
Abstract
The aim of this article is to report the clinical case of a right subcondylar fracture in a 4-year-old boy. The displaced and medial angulated fragmented mandibular condyle in coexistence with an enlarged lateral pterygoid process was compressing the inferior alveolar nerve (IAN) during its course in the area of the infratemporal fossa. This was expressed by exhibiting a rubbing behavior with resulting superficial ulceration at the right lower lip. Hypoesthesia of the lower lip may be a sign of the IAN entrapment after a subcondylar fracture in a child. In contrast to the adults where an open reduction is necessary to relieve the symptoms of hypoesthesia, in pediatric population, a conservative approach seems sufficient.
Mandibular fractures are uncommon in children and their incidence increases with the increasing age.1 The mandibular condyle is the most commonly involved area with an incidence ranging between 72 and 80%.2 Boys are more commonly affected than girls. The different fracture pattern in pediatric population is age related and is influenced by the bone elasticity in mandible, the mixed dentition, and the prominent skeletal background.1 Even though, the mandibular nerve passes through the foramen ovale in close proximity to the condyle, condylar fractures are rarely associated with nerve disturbances,3 although sporadic cases have been documented.45
The clinical manifestations of the condylar fractures include malocclusion, deviation to the affected side during maximum opening of the mouth and a slightly limited lateral excursion to the unaffected side, temporomandibular joint pain on palpation, some degree of trismus, chin abrasion or laceration, rupture of the external acoustic meatus and bleeding and cerebrospinal leak, and otorrhea in association with skull base fracture.6
Most authors adhere to a nonsurgical treatment protocol of condylar fractures in children.78 A long-term follow-up yielded good clinical outcome, except in unilateral fractures where the risk of failure is increased.9 This case highlights that hypoesthesia of the lower lip may be a sign of the inferior alveolar nerve (IAN) entrapment after a condylar fracture in children. It has been reported only in adults but never in children.
Case
A 4-year-old boy injured his chin during a game. The mother noticed that something was wrong and visited the local hospital. A computed tomography (CT) scan revealed a low right subcondylar fracture with medial displacement and angulation of the condylar fragment (Fig. 1). Clinically, the mouth opening was restricted to 26 mm, without deviation of the opening path during excursion. Both temporomandibular joints were not painful on palpation. The next day, the mother noticed that her child was chewing at the site of fracture causing a white patch and superficial ulceration of the right lower lip (Fig. 2a, b). In addition, the young boy demonstrated a constant rubbing of the teeth in the right-sided lower lip. Subsequently, the parents visited a tertiary center for a second opinion, considering the prolonged rubbing behavior. A cone-beam CT scan revealed a severe proximity between the angulated condylar fragment and the enlarged lateral pterygoid plate of the sphenoid bone. An entrapped IAN between the referred structures was diagnosed (Fig. 3a, b). The rubbing behavior of the young patient was the result of the lower lip hypoesthesia mimicking the bite wounds after the IAN anesthesia in dental practice. Several attempts of neurosensory mechanoreceptive and nociceptive testing did not yield reproducible results. An additional magnetic resonance imaging (MRI) was performed to detect if the fatty sheath around the involved nerve was compressed (Fig. 4). The MRI images revealed no compression and a conservative treatment followed. The patient remained on a soft diet during 4 weeks. Gradually, the ulceration of the lower lip healed, and the mouth opening was recovered.
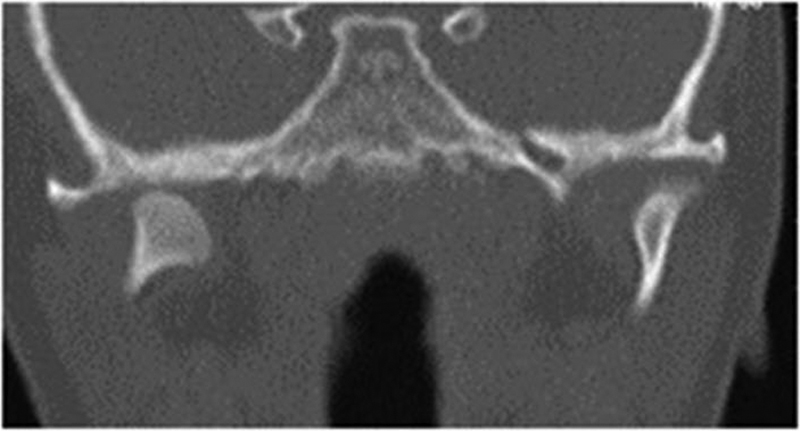
A frontal section of the right subcondylar fracture with displacement, medial angulation, and high position of the condylar head.
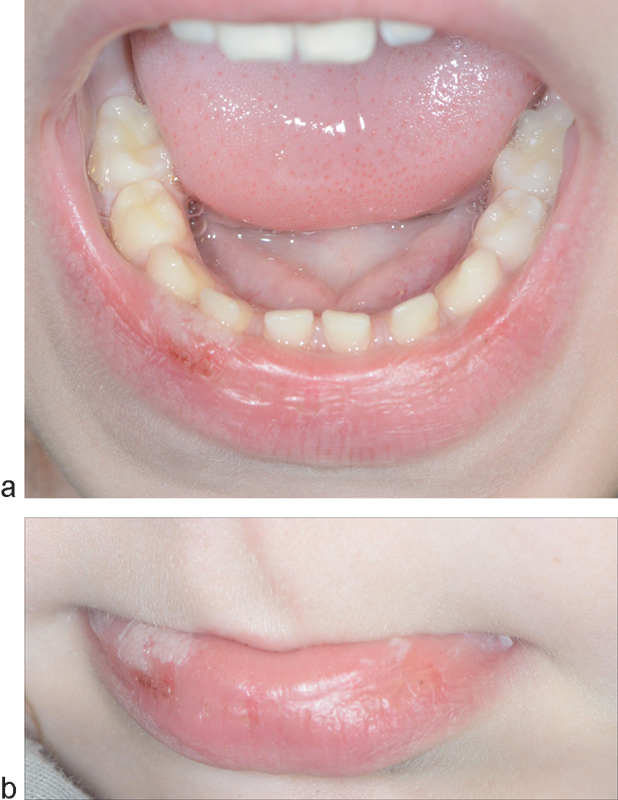
(a and b) Typical lesion corresponding to lip rubbing with the teeth: a whitish traumatic leukoplakia with localized ulceration at the anterior border is evident.
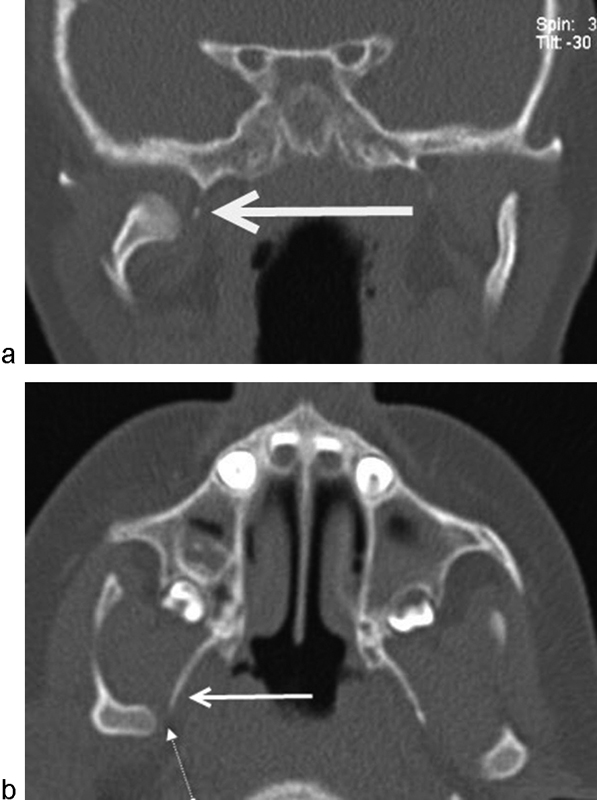
(a) The displaced but not dislocated fracture is depicted. The fragment is still connected to the ascending ramus of the mandible. The white arrow indicates the enlarged lateral pterygoid plate of the sphenoid bone. (b) Axial section clearly depicts the enlarged lateral pterygoid plate with the narrow passage for the inferior alveolar nerve between the condylar head and the pterygoid plate.
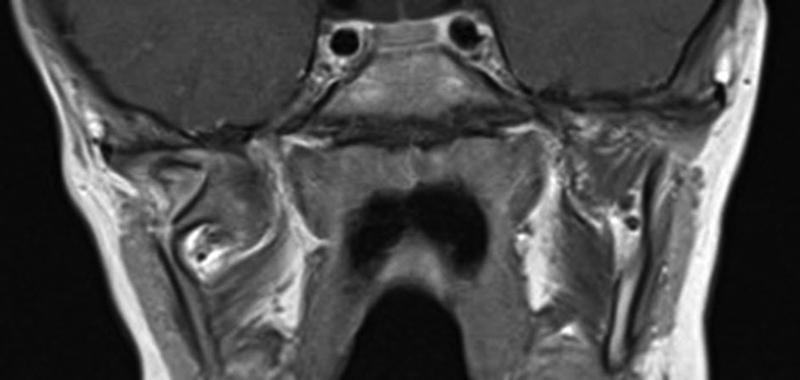
Frontal section of the magnetic resonance imaging shows no pathological alteration of the fatty tissue surrounding the inferior alveolar nerve.
Discussion
Young children are not capable to express the sensation of numbness of the lower lip. Therefore, the lip bite is a common complication after the IAN blockade. Because children are not familiar with this bizarre sensation, they usually rub, bite, or chew their inadvertently, since no pain is felt.10 In adults, the IAN or the lingual nerve anesthesia is a rare complication of condylar fractures because several preconditions need to occur simultaneously (Fig. 5).3 The first precondition is the type of fracture. A low subcondylar displaced and not dislocated fracture must exist. In dislocation, the condylar fragment is disconnected from the mandibular ramus and is unable to exert any compression. On the contrary, in displacement, the condylar fragment remains connected with the mandibular ramus and appears a variable degree of medial angulation.
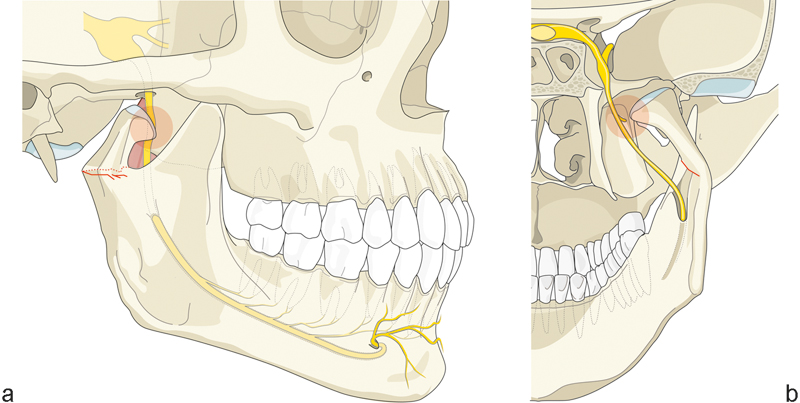
(a) In adults, the inferior alveolar nerve (IAN) or the lingual nerve anesthesia is a rare complication of condylar fractures because a number of preconditions need to occur simultaneously. (a and b) For the IAN to get compressed, a number of preconditions need to be met: a unilateral condylar fracture with displacement but no dislocation to exert compression (a) with an angulation toward an enlarged pterygoid process (b).
The second precondition is the degree of angulation of the fragment condyle. This broken part may be located beneath the skull base close to the foramen ovale.
The third precondition is that the presence of a unilateral fracture may allow the compression.
The fourth precondition which rarely occurs, but it was present in our case, is the enlargement of the lateral pterygoid process and the course of the IAN in the infratemporal fossa, between the condylar head and the enlarged lateral pterygoid plate.
In the literature review, Politis et al reported similar cases with anesthesia of the IAN and/or the lingual nerve.3 In these cases, symptoms were only relieved after open reduction of the fractures. In the young patient, a conservative treatment was chosen due to the fact that on MRI the compressed nerve did not show any sign of degeneration. Further follow-up proved that the lesions gradually healed and that the occlusion remained stable. Since objective neurosensory testing did not prove reliable, the resolution of the lip ulceration could equally well be due to the fact that the child became accustomed to the hypesthesia, or that the hypesthesia progressed to insensibility.
Conclusion
Unilateral displacement of a subcondylar fracture with medial angulation is capable of compressing the IAN toward an enlarged lateral pterygoid plate. In contrast to adults where an open reduction is necessary to relieve the symptoms of hypoesthesia, in a young child, a conservative approach may be feasible even in light of IAN involvement.