
Abstract
The main objective of this article is to evaluate the efficacy of platelet-rich fibrin (PRF) for secondary alveolar bone grafting. Patients between 9 and 14 years of age were included in study and were divided in two groups: Group 1—iliac bone with PRF and group 2—iliac bone without PRF. Radiographic assessment was done preoperatively, immediate postoperatively, and at 3, 6, and 9 months, respectively. Vertical bone height was assessed using 4-point scale. In group 1, 14 patients showed grade 1 resorption at 3 months and at 6 and 9 months all patients showed grade 1 resorption. In group 2, 16 patients had grade 1 resorption at 3 months, 2 patients had grade 2 resorption at 6 months, and 6 patients had grade 2 resorption at 9 months. Use of PRF growth factor with autogenous bone results in greater osteogenic effect which increases new bone regeneration and better wound healing.
Secondary alveolar bone grafting was first described by Boyne and Sand in 1972.1 Secondary alveolar bone grafting results in continuity of the maxillary arch thereby stabilizing the maxillary segments and also help in eruption of permanent teeth, obliterating oronasal fistula, and enhancing nasal base and facial appearance. Autogenous iliac bone graft is considered as the gold standard material because of sufficient quantity and high osteoinductive potential. However, even with iliac bone graft insufficient bone regeneration may occur due to several factors like patient's age, cleft width, bone resorption, and others.
Various materials like platelet-rich plasma and platelet-rich fibrin (PRF) have been developed and used to facilitate bone healing process, increase bone formation, and reduce bone resorption.2 PRF was first described by Choukroun et al and is a fibrin matrix in which cytokines, growth factor, and cells release substances and enhance tissue healing bone regeneration and formation.3 The aim of the study was to evaluate the efficacy of PRF on bone healing and quantity of bone formation at different time intervals for secondary alveolar bone grafting.
Materials and Methods
A prospective randomized study was carried on 40 patients with cleft alveolus between October 2014 and September 2016. The patients between the age range of 9 and 18 years were included in the study. Patients were categorized into two groups, a study group (iliac bone graft with PRF) and a control group (iliac bone graft without PRF) and were allocated randomly to each group by drawing lots at the time of surgery. The lot was drawn by a person who was not involved in the study and the information was passed on to the surgeon at the time of surgery. Cancellous bone graft was harvested from anterior iliac region and used for secondary alveolar bone grafting
Inclusion Criteria
Patients between 9 and 18 years of age with either unilateral or bilateral alveolar cleft.
Exclusion Criteria
Patients operated earlier for alveolar bone grafting.
Patients with systemic disease especially platelet disorders.
Patients with poor oral hygiene.
Preoperative Assessment
A through preoperative clinical and radiological assessment of patients was performed to determine the size of alveolar defects. The radiographs used to assess the defect include orthopantomogram, upper occlusal view, and cone beam computed tomography (CT) (KODAK 9000C and KODAK 9000C 3D extra oral Imaging System; Carestream Inc., 2016) All the patients were subjected to preoperative radiographs and immediate postoperative at 3, 6, and 9 months, respectively.
Platelet-rich fibrin Preparation
After the patient was anesthetized, 20 mL of fresh venous blood was drawn into two 10 mL vacutainer tubes (BD vacutainer tube, Becton Dickenson Inc.). Immediately after collecting the blood, tubes were shaken well to prevent clotting and placed in centrifuge machine with radius of 8 cm, at an angle of 25 degrees. The tubes were centrifuged at 2900 rpm for a period of 10 minutes with RCF(g-force) of 793.4 g4 (Sigma 3-3-ks; fixed angle rotor, Rotor diameter: 16 cm; Sigma laborzentrifugen GmbH). After centrifugation process, the tubes showed three distinct layers: platelet poor plasma in upper most layer, PRF in middle zone, and red blood cells in the lowest zone.
Operative Procedure
Alveolar bone grafting was performed under general anesthesia using standard Abhyloms Surgical Method for secondary alveolar bone grafting.1 The autogenous bone graft chips and PRF clot were mixed with bone particles so as to obtain proper consistency (Fig. 1) and were placed in the alveolar defect (Fig. 2) and closed with mucoperiosteal flaps.

Platelet-rich fibrin with bone graft.

Bone graft with platelet-rich fibrin in cleft alveolar region.
Postoperative Follow-Up
The patients were clinically assessed for wound healing, pus discharge, and dehiscence. Radiologically, the extent of postoperative vertical bone height was determined in relation to interdental bone height and assessed on a 4-point scale5 at immediate postoperative 3 months, 6 months, and 9 months, respectively. Patients in both groups were administered similar antibiotics, analgesics, and steroids as per their body weight.
The numerical data are collected and presented as mean with standard deviation. The significance of data was analyzed statistically using Student's paired t-test.
The necessary approval and clearance for the study were obtained from the institutional review board (ethical committee board)—IRB No. 2018/S/OS/56.
Results
A total of 40 patients were included in the study out of which 20 patients were in study group and 20 patients were in control group. Patients were selected randomly and categorized among the two groups. Mean age of patients in control group was 15.47 years and mean age of patients in study group was 15.11 years (Table 1). Among the 20 patients in study group, there were 10 male patients and 10 female patients and in control group there were 11 male patients and 9 female patients. Among the type of clefts in study group, there were 16 unilateral and 4 bilateral cleft cases whereas in control group there were 15 unilateral and 5 bilateral cleft cases (Table 2).
Comparisons between study and control group in relation to mean age by student's t-test

Abbreviations: SD, standard deviation; SE, standard error.
Comparison of patients between study and control group in relation to gender, site, and status unilateral/bilateral by chi-square test
Defect
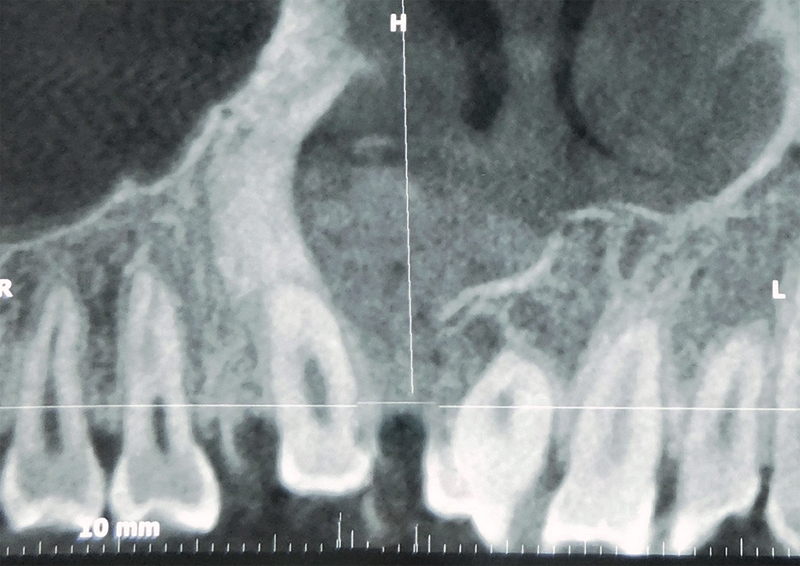
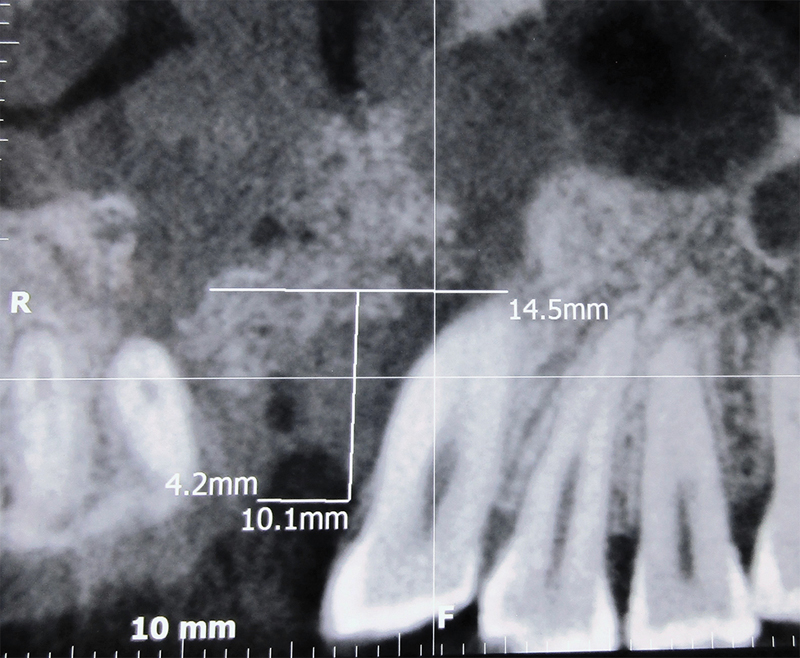
Preoperatively, the mean vertical height of the cleft alveolar defect in study group on cone beam CT was found to be 14.04 mm, whereas it was 13.9 mm in the control group. The maximum vertical height in study group was found to be 15.4 mm, whereas in the control group, it was 15.9 mm (Figs. 3, 4) (Table 3). Also, it was noted that maximum size of cleft defect at cementoenamel junction was 6.5 mm and maximum size at root apex was 11 mm in study group, while in control group maximum size of defect at cementoenamel junction was 5.8mm and defect size at root apex was 19.3 mm (Table 4). A statistical analysis of the vertical of the defect between the control and study group showed a p value of 0.1963 which was not significant. Also on comparison of width of the defect between two groups, a p-value of 0.8792 was noted and was not statistically significant. This was assessed with the mean and standard deviation values and the significance was analyzed using student s paired t-test (Table 5).
Comparisons of mean defect height between study and control group by t-test

Abbreviations: SD, standard deviation; SE, standard error.
Comparisons of mean defect-width between study and control group by t-test

Abbreviations: SD, standard deviation; SE, standard error.
Statistical analysis of mean defect size between study and control group by t-test

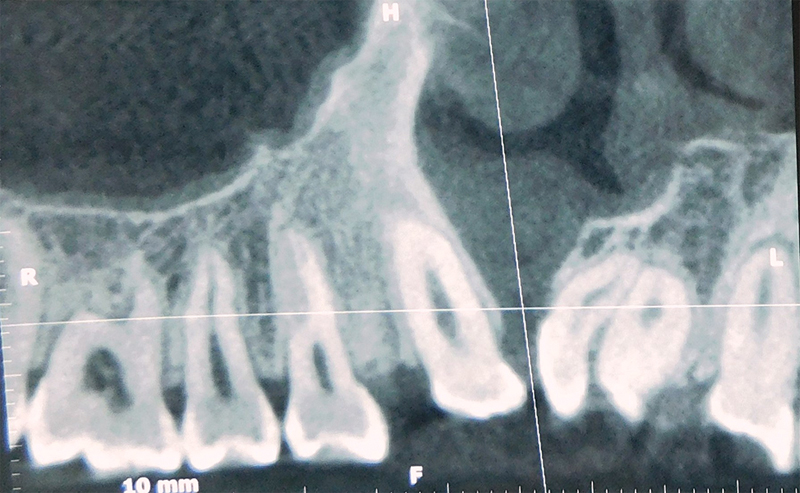
Study group preoperative radiograph.

Control group preoperative radiograph.
Wound Healing
Primary healing was observed in 16 patients (80%) and 4 patients (20%) showed secondary healing in the study group, whereas in control group primary healing was noted in 12 patients (60%) and in 8 patients (40%) healing was secondary in nature. Dehiscence was noted in 4 patients (20%) in the study group (Fig. 5), whereas 8 patients (40%) had dehiscence in the control group (Fig. 6), which is 50% more than the study group. Serous discharge was present in one patient (5%) in the study group, whereas six patients (30%) in the control group had serous discharge and none of them had pus discharge. Frequent irrigation and local dressing were used to promote secondary healing which was noted within 30 to 40 days of follow-up.

Study group immediate postoperative radiograph.

Control group immediate postoperative radiograph.
Bone Resorption
At 3 months follow-up in study group, 14 patients had grade 1 resorption and 6 patients did not show any resorption, while in control group, 16 patients presented with grade 1 resorption, 1 patient showed grade 2 resorption, and 3 patients did not show any resorption. On statistical analysis, no significant difference was noted at postoperative 3 months. After 6 months, all the 19 patients in study group showed grade 1 resorption with 1 patient showing grade 2 resorption and 14 patients in control group had grade 1 resorption pattern with 6 patients showing grade 2 resorption. No statistically significant difference was seen at postoperative 6 months. At 9 months follow-up in study group, 19 patients showed grade 1 resorption, 1 patient showed grade 2 resorption, and none of the patients in study group showed grade 3 and 4 resorption (Fig. 7), whereas in control group 8 patients showed grade 2 resorption and rest still showed grade 1 resorption (Fig. 8). On statistical comparison between the two groups on 9 months follow-up, we found p value of 0.007 which was significant (Table 6 and 7). Among the patients who had grade 2 resorption in control group, five patients were unilateral cleft alveolus and one patient was bilateral cleft alveolus. In study group, none of the unilateral or bilateral cleft patients presented with grade 2 resorption patterns. Among six patients in control group with grade 2 resorption pattern, three patients had wider cleft with defect width at cementoenamel junction of 5.8mm. While in study group, eight patients had cleft width more than 5.8 mm at cementoenamel junction, none of them had grade 2 resorption patterns.
Results of statistical analysis between the two groups at different intervals
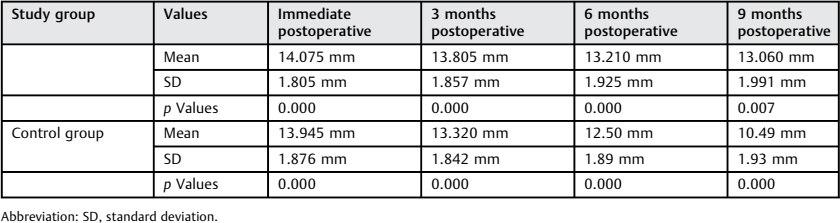
Abbreviation: SD, standard deviation.
Grade of resorption between two groups at different intervals

Study group postoperative 9 months radiograph.
Control group postoperative 9 months radiograph.
Discussion
The reconstruction of the alveolar process in patients with cleft lip and palate is well established. Development of biosurgical additives is one of the great challenges of clinical research which has been used to regulate inflammation and increase the speed of healing. Various biomaterials have been used for the treatment of cleft alveolar defects and have demonstrated variable results. The current study attempted to determine whether PRF is useful for preventing postoperative resorption of grafted bone in the alveolar cleft.
The way of checking the bone increase and decrease remains controversial. Various evaluation methods of postoperative course of grafted bone have been reported in dental radiographs occlusal radiographs, panoramic radiographs, and CT. In current study, we have used the digital volume tomogram radiographs for the measurement of alveolar bone. Trindade et al in their study found 86% of the cases with surgical success rate and also 95% success rate with canine eruption on 4 years follow-up and defends periapical radiograph to confirm the success of grafted bone.6 However, Feichtinger et al rejected two-dimensional radiographs to quantify bone loss and advocates three-dimensional (3D) CT for buccopalatal bone assessment.7 Oyama et al used 3D CT to compare iliac bone grafting with platelet-rich plasma and without platelet-rich plasma and found more bone in platelet-rich plasma group.8 They also stated that there is no widely accepted method for bone quantification and suggested that bone formation quality should be tested. Also, the cost factor influences the investigation used and makes the investigator handicapped. The deep vein thrombosis radiograph used in the study can be less sensitive in assessment of the bone resorption when compared with the 3D CT and hence can be the limitation of this study.
Autogenous bone provides three elements necessary to generate and maintain bone: scaffold for osteoconduction, growth factors for osteoinduction, and progenitor cell for osteogenesis. This is in agreement with previous studies that showed that autogenous bone graft harvested from the anterior iliac crest was gold standard and associated with higher success rate.9 Other donor sites such as tibia or chin are only chosen on small size defects because of limited amount of available bone. So, only autogenous iliac bone graft was used in all of our patients.
Particulate bone grafts were used in the current study because they are more readily incorporated and remodeled to the adjacent alveolus. This has been attributed to rapid revascularization. Moreover, particulate cancellous iliac grafts provide better and favorable results.8 In cases of deficient tissues and tissues sutured under tension, the spicules of a particulate graft may get exposed and exfoliate leading to partial graft loss. So as to prevent this (dehiscence and graft loss), we used PRF membrane to achieve an adequate seal to overcome the complications and challenges created by oronasal seal.
In the present study, the preparation of PRF followed the PRF protocol of Dohan et al.4 The preparation of PRF was simple and took only 10 minutes; there were no complications from the blood draw and PRF preparation. We used plastic vacutainer coated with silica to avoid tube breakage, cuts, and contamination. PRF represents a new revolutionary step in the platelet gel therapeutic concept. Unlike other platelet concentrates, this technique does not require any jellifying agent, but not more than centrifugation of the natural blood without additives.3 There is also a new concept in preparation of PRF in which centrifugation should be done at medium speed which yields in better PRF material and growth factor.10 However, we have followed the conventional method of obtaining PRF.
Platelet-rich fibrin contains a high concentration of platelets and is an autologous source of growth factors (platelet-derived growth factor, tumor growth factor, and vascular endothelial growth factor) cytokines, and leukocytes that affect healing and maturation of the soft tissue and bone formation. A wide range of intra- and extra-articular events and various signaling proteins mediate and regulate the healing process of both hard and soft tissues, respectively. Also, platelet concentrate in PRF has bioactive surgical additive which promotes hemostasis, regulates inflammation, and increases the speed of healing process.3 Also, a study by Kubesch et al found that by reducing the relative centrifugal force and increasing the centrifugal time lead to advanced PRF production with significantly higher growth factor release at different intervals over 10 days period.10 Study group patients showed improved healing, which was attributed to the PRF effect. This is in accordance with the latest studies that involved the use of platelet-rich plasma, fibrin glue, or allograft, together with the autogenous bone, to improve wound healing, bone density and decrease the amount of bone resorption.11
Platelet-rich fibrin membranes protect the surgical site; promote soft tissue healing; and when its fragments mix with graft material, it functions as a “biological connector” between the different elements of graft and acts as a matrix which supports neoangiogenesis, capture of stem cells, and migration of osteoprogenitor cells to the center of graft.12 PRF is believed to be effective in the first phase of healing during the first few weeks after surgery when growth factors are actively released, reaching a peak at 14 days after surgery, and then decrease gradually; this is another reason why PRF reduces bone resorption and accelerates wound healing in soft tissues.13
Pain was managed by using similar analgesics (aceclofenac with paracetamol combination) in both the groups for a period of 5 days. Donor site pain was managed by using bupivacaine (0.25%) which was administered by an epidural catheter at the donor site. Postoperative swelling was managed by administration of intravenous dexamethasone (as per body weight) intraoperatively and on the first postoperative day. Postoperatively, a combination of amoxicillin-clavulanic acid intravenous antibiotics was administered for a period of 3 days, following which oral antibiotics were administered for 3 to 4 days. These parameters were not assessed subjectively for long term (3, 6, and 9 months) as was done to assess the bone formation.
In our study, only two patients with PRF had dehiscence during early follow-up period, whereas six patients in control group had dehiscence with serous discharge which was managed conservatively, thus indicating a better and faster healing in PRF group. So, the acceleration of wound healing by PRF results in reduction in bone resorption. Aroca et al, in 6 months of their randomized clinical trial, concluded that addition of a PRF membrane positioned under the modified coronally advanced flap provided an additional gain in gingival/mucosal thickness at 6 months compared with conventional therapy.3 Miron et al in his article has mentioned that addition of PRF helps in speeding up of soft tissue wound healing.14
The role of PRF is subject to much debate, so in the present study, PRF was used to assess the bone formation and bone resorption in alveolar cleft bone grafting. This was in accordance with the finding of Marukawa et al who used PRF to promote bone formation and reduce bone resorption in alveolar cleft reconstruction.15 In the present study, PRF was added to the autogenous cancellous bone graft in study group for alveolar cleft reconstruction and study group patients (PRF) showed more radiopacity indicating presence of dense bone at 3, 6, and 9 months follow-up compared with control group. Radiopacity of adjacent tooth to the cleft was used to assess the bone formation and density as it remains constant.
In the current study, failure of bone graft grade 2 occurred in six patients in control group, whereas none of them had grade 2 bone loss in PRF group at 9 months follow-up. Bone present at 3 months was maintained for the period of 9 months in PRF patients, whereas there was bone resorption grade 2 at 9 months follow-up in control group. This finding can be attributed to the additional biological properties of PRF which acts like adhesive, holds, and maintains the bone and flap in stable position. Studies by Simonpieri et al provide evidence that addition of PRF to bone during these interventions offers better postoperative control of the surgical site and seems to accelerate the integration and remodeling of the grafted biomaterial.12 Lucaesrely found no significant differences between both groups on bone regeneration based on the digital radiographs 1 to 6 months after surgery.4 Miron et al in his article have noted that PRF acts as an ideal material after bone grafting by improving bone healing/regeneration, preserving quality and density of the residual ridge.14
Apart from above-mentioned PRF factor, various prognostic factors for postoperative bone resorption in secondary autogenous bone grafting have been identified. Many authors have indicated that age at operation, width of the alveolar cleft, volume of grafted bone, and position of canine teeth are the major factors that affect bone resorption of the bone bridge. Several authors have emphasized that continuous mechanical stress by the adjacent teeth is the most important factor that influences bone resorption of grafted bone.
In our results, we found a marginal effect on bone resorption pertaining to bone width at cementoenamel junction. Three patients in control group with cleft width of 5.8mm at cementoenamel junction showed grade 2 bone resorption, but eight patients with cleft width of more than 5.8 mm in study group did not show any grade 2 or grade 3 resorption; this shows that patients with the wider cleft with PRF had lesser resorption in study group when compared with the patients with wider cleft without PRF in control group. On statistical comparison between the two groups at 3 months, 6 months, and 9 months intervals, we did not find any significant difference between the two groups. However, apart from the cleft width, other factor also plays important role in outcome of bone grafting such as soft tissue availability; tissue quality among other factors A study by Long et al showed significant but low negative correlation between cleft width and outcome of bone graft. Also, they stated that not absolute cleft width itself, but the cleft width as it relates to the availability of neighboring soft tissues for appropriate design and construction of flaps may be the critical factor.16
In our study, all the patients had undergone presurgical orthodontics wherein arch expansion was performed thereby increasing cleft alveolar width. The lack of significant difference relating to the cleft width to the success of alveolar bone grafting seems to indicate that presurgical expansion can be performed without the fear of bone resorption. In control group, there were 7 patients who underwent secondary bone grafting and 13 patients underwent late secondary bone grafting, whereas in study group 8 patients underwent early secondary bone grafting and 12 patients underwent late secondary bone grafting. In control group, we found remaining bone levels of 81.33% in late secondary bone grafting group, while in intermediate bone grafting group we found bone levels of 84.23%. In study group, we noted remaining bone levels of 92.39% in late alveolar bone grafting group, whereas in early bone grafting group we noted bone levels of 93.35%.
Conclusion
The PRF with autogenous bone graft may favor formation of new bone. PRF keeps the graft particles together and preserves the height of graft better than control group. It can be concluded that applying growth factor to bone defects results in greater osteogenic effects than applying nothing. Also, PRF is more than growth factors; it also includes cells and a fibrin matrix which has been shown to have an effect on vascularization.10 Hence, because of its ease of use combined with its low cost and autologous source, PRF is an ideal biomaterial for regeneration of bony defects.14
Footnotes
None.