
Abstract
Jacob disease is a rare entity consisting of the formation of a pseudojoint between the inner surface of the zygoma and the coronoid process. This requires constant contact between the two implicated surfaces. It can be achieved by two mechanisms: one by an enlarged coronoid process and two by an anterior displacement of the coronoid process caused by a temporomandibular joint (TMJ) disorder. Although von Langenbeck described coronoid process hyperplasia in 1853, Oscar Jacob was the first author to describe the pathology in 1899. Since then, only a few cases have been published in the literature. The authors report a rare case of Jacob disease caused by an osteochondroma of the coronoid process, which is even less common, and review the literature.
The osteochondroma is one of the most frequent tumors in the axial and appendicular skeleton, although it is uncommon in the maxillofacial area, and even less common in the coronoid process. This tumor grows slowly and when it is sited in the coronoid process, it causes progressive limitation of mouth opening, and facial asymmetry. Because masses in the coronoid process are rare, Jacob disease is often misdiagnosed and treated as a temporomandibular joint (TMJ) dysfunction or a pain syndrome.12
Case Report
A 42-year-old man was referred to our outpatient service with a suspected TMJ disorder. The patient suffered a 5 to 6 month history of progressively decreased mouth opening. He did not complain of pain or other symptoms. There was no history of blockages or dislocations of TMJ, neither previous trauma in the jaw. Physical examination showed a mechanic stop when the interincisal opening reached 20 mm. Facial asymmetry was observed, presenting swelling in the right zygomatic region and a 4-mm jaw deviation during opening toward the right side. Oral examination showed a class I interarch relation, and no open bite or other disocclusion was observed. The panoramic radiograph revealed an elongated right coronoid process. A computerized tomographic (CT) scan was performed which showed an exostosis of bony and cartilage density tissue from the lateral aspect of the coronoid process that contacted and remodeled the inner surface of zygomatic arch (Fig. 1).
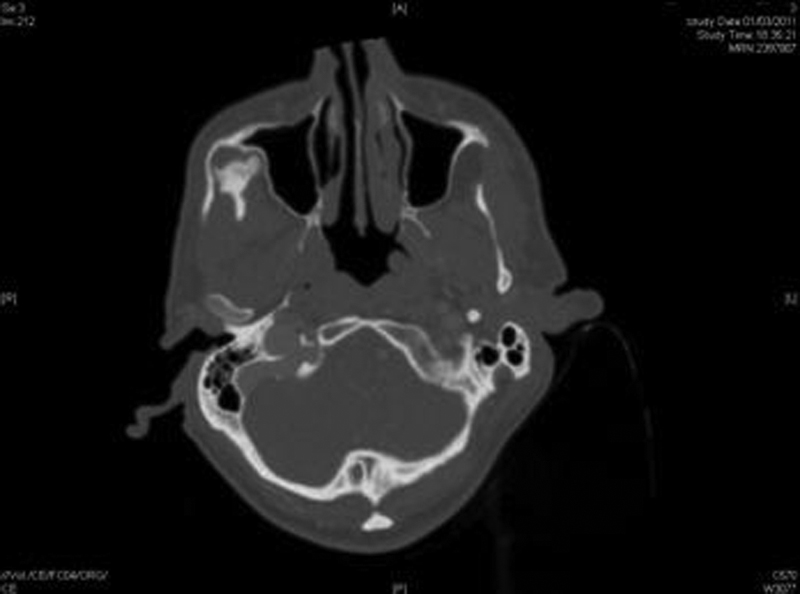
Computed tomographic scan (axial cuts) showing the mass from the coronoid process modeling the zygomatic arch.
The patient was surgically treated under general anesthesia and nasotracheal intubation. An intraoral approach was employed. The tumor was exposed, and we observed how the cartilage structure perfectly articulated with the inner surface of the zygomatic arch (Fig. 2). We performed an intraoral coronoidectomy (Fig. 3) and remodeled the external surface of the zygomatic arch to achieve facial symmetry.
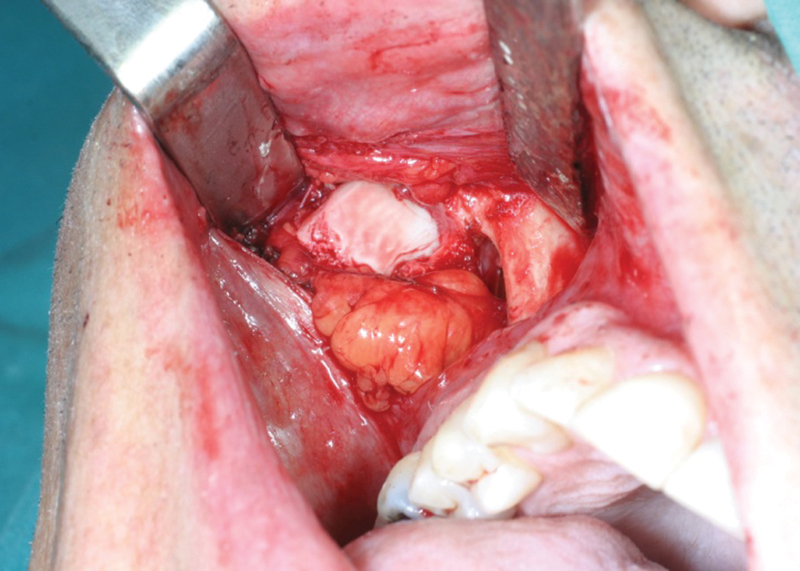
Intraoral approach showing the osteochondroma.

Osteochondroma depending on coronoid process.
In the immediate postoperative, the patient achieved a 45-mm maximum mouth opening capacity (Fig. 4). The histopathological exam revealed cartilaginous and osteoid tissue with few areas of fibrous tissue. They are the typical features of osteochondroma (Fig. 5). Now, the patient is asymptomatic, with a maximum mouth opening of 41 mm. The aesthetic is satisfactory, with minimal facial asymmetry.
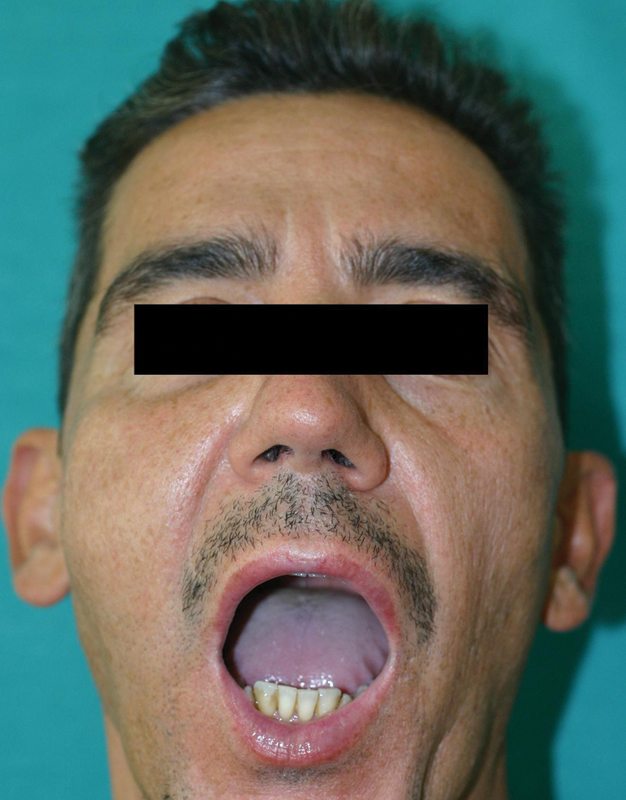
Maximum mouth opening immediately postoperative.

Histopathological exam revealed the typical features of osteochondroma: cartilaginous, bony, and fibrous elements irregularly arranged.
Discussion
Jacob disease is an uncommon pathology with few cases reported in the literature. There are different etiologic hypotheses, but none of them has been proved. The most popular are history of previous childhood trauma and hyperactivity of temporal muscle. This stimuli would be an hyperplasic inductor force to pluripotent cell of the periosteum.34
The disease courses with insidious clinical symptoms. Progressive reduction of the mouth opening over an extended period of months is the main symptom. Lateral deviation toward the affected side and increased ipsilateral malar swelling are frequently found. Pain and disocclusion are uncommon.5
Jacob disease due to osteochondroma of the coronoid process is even less frequent, and although extremely rare, bilateral cases have been reported in the literature.67 In 2011, Sreeramaneni et al published a summary with only 51 osteochondrome cases related to this disease after reviewing the international literature. This tumor appears to be slightly more common in males and in the left coronoid process.8
In the radiologic diagnosis, water's projection and panoramic radiography are useful, which can show an enlarged coronoid process. However, the gold standard test is three-dimensional CT9 because it provides anatomical details that allow us to plan the surgery (Fig. 6).10 Furthermore, the CT led us to suspect a diagnosis of osteochondroma because it has a typical radiologic image: a mass with bone and cartilage density areas. Definitive diagnosis is by histopathologic analysis.

Three-dimensional computed tomography showing the mass and pseudojoint.
The best treatment is to perform a coronoidectomy involving the tumor because it is a definitive one. Recurrences are rare if complete resection is achieved (2%).9 Intraoral, extraoral, or a combination of the two approaches can be used for the resection of the tumor. Other approaches are described in the literature according to the location and size of the lesion (bilateral coronal,1112 hemicoronal, transzygomatic,12 submandibular,13 Alkayat-Bramely14). Whenever possible, we prefer an intraoral approach, as it avoids facial scars and minimizes the risk of damage to the facial nerve. On the other hand, visualization may be limited by decreased mouth opening, and sometimes it is impossible to perform it when the trismus is severe.
Conclusion
Jacob disease is a rare pathology consisting of the formation of a pseudojoint between the inner surface of the zygoma and the coronoid process. A rare case of Jacob disease due to an osteochondroma of the coronoid process is presented. This disease should be suspected in patients presenting progressive limitation of mouth opening and facial asymmetry, while pain and disocclusion are less common. A three-dimensional CT is the gold standard for preoperative diagnosis, although the final diagnosis is the histopathologic analysis. The CT may be diagnostic in cases of osteochondroma, and may help plan the surgical treatment. Resection of the enlarged coronoid process or the coronoid osteochondroma is a definite treatment, with low recurrence risk. Whenever possible, we prefer an intraoral approach.