
Abstract
Subcranial approach is a useful procedure in the management of limited anterior skull base tumors. But the posterior and superior visualization may be limited, in ethmoid malignancies with a large intracranial extension. A 55-year-old male patient, a case of an ethmoid malignancy, with a large intracranial component was resected with adequate margins by a subcranial approach. The coincident pneumosinus dilatans helped the surgical resection. This case demonstrates that assessment of pneumatization of the frontal sinus is as important as the size and extent of the tumor, while deciding an anterior skull base surgical approach. Even large malignant lesions may be approached subcranially if the frontal sinus is proportionately large. Pneumosinus dilatans, though rare, can be used to the benefit of the patient in selecting a less invasive approach.
Keywords
Subcranial approach is a useful procedure in the management of limited anterior skull base tumors. But the posterior and superior visualization may be limited, in ethmoid malignancies with a large intracranial extension. We report a case of an ethmoid malignancy, with a large intracranial component, that was resected with a subcranial approach. Although the patient had a significant intracranial part, the coincident pneumosinus dilatans (PSD) with enlarged frontal sinus helped the tumor removal, with adequate margins. The institutional review board has approved submission of this report.
Case Report
A 55-year-old male patient presented with multiple spontaneous episodes of bleeding from the left nostril and left nasal obstruction of 3 weeks duration. Endoscopy showed a pale red mass on either side of the nasal septum, predominantly on the left side. The preoperative biopsy was reported as sinonasal undifferentiated carcinoma. Magnetic resonance imaging showed an ill-defined enhancing soft tissue mass involving the anterior and posterior ethmoidal air cells, with close proximity to the posterior wall of the left frontal sinus. The lesion was extending to the extradural space with a breach in the dura of the frontal region. Neuroparenchyma appeared normal. The frontal and sphenoid sinuses were extensively pneumatized (Fig. 1a, b). The case was discussed in a multidisciplinary board and was decided for surgery followed by adjuvant radiation therapy. Endoscopic approach was not considered as the mass was large and there was a suspicion of dural involvement extending laterally above the orbit. Though the tumor was intracranial and extending close to the planum sphenoidale, an endoscope-assisted subcranial approach was planned, considering the extensive pneumatization of the frontal sinus. The patient underwent a complete resection of the tumor with adequate margins.
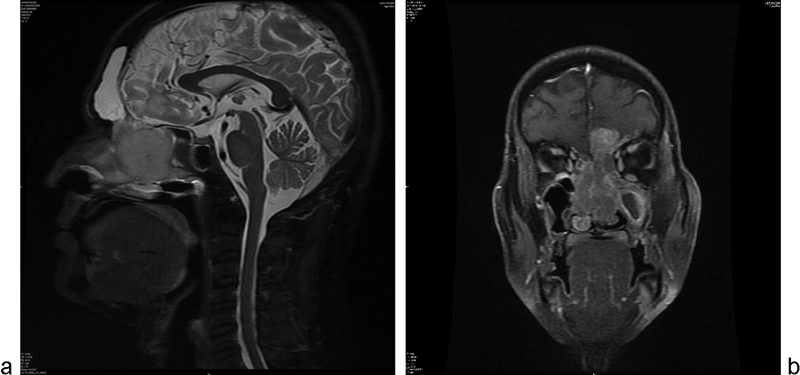
(a) Magnetic resonance imaging (MRI) scan, sagittal view showing the large frontal sinus and the tumor. (b) MRI scan, coronal view showing the intracranial extent of the tumor.
A bicoronal incision was done and the flap was elevated in a supragaleal surgical plane. Frontonasal bone was flap marked with the help of transmitted illumination (Fig. 2). A superiorly based vascularized bone flap was raised. Posterior table of frontal bone was then drilled and removed. The dura was exposed. The disease was seen going intradurally eroding the cribriform area (Fig. 3). Frontal pole on the left side was excised and approximately 0.5 cm of the brain around the tumor was excised sub piele. Then tumor was decompressed internally, separated all around, and the intracranial portion excised. The dura was incised with adequate margins. Posteriorly, the disease was seen about a centimeter anterior to the planum sphenoidale. The dura was incised all around with adequate margins. Bone cuts were taken at the lateral lamina of cribriform on both sides. Anterior and posterior bony cuts were completed. Lower cuts were taken endonasally using an endoscope. Central part of the tumor was debulked. Periorbita was seen uninvolved. A “lamina to lamina” resection was done endoscopically. Uncinectomy was done bilaterally; bilateral middle turbinates were also resected. Anterior wall of sphenoid sinus was opened. Anterior and posterior ethmoidectomy was done. Lamina papyracea was separated from periorbita on both sides. Periorbita appeared normal. Bilateral maxillary and sphenoid sinus were cleared of the secretions. The septum was incised with adequate margins. After removing the specimen, dural repair was done with a temporalis fascia patch. Intradurally, a small pericranial-onlay patch was placed. An extradurally pedicled left temporalis facial flap was rotated and placed. Bone flap was repositioned. Postoperative histopathology studies showed esthesioneuroblastoma, Hyam grade 3. Adjuvant radiation therapy, 6,000 cGy in 30 fractions by intensity-modulated radiotherapy was given. Posttreatment, the patient has been kept on clinical and imaging surveillance, and is disease free at 12 months follow-up.
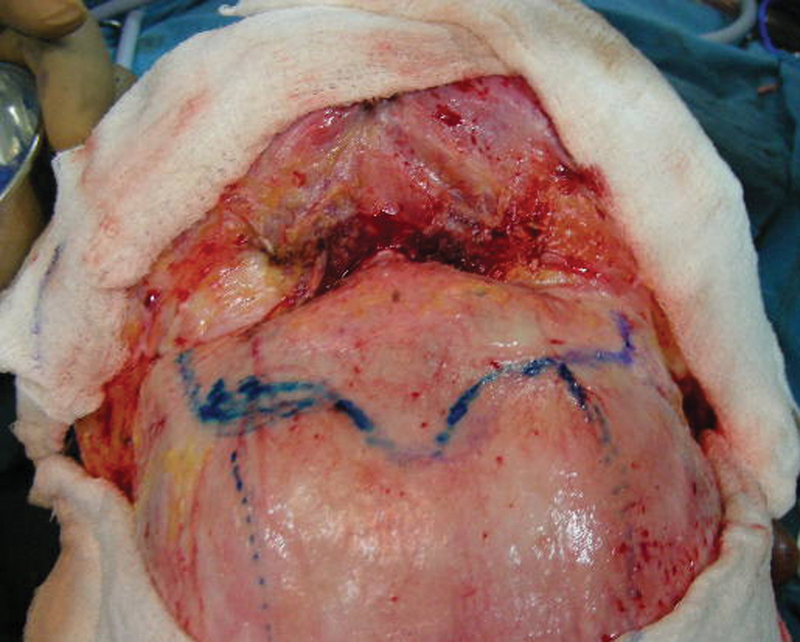
Intraoperative picture showing the extent of frontal sinus marked with transfrontal illumination method.
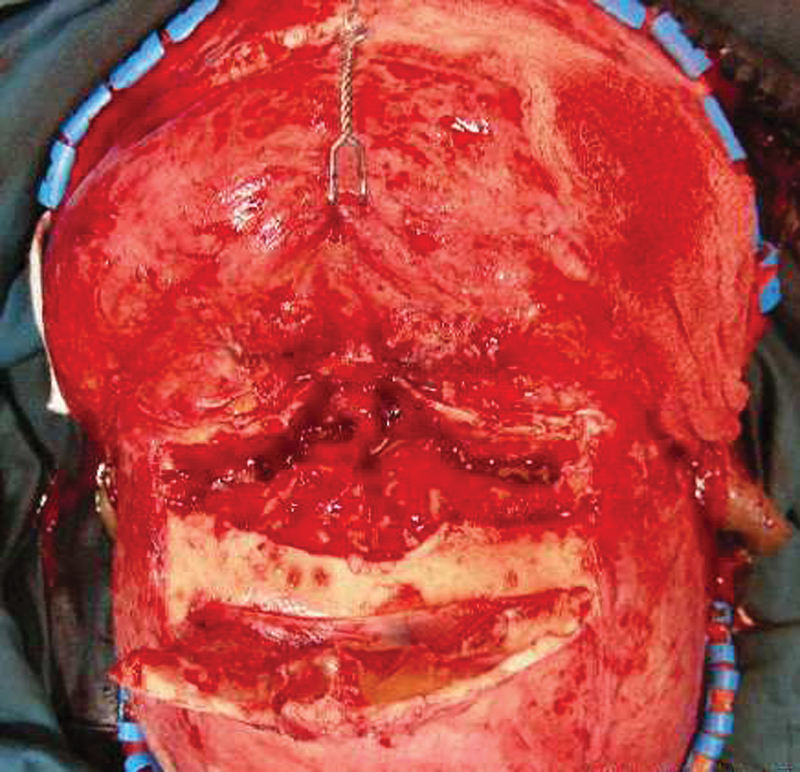
Intraoperative picture showing the subcranial approach with the tumor exposed.
Discussion
Joram Raveh developed the subcranial approach in 1978 as a technique for the treatment of trauma in the frontoethmoidal orbital region. It was later popularized for the removal of anterior skull base tumors. In this technique, the anterior skull base is approached by disarticulating the nasal root and glabella, to directly access the frontal and ethmoid sinuses and the anterior cranial fossa.1 Since then, this approach has been proposed as an alternative to transcranial bifrontal approach for selective indications. This approach provides a broad exposure to the frontal skull base with excellent access to anteromedial part of orbit, nasal, and paranasal structures.2 The approach enables the exposure of anterior skull base planes from the anterior to the posterior direction, under direct vision, avoiding frontal lobe retraction. This is in contrast to the craniofacial approach that requires, apart from the craniotomy, additional transfacial approaches so as to assess the tumor. It is considered by many authors as a less invasive approach than craniofacial resection, but it renders a broad exposure and visualization of the tumor margins. However, the exposure may be limited when it comes to large malignant tumors extending posteriorly and superiorly.
The reported patient had a malignant ethmoid tumor with a large intracranial component with dural involvement. A complete endoscopic approach was not attempted in this patient due to the large intracranial dural component with suspicious lateral dural involvement above the orbital roof. A standard craniofacial resection would have been the usual approach of choice, for a tumor of this size. But this patient had extensive pneumatization of his frontal and sphenoid sinuses, a condition known as PSD. The enlarged frontal sinuses in this patient gave us adequate exposure from above, helping in the clearance of the tumor by subcranial approach.
PSD is a rare entity described for the first time by Benjamins.3 It is characterized by idiopathic progressive expansion of one or more of the paranasal sinuses beyond normal margins without an associated mass. This rare disorder may affect all paranasal sinuses but frontal sinus involvement is the most common.4 Urken and coworkers5 classified abnormally pneumatized sinuses into hypersinus, PSD, and pneumocele. A hypersinus is a frontal sinus that has developed beyond the upper limits of a normal frontal sinus, but not beyond the normal boundaries of the frontal bone. The sinus is aerated and its walls are normal. PSD is an aerated sinus that is abnormally expanded. The sinus walls, although intact and of normal thickness, have been displaced outwardly to cause frontal bossing, intracranial extension or ethmoid, nasal or orbital encroachment. Pneumocele is an aerated sinus with either focal or generalized thinning of the bony sinus walls. However, many authors prefer to use the term “pneumosinus dilatans” for all cases of dilated, air-filled sinuses of uncertain origin with outwardly bulging walls, stating that differentiation of PSD from pneumocele radiographically is impossible, and both present with identical clinical symptoms.6 The pneumatization of the frontal sinus should be evaluated, irrespective of the definition, while planning an approach for frontal skull base tumor resection. The hyperpneumatized frontal sinus in the patient could be used effectively to perform a subcranial approach and resect the tumor with margins. This case demonstrates the importance of assessment of sinus pneumatization while deciding the approach for anterior skull base malignancies. We suggest that tracking the frontal sinus three dimensionally and creating a tangential projection from the superior limit of the sinus to the posterior end of the tumor would enable the surgeon to decide with confidence between the standard craniofacial resection and subcranial approach.
Conclusion
We report a case of advanced ethmoid malignancy with a large intracranial component with dural involvement that was removed by subcranial approach, in a patient with PSD. This case demonstrates that assessment of pneumatization of the frontal sinus is as important as the size and extent of the tumor, while deciding an anterior skull base surgical approach. Even large malignant lesions may be approached subcranially if the frontal sinus is proportionately large. PSD, though rare, can be used to the benefit of the patient in selecting a less invasive approach.
Footnotes
None.