
Abstract
The purpose of this study was to analyze mandibular fracture site, relationship of the fracture line to the periodontium, vitality of teeth, displacement of the fracture segments and their implications, and determine whether to retain or remove the teeth in the fracture line. Fifty patients with 62 fractures were involved in this study. An electric pulp tester was used to measure the pulpal response. The degree of fracture displacement and the relationship of the fracture line to the periodontium were evaluated using panoramic radiographs. Fractures of the parasymphysis region constituted a majority of 60.87% in the gross displacement category. Four of 50 patients showed no response presurgically and minimal response postoperatively on pulp vitality testing. Patients with teeth in the fracture line showing no response on pulp vitality testing should be advised extraction to avoid further complications.
Many factors precipitate fractures occurring in the mandible although it is the heaviest and the strongest facial bone.1 The pattern and displacement of fracture depend on the amount of force, soft tissue involvement, bone density, direction of muscle pull, and vulnerable areas that represent weak anatomic structures.2 Such fractures present with pain, edema, hematoma, derangement of occlusion, displacement and mobility of the fracture segments, facial asymmetry, and disturbance in phonation.3
Injury to teeth in the fracture line may compound the fracture even more if the injury involves the periodontium.456 Injury to such teeth can result in their avulsion, subluxation, root fracture, nonvitality, and varied pathology, all of which may interfere with or complicate healing.7
The influence of teeth in a fracture line on infection is not easy to determine due to interaction with other factors.8 Root fractures, periodontal pathology near the fracture line, functionless teeth, and vertical tooth fracture are all recommended for extraction.9 The purpose of this study was to evaluate teeth in the line of fracture, clinically and radiographically, and their associated complications so as to indicate if they should be retained or removed.
Materials and Methods
The study was performed in the Department of Oral and Maxillofacial Surgery, Vinayaka Mission's Sankarachariyar Dental College, and included a group of patients with mandibular fracture in the dentate region. The sites of fractures in the mandible included symphysis, parasymphysis, body, and angle (Figs. 1 and 2) and excluded condylar fractures, all of which were treated with open reduction and internal fixation under general anesthesia.
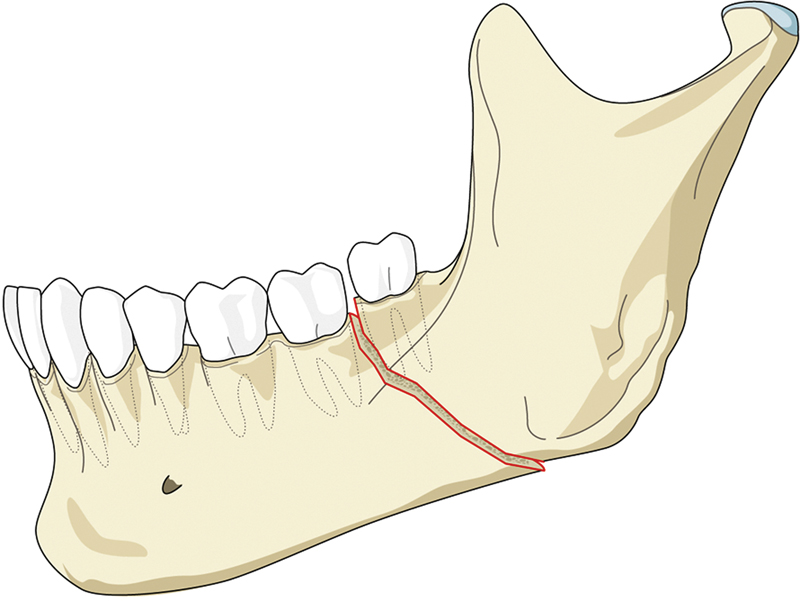
Mandibular fracture—lateral view.
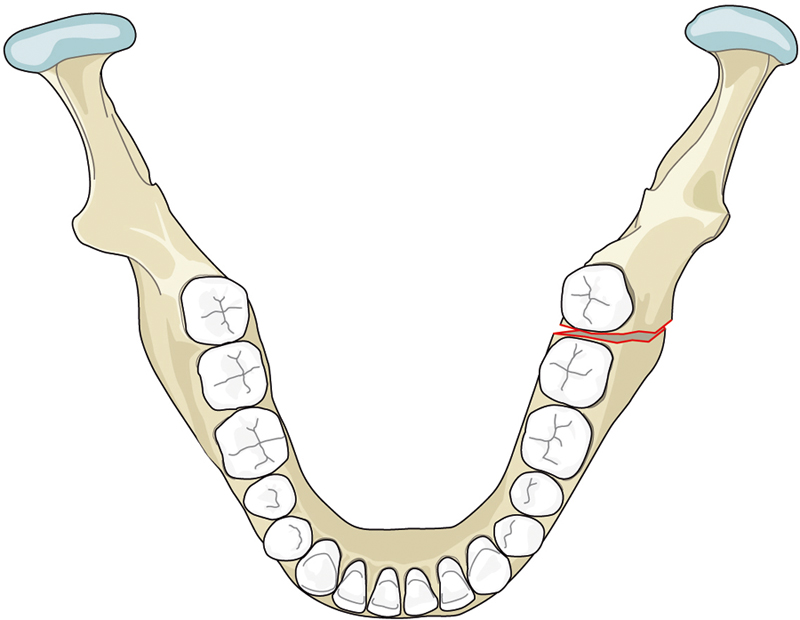
Mandibular fracture—occlusal view.
On these criteria, 50 patients from 2006 to 2008 were selected for this study. The postoperative follow-up period was 14 to 18 months with a mean of 16 months. The data collected from the patients included preoperative and postoperative radiographs, which included panoramic radiographs (Figs. 3 and 4); age at the time of injury; sex; cause of trauma; and site and type of fracture. The age of the patients ranged from 18 to 48 years with a mean of 29 years. In total, 62 fractures occurred in 50 patients. Treatment modalities included open reduction and internal fixation with conventional stainless steel81011 miniplates (2.5 mm, four holes/six holes), stainless steel three-dimensional plates (2 mm, four holes/six holes), and titanium three-dimensional plates (2 mm, four holes) with 6- and 8-mm stainless steel and titanium screws, respectively. Maxillomandibular fixation was used only intraoperatively to help in achieving occlusion.131415
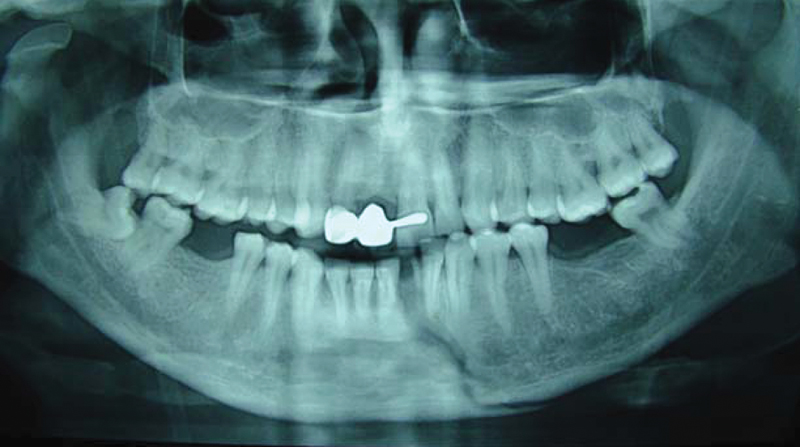
Orthopantomogram revealing a parasymphysis fracture of the left side.

Orthopantomogram revealing an angle fracture of the right side.
Patients were administered intravenous ampicillin (Ampoxin, Unichem Laboratories, India) 500 mg, metronidazole (Flagyl, Piramal Healthcare, India) 400 mg, and intramuscular diclofenac sodium (Voveran, Novartis India Ltd, India) 50 mg postoperatively, which varied between 5 and 7 days. They were also prescribed an antiseptic mouthwash (Clohex 0.2%, Dr. Reddy's Laboratories, India) chlorhexidine for a week's time.
All patients were divided into different groups based on four categories:
Anatomic location of the fracture
Degree of displacement of fracture7
Hairline (no displacement) Minimal (1 to 2 mm) Gross (>2 mm)
Position of fracture in relation to the apical foramen and the lateral periodontium of the involved tooth into four groups (Fig. 5)
Involving lateral and apical fibers completely Involving three-quarters of the lateral fibers Involving apical fibers completely Involving apical one-third of lateral fibers bilaterally
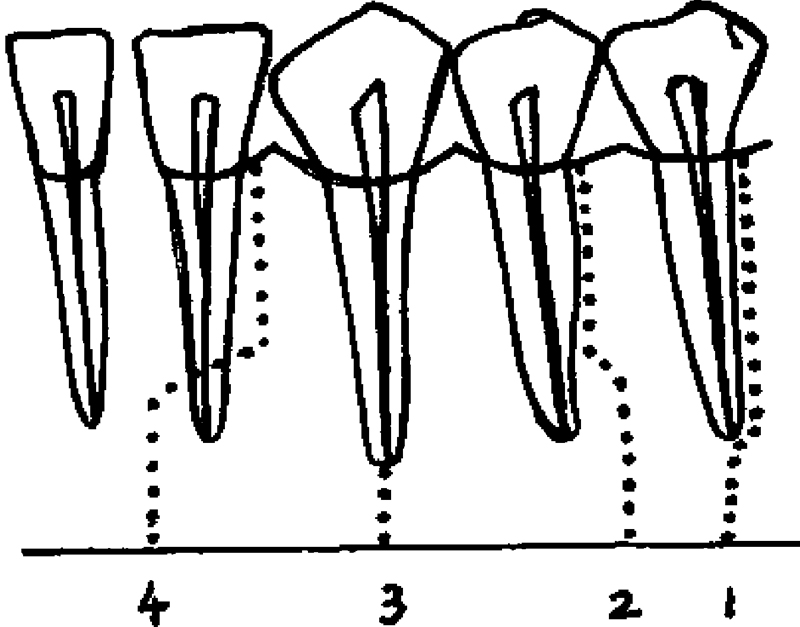
Relationship of fracture line to the periodontium categorized into four groups.
Pulp vitality testing with the help of C-PULSE pulp tester (Foshan Coxo Medical Instrument Co. Ltd, China) (Fig. 6) was done preoperatively and postoperatively at regular follow-up intervals of 1, 2, 4, and 6 months consecutively. It was done in the mandibular teeth, and teeth not in direct line of fracture were taken as controls. Maxillary teeth were taken as controls in patients who had bilateral mandibular fractures. The teeth taken as controls showed good response, and there was no change in vitality during the follow-up.
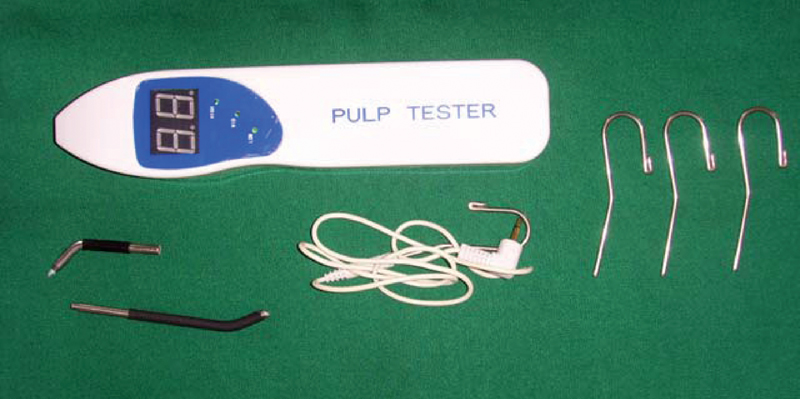
Electric pulp tester C-PULSE used for pulp vitality testing of the teeth in the line of fracture.
Results
Mandibular fractures occurred more frequently in males (96%) than females (4%). Anatomic location of fractures included 10% in the symphysis region, 52% in the parasymphysis, 11% in the body, and 27% in the angle region (Fig. 7). There were 13 cases of type 2 fractures in the parasymphysis region based on the relationship of the fracture line to the periodontium, which constituted 68.42% (Fig. 8). Type 1 was the most severe type and included 8.33% in the symphysis region, 41.67% in the parasymphysis, 12.5% in the body, and 37.5% in the angle region. Parasymphysis fractures constituted the majority with 60.87% in the gross category, 48.48% in the minimal category, and 42.86% in the hairline category (Fig. 9).
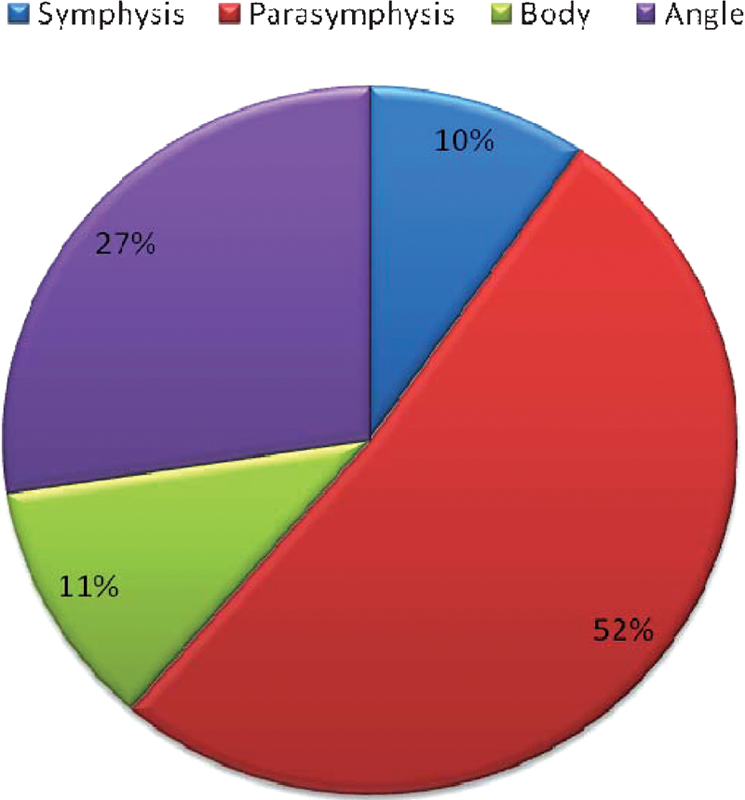
Percentage of fractures based on the anatomic site of occurrence.
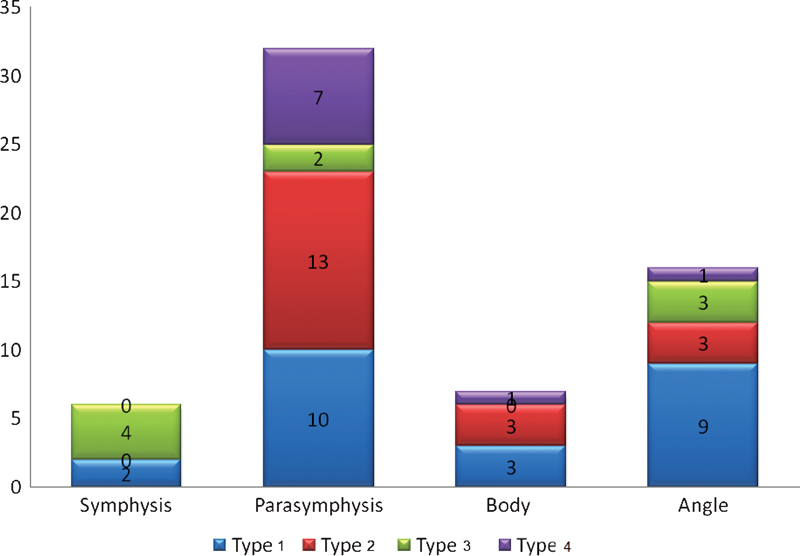
Relation between the fractures occurring in different sites to the periodontium.
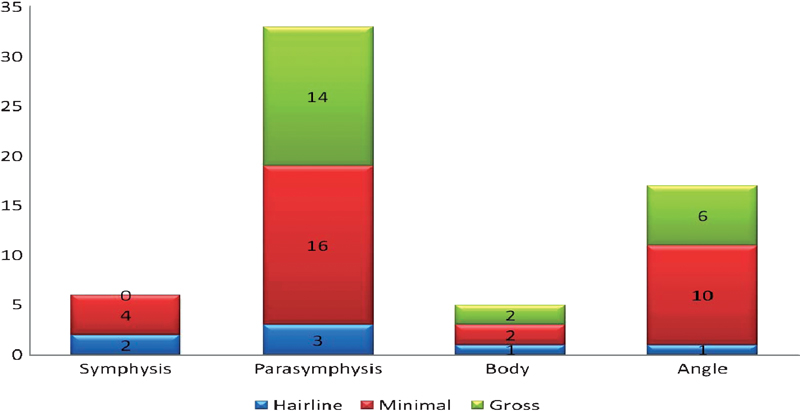
Degree of displacement of fractures subdivided into three groups.
On testing the pulp vitality, 4 of 50 patients (Fig. 10) presented with no response in the teeth in the fracture line presurgically (Table 1). Three patients had their teeth in the fracture line extracted between 4 and 6 weeks after surgery as the fracture sites were infected. One patient reported with infection in relation to the fracture line after 1 year. The teeth in the fracture line that had no response included three patients with mandibular third molars and one patient with mandibular lateral incisor (Fig. 11).
Patient Demographics
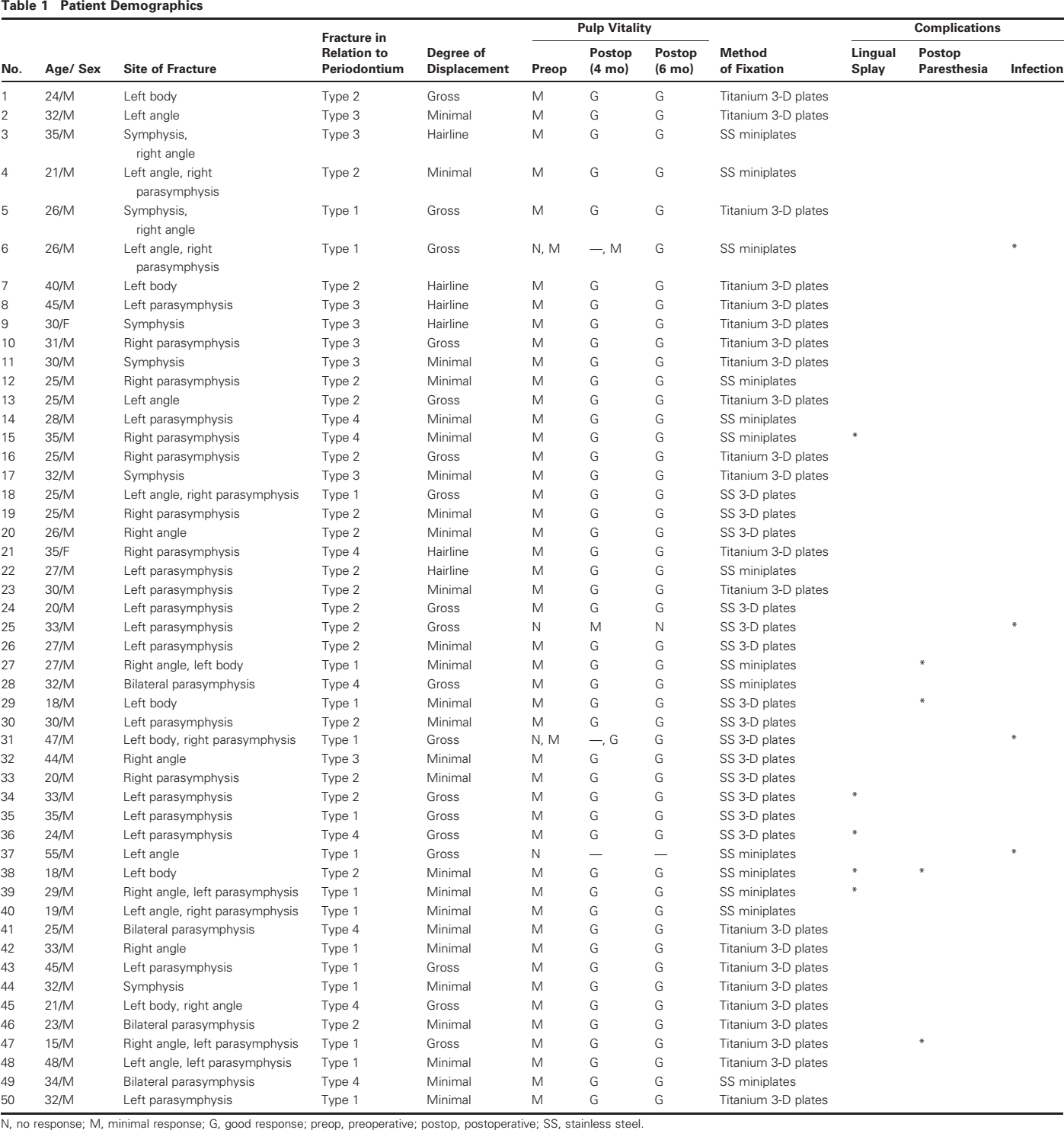
N, no response; M, minimal response; G, good response; preop, preoperative; postop, postoperative; SS, stainless steel.
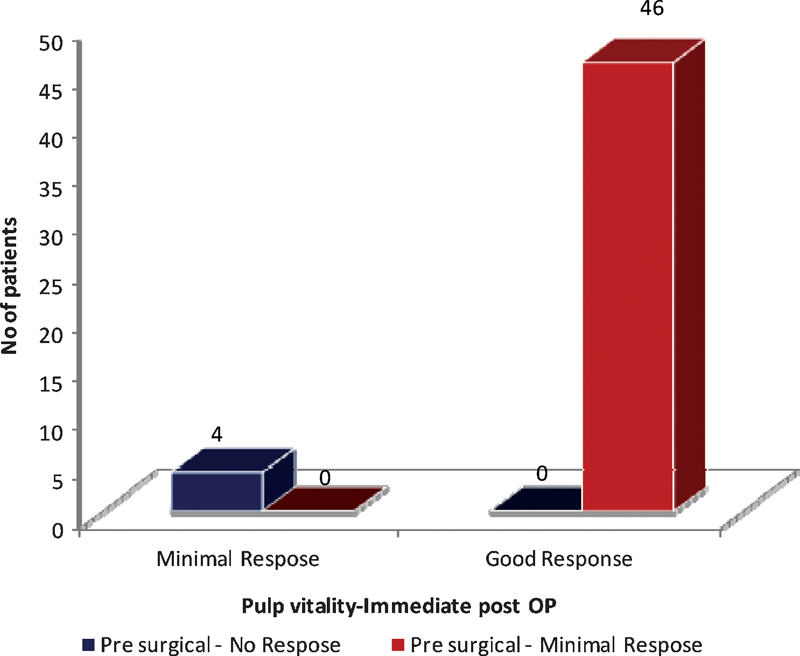
Pulp vitality responses in presurgical and immediate postoperative (post OP) stages.
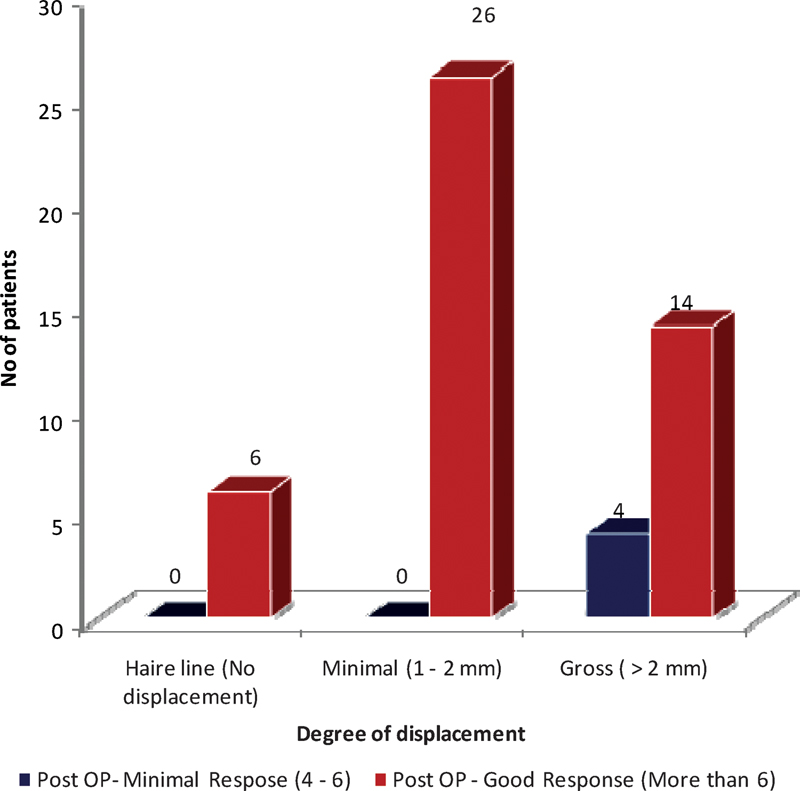
Relationship of the degree of displacement of fracture to pulp vitality response in immediate postoperative (post OP) stage.
The association between responses with reference to presurgical and immediate postoperative response was also analyzed using chi-square test at 5% level of significance, and the results are given with the following bivariate in Table 2 (p < 0.01; hence the result is highly significant—i.e., significant at 1% and 5% level). From the analysis, it is concluded that there is close relationship between the presurgical response and immediate postoperative response. Hence it is concluded that the majority of patients (92%) who showed minimal response presurgically (Table 3) showed good response immediately after surgery (Table 4). Those who had no response presurgically showed only minimal response immediately after surgery.
Pulp Vitality Responses in Presurgical and Immediate Postoperative Stages
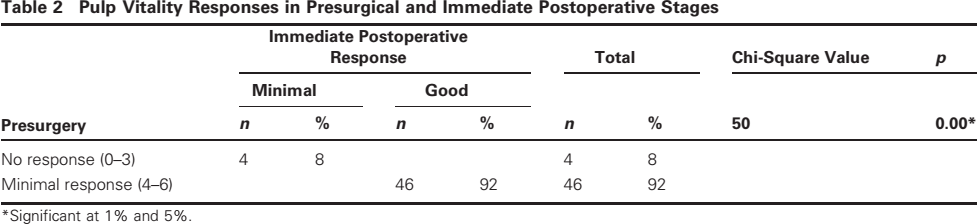
Significant at 1% and 5%.
Relationship of the Degree of Displacement of Fracture to Presurgical Pulp Vitality
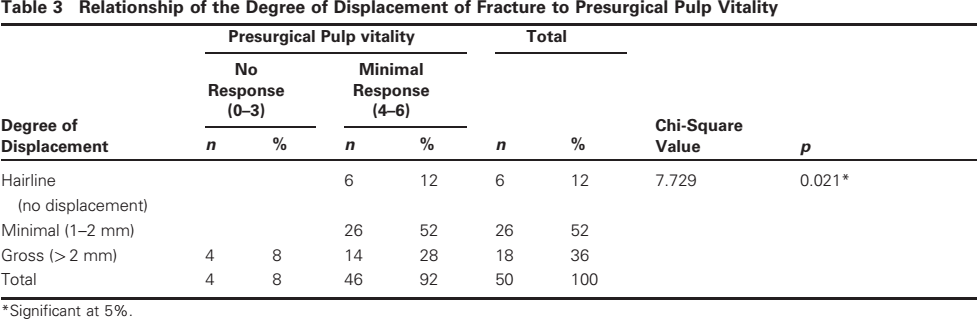
Significant at 5%.
Relationship of the Degree of Displacement of Fracture to Pulp Vitality Response in Immediate Postoperative Stage
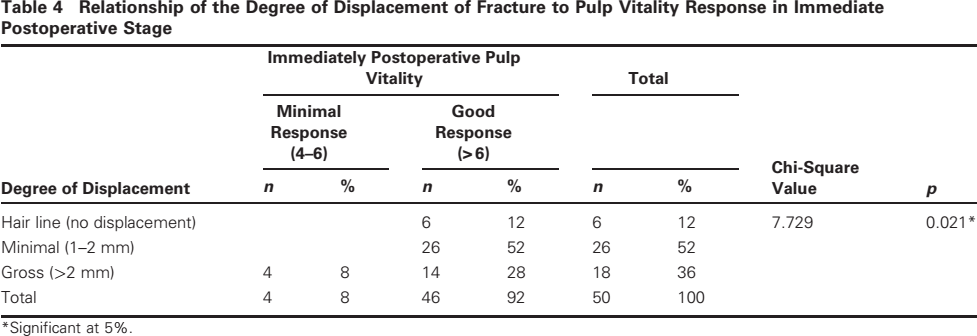
Significant at 5%.
Discussion
Correct repositioning of fractured fragments is made quicker and easier if the tooth in the line of fracture is conservatively managed. The teeth provide occlusal reference and posterior stop. They have a stabilizing effect and do not impede bone healing. If extracted, they increase the risk of fracture contamination and may sometimes be difficult to suture.16
Pulp changes like pulp fibrosis and acute pulpitis may be noted in teeth that respond to electronic pulp tester. The loss of vitality may also be reversible as vascular and neural recoveries are possible. The follow-up of ∼1 year would be sufficient for the return of temporary loss of vitality as suggested by Kahnberg and Ridell.7 In our study, all patients were followed to 18 months. The vitality of teeth improved in all patients except four for whom the teeth in the fracture line were extracted as they reported with infections.
The disposition and the presence of teeth do not directly influence complications but are influenced by the anatomic location of the fracture.17 In our study, extractions of third molars were performed as they got infected and one patient had his plate removed. One likely reason for nonvitality nearer to fracture line can be the presence of screws used for fixation of fractures. The number of screws can be limited if and when the fractures are fixed using three-dimensional plates.12
The fracture displacement showed some significance in determining pulp vitality. Fractures with gross displacement had pulp vitality with no response in the presurgical stage. In comparison, hairline fractures did not influence pulp vitality.
Extractions of teeth in the line of fractures in a few cases tend to displace the fracture segments. However, after the analysis, it was proved that a tooth in the fracture line showing no response in the presurgical stage resulted in infection of the fracture site. Hence, in such cases, it would be appropriate to proceed with extraction of such teeth followed by the management of fractures.
Conclusion
In conclusion, according to our study, a tooth that shows no response on pulp vitality testing should be advised for extraction to avoid further complications in patients presenting with mandibular fracture.