
Abstract
Knowledge of the branching pattern of the mental nerve is an important consideration during placement of tooth implants and reconstructive plates. It is known to display population variations and data for the same is scarce form the sub-Saharan region. With the recent increase in surgical interventions in the mandibular region in Kenya, a detailed description of mental nerve is warranted. A total of 64 mental nerves were dissected and branching pattern was noted. Single mental nerve was present in 60 (93.7%) cadavers while double mental nerves occurred in 3 (4.7%) and accessory in 1(1.6%). Most common pattern was bifurcation (39%) followed by trifurcation (34%), single (19%), and quadrification (8%). The double and triple branches were seen to further divide into two to three subbranches with diverse patterns. Side symmetry in branching was seen in four (6.25%). These are important anatomical considerations during placement of reconstructive plates for mandibular trauma and administration of mental nerve blocks.
Keywords
The mental nerve (MN), terminal branch of the inferior alveolar nerve, exits the mental foramen (MF)1 and divides into three branches to innervate the skin of chin, lower lip, and gingivae.2 The number of MNs on the ipsilateral side varies from none to four with the most common variation being two.34567 Branches of the MN vary from one to four,89 with the most common being four branches, namely medial, lateral inferior labial, angular, and mental.10 These data are, however, mainly in form of case reports, hence the true incidence of such occurrences is difficult to establish. A detailed description regarding the exact branching pattern is important for effective presurgical evaluations in implant surgery, administration of MN block anesthesia, and for osteotomy procedures.11 Surgical interventions involving the mandibular region have increased in the past decade.12 The branching pattern displays population differences.9 There is however no data for the black Kenyan population. The aim of this study was, therefore, to clearly elucidate the branching pattern of the MN in Kenyans to minimize iatrogenic injuries during surgical maneuvers.
Materials and Methods
A total of 64 MNs were dissected at the Department of Human Anatomy, University of Nairobi. All the specimens were from adult black Kenyan. The MN was exposed by three skin incisions and lateral reflection of the skin flap. A midline incision extended from the midpoint of the superior border of the lower lip to the midpoint of the inferior border of the mental symphysis (MS). A lateral incision extended approximately 7 cm from the angle of the lip on either side. An inferior incision was made along the lower border of the mandible from the MS till the lateral extent of the lateral incision. Using blunt dissection, the flap was detached from the bone and reflected laterally until the MN was seen to exit from the MF. The MN was carefully dissected and the branching pattern was carefully displayed. Data collected included the number of MNs, initial branching pattern, terminal branching pattern, and symmetrical branching patterns. A branching pattern was classified as high or low depending on whether the MN branched at the level of the MF or at a distance from the MF, respectively. The data collected was analyzed using Microsoft Excel 2007 (Microsoft Corporation, Redmond, WA). The frequencies and percentages of the various branching patterns were determined. The variations noted were photographed using a high resolution digital camera and managed using Photoscape version 3.5 (MOO11 Tech, Korea).
Results
The MN was present in all cadavers that were dissected. The pattern of branching of the MN after its exit from the MF displayed diverse set of variations in the number and branching pattern. A single MN was present in 60 cadavers (93.7%) while double MNs occurred in 3 (4.7%) (Fig. 1A, B) and accessory in 1 (1.6%) (Fig. 1C). The accessory MN emerged in the region of the second premolar, 4 mm from the MN. When the inferior alveolar nerve branched into two terminal branches which were of similar sizes, the pattern of branching was described as double MNs. Accessory MNs were smaller branches from the inferior alveolar nerve in addition to the MN that had the same area of innervations as the MN.
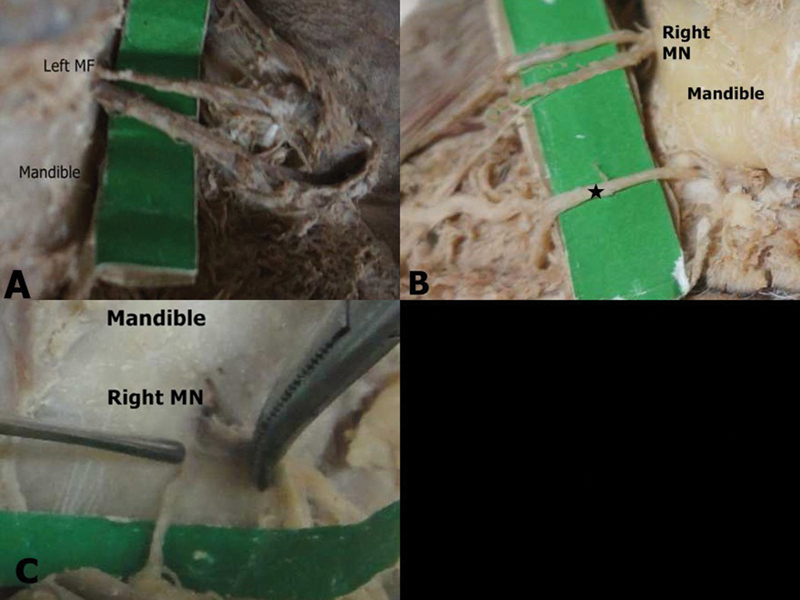
Macrographs showing double and accessory mental nerves (MNs). (A) Double MN arising from the left mental foramen (MF). (B) Double MN on the right side with aberrant origin. Whereas, the second MN was seen to arise from an aberrant position (star), the superior MN emerged from the MF before dividing into two branches. (C) Accessory MN on the right side arising from an accessory MF. The two MF were in close proximity being separated by a distance of only 4 mm. Note that, unlike the main MN, the accessory was not seen to further divide into smaller branches.
Initial Branching Pattern
The MN displayed a varied branching pattern with the number of branches varying from one to four on the ipsilateral side. The most common pattern of branching was division of the MN into two branches (39%) which displayed a high level division, that is, branching at the level of the MF in 11% (Fig. 2A) while in 28%, the branching was seen at a distance from the MF hence a low division branching pattern (Fig. 2B). The MN split into three branches in 34% (Fig. 2C), continued its course as a single nerve without splitting into any branches in 19% (Fig. 2D). In 8% of the cadavers, a quadruple division was observed (Fig. 2E).
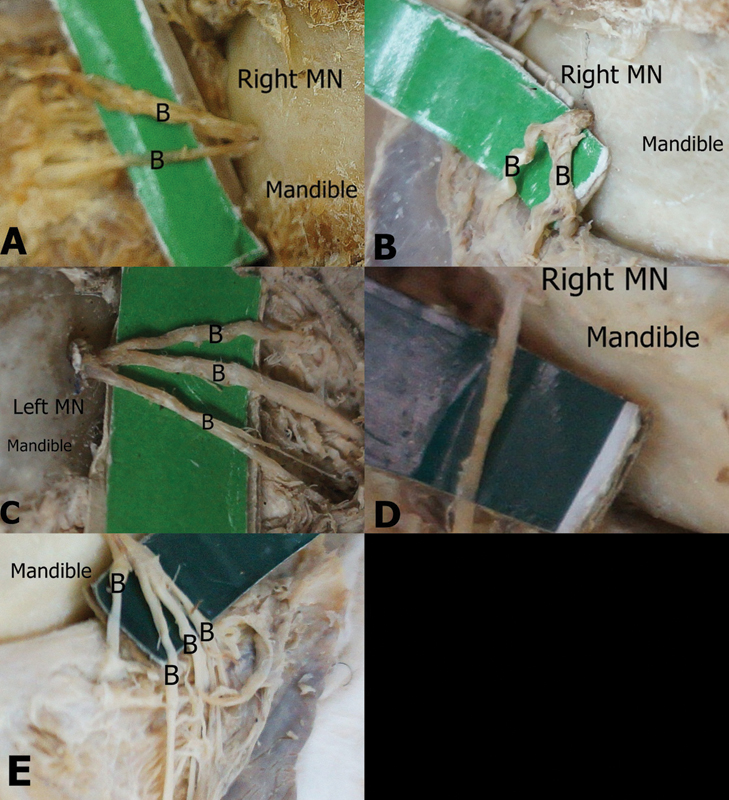
Macrographs showing the initial branching pattern of the mental nerve (MN). (A) Right MN dividing into two separate branches (B) at the mental foramen (MF). Note the high level of division where single MN divides into two branches as it exits the MF. (B) Right MN emerging as a single branch and then dividing into two branches at a distance from the MF. Note that the two branches arise from a common point at the MN. Note also that the two branches do not further divide into smaller branches but continue as single branches to their respective areas of distribution. (C) Left MN dividing into three separate branches after its exit from the MF. The branches continued to their respective areas of distribution without further division. (D) Right MN emerging as a single branch. Note that the single branch continues to its area of distribution without dividing into further branches. (E) Left MN seen to divide into four branches after emergence from the MF.
Terminal Branching Pattern
The double and triple branches of the MN further exhibit a diverse pattern of division into subbranches. For the double branches, the most commonly observed redivision pattern was seen in 12.7%, where each of the two main branches of the MN further divided into two smaller branches (Fig. 3A), hence a total of four subbranches arising from the two branches of the MN. In 7.8%, one of the two main branches of the MN further redivided into two smaller subbranches (Fig. 3B). In 1.56%, five subbranches were seen to arise from the two branches of the MN (Fig. 3C). About 9.1% of the triple branching patterns, divided further into two subbranches (Fig. 3D) while in 1.56%, four subbranches were observed (Fig. 3E).

Macrographs showing the terminal branching pattern of the mental nerve (MN). (A) Left MN dividing into two branches (B) which further divides into four smaller branches (arrows). (B) Two branches of the left MN dividing further into two subbranches (arrows). In this case, it is the right branch, which further divides into two subbranches (arrows). (C) MN with two branches and five subbranches (arrows). The left branch divided into three subbranches (arrows) while the right branch divided into two subbranches (arrows) and hence five subbranches in total were seen to arise from this double branch division of the MN. (D) Left MN with three branches and two subbranches (arrows). Note that it is the middle branch which further divides into two subbranches (arrows). (E) Right MN with three separate branches and four subbranches (arrows). The left and middle branches each divide further into two subbranches (arrows). Note that the left branch does not give rise to any subbranches unlike the other two.
Symmetry
Significantly high levels of side asymmetry were observed in the same cadaver. Symmetrical branching pattern was observed in only 6.25% of the cadavers (Fig. 4A, B). In 3.125%, the MN continued as a single branch on both the right and left side on the same cadaver (Fig. 4A). Similarly, for another 3.125% of the cases, it split into the triple branch presentation on both the right and the left sides of the same cadaver (Fig. 4B).
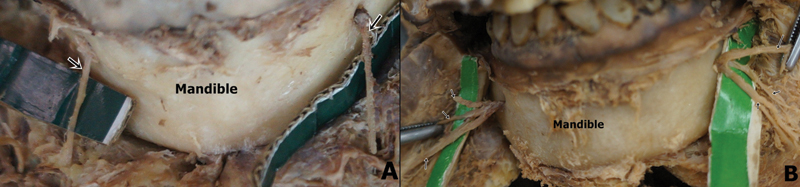
Macrographs displaying the symmetry in branching pattern of the mental nerve (MN). (A) MN (arrows) arising as a single branch from both the left and right mental foramen. Note that in either case, the MN is not seen to further divide into smaller branches. (B) MN dividing into three branches (arrows) on both the right and left sides after its exit from the mental foramen.
Discussion
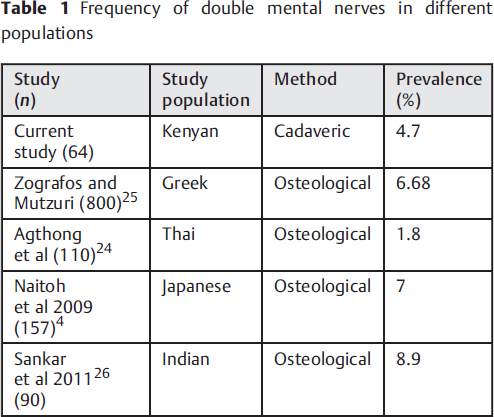
The MN was present in all the 64 hemifaces, which is at variance with previous studies that have reported unilateral and bilateral absences.13 The prevalence of double MNs in the current study (4.7%) falls in the range of 1 to 10.6% reported in the previous studies.414 It is, nonetheless higher than that reported for the Thai population but lower than in Greeks, Indian, and Japanese population (Table 1). This suggests wide population differences. Separation of the MN earlier than the formation of the MF is a likely explanation for the presence of variations in the number of nerves.4 The presence of additional MNs has been associated with failed mandibular anesthesia.15 There are currently no studies done on the failure rates of complete mandibular anesthesia in the sub-Saharan region, but these results suggest a lower rate for Kenyans compared with the Greek, Indian, and Japanese population (Table 1).
Frequency of double mental nerves in different populations
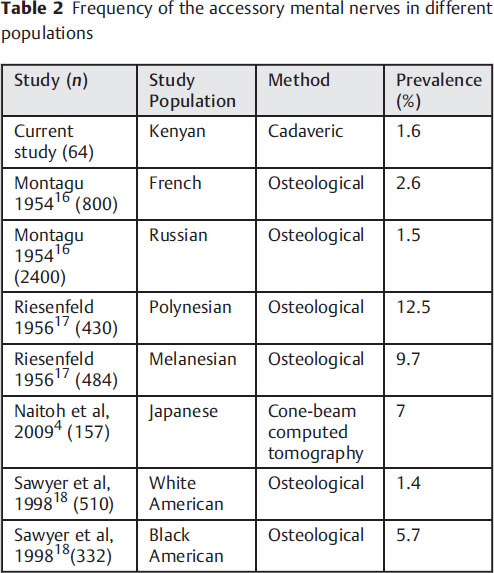
Knowledge of the prevalence of accessory MNs is important during the placement reconstruction plates for mandibular fractures and in screwing tooth implants as accessory MNs may be injured during these procedures.11 The 1.6%, prevalence of accessory MN is comparable to that seen in the Russian and White American population (Table 2). It is however, lower than that reported for Polynesian, Melanesian, Japanese, and Black American population. This suggests wide population differences. The discrepancies observed could also be attributed to the differing sample sizes and to the different study methods whereby dry mandibles161718 or cone beam computed tomography4 and cadaveric dissection (current study) were used.
Frequency of the accessory mental nerves in different populations
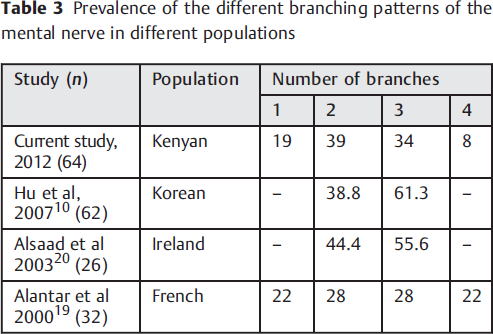
The current results confirmed the previous descriptions of the MN dividing into one to four branches (Table 3). The classic description of division into three branches was only seen in 34% of the cadavers. The most commonly observed branching pattern was division into two branches. These results are at variance with those reported by previous studies where the most commonly observed pattern is division into three main branches.101920 The MN divided into four branches in 8% and continued as a single branch 19%. This is lower when compared with the prevalence reported by a French study, at 22% for each branding pattern.19
Prevalence of the different branching patterns of the mental nerve in different populations
It is important to know the branching pattern of the MN since accessory branches can be used for facial nerve grafting. This diverse pattern of branching needs to be considered before biopsy of minor salivary glands, excision of nodules symphyseal bone procedures through the labial route. Damage to the branches of the MN can lead to labiomental sensory disturbances which produce severe discomfort.19 Knowledge of variant branching patterns could be of help in explaining failed MN anesthesia21 and also referred pain to teeth during cases of injury to any of the cutaneous branches. The branching pattern of the MN becomes an important surgical considerate in sliding horizontal osteotomy procedures of the mentum during genioplasties. The MN is also vulnerable to iatrogenic injury during procedures involving placement of alloplastic implants, in horizontal advancement osteotomy also during bone grafting to correct microgenic mandible.22
The branching pattern further becomes relevant during MN transpositioning and repositioning in mandible endosteal reconstruction implant surgeries. This is a difficult surgical procedure where the anatomy of the MN often challenges the surgeon during replacement of removable prosthetics, stabilizing the anterior residual dentition, and reducing alveolar ride atrophy.23
In the current study, only 6.25% of the MNs exhibited the same branching pattern bilaterally compared with a French study19 where 56% homogeneity in branching pattern was observed. This finding has important implications during surgical interventions where side consideration becomes an important factor in avoiding nerve injury. The branching pattern on the right and left side should not be treated in the same way during surgical maneuvers in the area.
Conclusion
Double and accessory MNs were present in 6.3%. The diverse hierarchical pattern of branching of the MN and the high level of asymmetrical branching are important anatomical considerations during placement of reconstructive plates for mandibular trauma and administration of MN blocks.