery involved at minimum, lateral rhinotomy with medial maxillectomy. Of the 8 patients in the investigational group, 6 (75%) underwent radical surgery, with 2 (25%) being treated conservatively. In comparison, in the control group 34 of 64 (53.1%) were treated conservatively, and 30 of 64 (46.9%) were treated aggressively.
The recurrence rate, according to the type of surgery, is summarized in table 4. In the patients treated conservatively, 2 of 2 (100%) in the MSP group and 15 of 35 (42.9%) in the BSP group had recurrence of their disease. In the MSP patients treated aggressively, 1 of 6 (16.7%) had recurrent disease. No recurrence was evident in 29 patients in the control group who had under-gone radical surgery. In summary, the overall recurrence rate for SP patients treated aggressively was 1 of 35 (2.9%), whereas the overall recurrence rate for those treated conservatively was 17 of 37 (45.9%). This difference in the efficacy of the surgical approach regarding recurrence is statistically significant (P = 0.000). The relative risk of recurrence in MSP patients treated with radical surgery is only 14.3% of that in MSP patients treated with limited procedures.
Presenting symptoms in SP patients
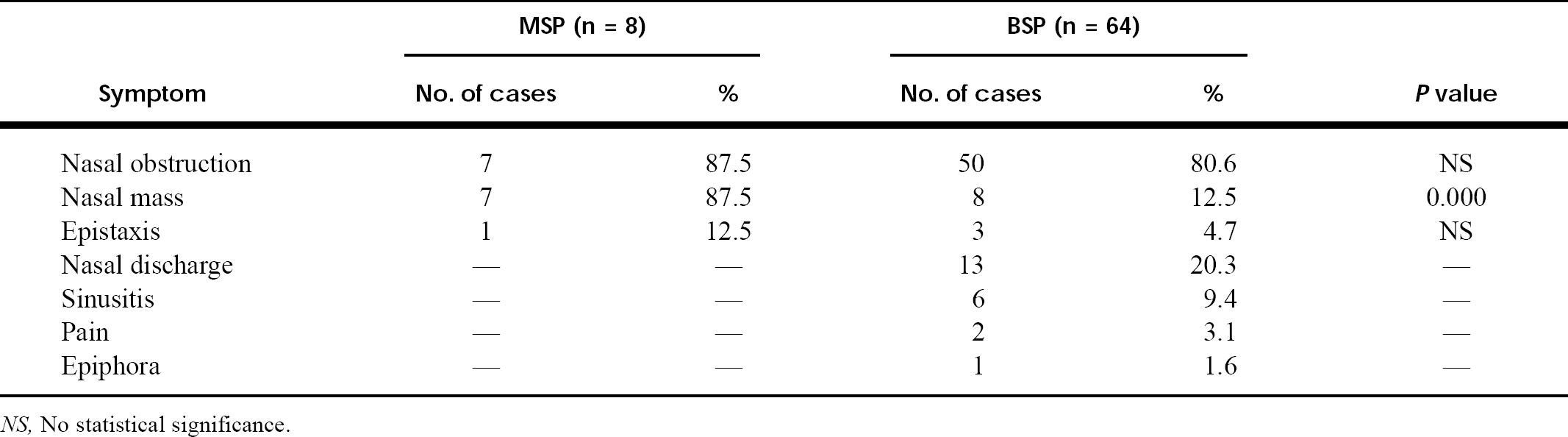
NS, No statistical significance.
Extent of tumor involvement in 72 SP patients ∗
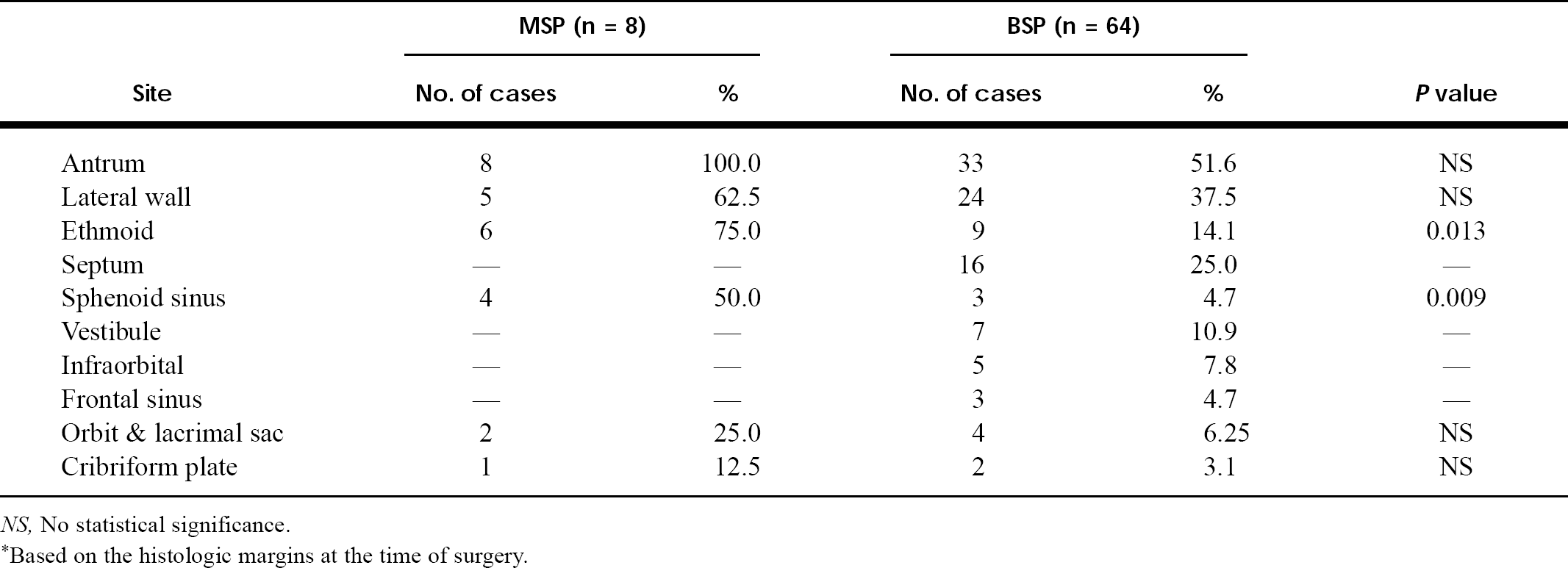
NS, No statistical significance.
∗Based on the histologic margins at the time of surgery.
Histologic characteristics of 72 SP patients
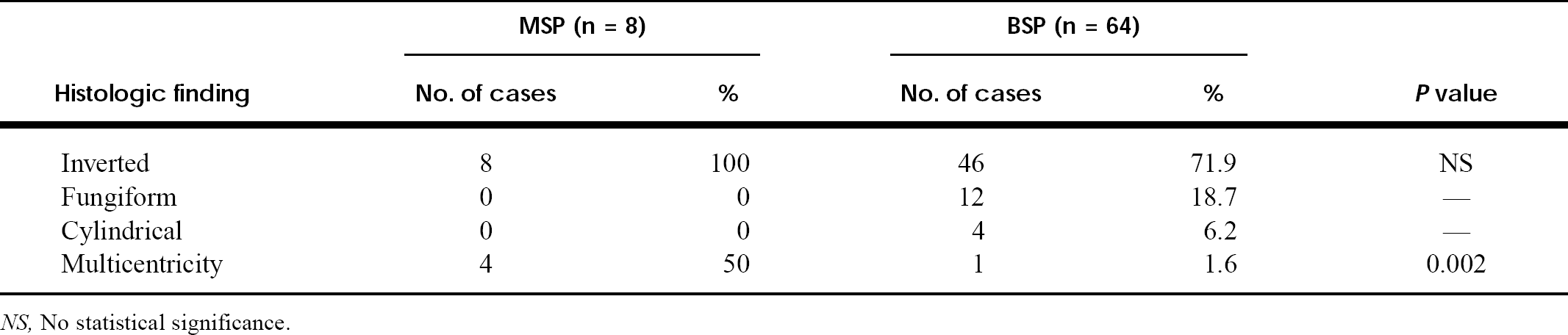
NS, No statistical significance.
The highlights of the follow-up and outcome of the 8 MSP patients are presented in table 5.
DISCUSSION
SP is a locally aggressive tumor of the sinonasal tract. The cause of SP remains unconfirmed, with several Possible causes having been proposed. These include viral infection, chronic inflammation, allergic proliferation, and environmental carcinogen exposure.
Evidence linking industrial carcinogens to an increased risk of SP 15,16 did not appear to play a role in the current study because no evidence of exposure was noted in our patient Population. Although no link between smoking and the development of SP as a whole was found, the evidence in this study showed a significantly higher proportion of patients with a Positive smoking history in the MSP Population than in the BSP Population (75% versus 16%). A viral cause, specifically human papilloma virus, was Postulated as the cause of SP. 5,17 In particular, there appears to be an association between human papilloma virus types 6 and 11 in BSP, and types 16 and 18 in MSP. 6,18
Clinically, SP tends to present in the fifth to seventh decades of life, 19-21 with a markedly male predomi-nance, 6,22 which is consistent with results seen in this study. The incidence of MSP has been reported at between 2% and 56%. 6 The incidence in our Population was 11.1%. From the results presented in this study, cases of MSP have similar age distribution and male predominance to BSP.
According to several studies, 7,9,10,23 the most frequent symptom at the time of presentation for SP is nasal obstruction. Other symptoms include presence of a nasal mass, sinusitis, epistaxis, rhinorrhea, facial pain, epiphora, anosmia, paresthesia, diplopia, and headaches. 7,10,19,24 In our study nasal obstruction was the most common presenting symptom for MSP as well as BSP cases, with the second most common symptom being the presence of a unilateral nasal mass. The presence of a nasal mass was significantly more frequent in the MSP group than in the BSP group, 87.5% versus 12.5%. A unilateral Polypoid mass was found in two thirds of the cases. The finding of a unilateral Polyp in the presence of normal nasal mucosa on the contralateral side should therefore alert the physician to consider the diagnosis of SP. Inflammatory Polyps are more often bilateral, 25 although they share common symptoms. 26
SP typically arises from the lateral wall of the nasal cavity 6-9,19,22,23 and frequently extends to involve the paranasal sinuses, most often the maxillary and ethmoid sinuses. Other less common sites of SP involvement include the sphenoid sinus, frontal sinus, orbital structures, and nasal septum. 6,7,9,27 All the MSP patients in our study exhibited maxillary antrum involvement at the time of diagnosis, compared with 51.6% of BSP patients. This difference was not statistically significant. However, ethmoid and sphenoid involvement was significantly more frequent in MSP patients at the time of diagnosis than in BSP patients, as can be seen in table 2. From this, we suggest that attention be paid to lesions involving not only the maxillary sinus but also the ethmoid and sphenoid sinuses.
Recurrence rate by type of surgery
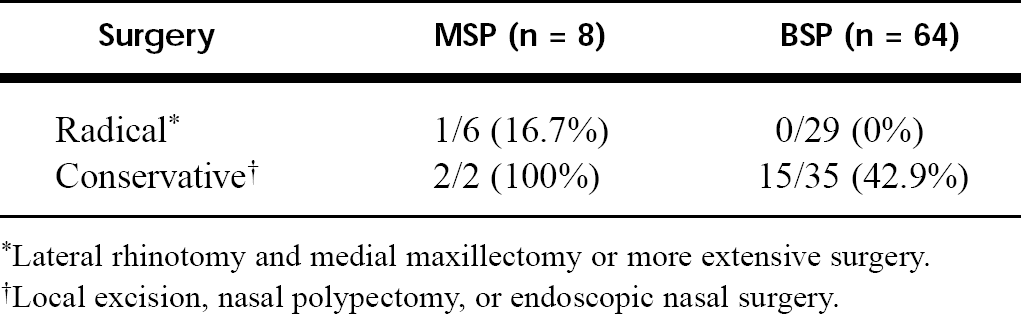
∗Lateral rhinotomy and medial maxillectomy or more extensive surgery.
†Local excision, nasal Polypectomy, or endoscopic nasal surgery.
Some authors 5,12,19,22 reported histologic multicentricity, defined as separate lesions not having mucosal or submucosal continuity, in 4% to 35% of SP cases. Our study found multicentric lesions in 5 (6.9%) patients overall, 4 with MSP and 1 with BSP. The difference was statistically significant (table 3). As such, multicentric lesions should raise suspicion of MSP.
The extent of surgery is a subject of great debate and controversy. Most authors believe that the treatment of choice is the achievement of wide surgical margins and that these should be obtained through lateral rhinotomy and medial maxillectomy. 8,9,11,24,28-30 The recurrence rate for SP has been reported in the literature to be between 28% and 74% 28,31 and has been attributed mostly to inadequate margin resection. Kristensen et al 9 reviewed the recurrence rates of several authors. They reported an average recurrence rate of 11% for patients treated with radical surgical excision, as compared with an average of 64% for patients treated with only limited excision. Our study showed a remarkable difference in both the BSP and MSP groups with respect to those treated conservatively, as compared with those treated aggressively, forwarding the premise of radical surgery. Several authors, including many of those favoring wide excision, also recommend the use of a more conservative limited resection in cases in which there appears to be limited disease. 6,9,11,23 Here, CT may help to identify those patients seemingly suitable for more conservative management. Blokmanis 32 and Kamel 33 recommended the use of a conservative endoscopic approach sparing the maxillary sinus in cases of small lesions of SP. It is the belief of some authors that recurrence of disease is a predisposing factor in the development of MSP, 9 whereas others refute this Point, 22 claiming it is the inadequate resection of the initial lesion that promotes recurrence. As such, in both of these scenarios, aggressive surgical management eradicating the disease process is preferable.
Our findings indicate that the relative risk for developing recurrence in MSP patients after radical surgery, such as lateral rhinotomy with medial maxillectomy, is only 14.3% of the risk after conservative surgery. Therefore it is our recommendation that the treatment of choice be aggressive surgical management.
Outcome of 8 patients with MSP
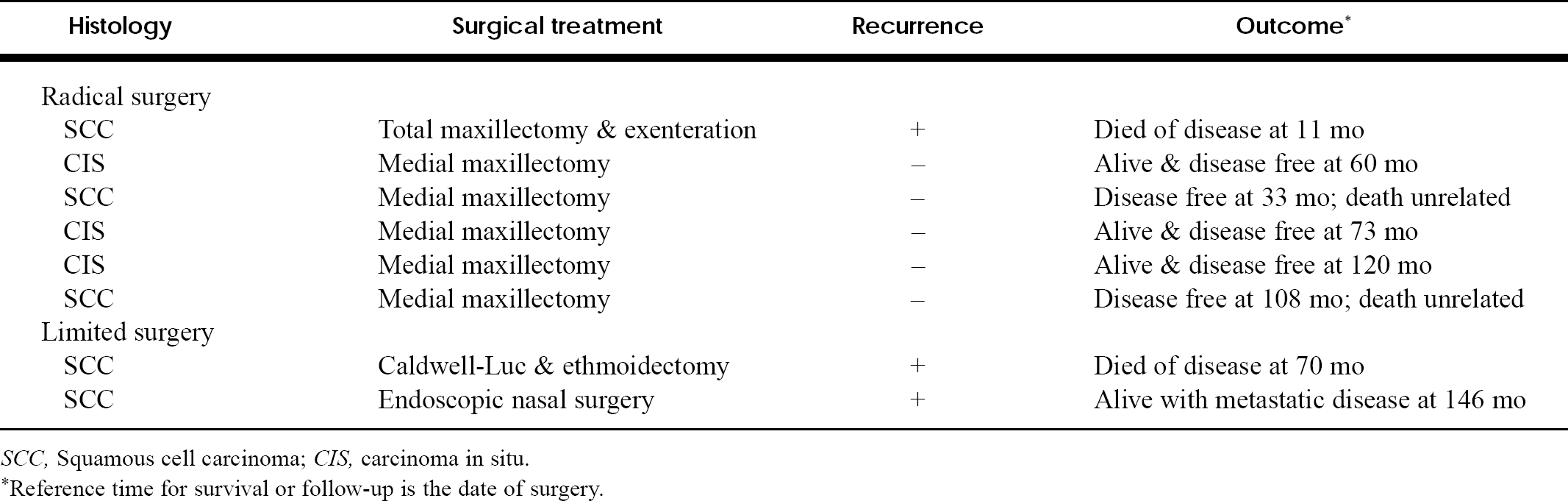
SCC, Squamous cell carcinoma; CIS, carcinoma in situ.
∗Reference time for survival or follow-up is the date of surgery.
With regard to pathologic characteristics, there are 3 subtypes of SP: inverted, fungiform, and cylindrical. The inverted type has an endophytic growth pattern, is found almost exclusively on the lateral nasal wall, 3 and accounts for approximately 47% of SP cases. 34 The fungiform subtype is an exophytic growing form of SP, has a frequency of 50%, and almost exclusively involves the septum. 34 The cylindrical type is the rarest form of SP, accounting for only 3% of cases and typically exhibiting an endoexophytic growth pattern most commonly involving the lateral nasal wall and maxillary sinus. 3,22,34 The most frequent subtype found in MSP patients is, according to several series, 9,35,36 the inverted subtype. This applied as well to our series because all of our patients had the inverted variant at presentation. The control group appeared less homogeneous and consisted of 71.9% with the inverted subtype, 18.7% accounted for by the fungiform type and 6.2% the cylindrical type. The difference was not statistically significant.
Long-term follow-up is of key importance in the management of SP. Many authors believe that most instances of recurrence occur within 2 years of the original excision. 27,31,37 However, several reports of recurrence more than 5 and 10 years after the initial treatment exist. 27,37 We believe that follow-up should occur at regular intervals for at least 5 years after surgical intervention. 30 This has important implications given the known association of SP and squamous cell carcinoma. Furthermore, we and other authors 23,33 believe that the role of endoscopy in initial treatment is limited. However, this modality proved to be an effective technique for staging of the original disease, as well as for monitoring disease recurrence and managing Postoperative complications. As such, we recommend regular endoscopic examinations of Postoperative patients in conjunction with follow-up visits.
CONCLUSION
SPs are nasal and paranasal sinus tumors that act locally aggressive. They are most often benign, but a substantial proportion of these tumors are associated with malignant changes. Several characteristics may allude to this malignant variant, including a Positive smoking history, report of a nasal mass, ethmoid and sphenoid sinus involvement, and histologic multicentricity.
Treatment should center on aggressive surgical management with lateral rhinotomy and medial maxillectomy. Long-term follow-up is an intrinsic part of the management of this disease.
We gratefully acknowledge Dr Ian Shrier from the Department of Epidemiology, Sir Mortimer B. Davis-Jewish General Hospital, Montreal, for assistance in the statistical analysis.
Footnotes
Microscope- and Endoscope-assisted Paranasal Sinus Surgery
This international preparation course will be held February 17-19, 2000. The professor and chairman is H. Rudert, MD, Department of Otorhinolaryngology-Head and Neck Surgery and the professor and co-chairman is B. Tillmann, MD, Center of Clinical Anatomy, Department of Anatomy.
For further information, contact Mrs Sabine Eickemeyer, Department of ORL-HNS, University of Kiel, Arnold-Heller-Straße 14, 24105 Kiel, Germany; phone 49-431-597-2242; fax 49-431-597-2272; e-mail,