
Abstract
Despite recent advances in the diagnosis and therapy of patients with chronic renal failure and secondary hyperparathyroidism (HPT), 5% of these patients may need parathyroidectomy. The purpose of this article is to present our experience with parathyroid surgery in 30 patients with chronic renal failure at “La Paz” University Hospital, analyzing the clinical and biochemical evolution after surgery as well as the recurrence rate. In the first month after surgery, calcium, parathyroid hormone, phosphorus, and alkaline phosphatase levels, as well as bone pain and pruritus, all decreased significantly. Within the first postoperative year, 24 patients remained asymptomatic, and no recurrent secondary HPT was detected. Within the second year after surgery, 15 patients were asymptomatic, and 3 patients showed a recurrence. According to these results, parathyroidectomy is an appropriate surgical procedure for patients with severe overt secondary HPT.
The appropriate use of phosphate binders, calcium supplements, and especially vitamin D analogs has significantly decreased the incidence of overt secondary hyperparathyroidism (HPT) in patients undergoing dialysis. With the demonstration that calcitriol can directly inhibit parathyroid hormone (PTH) secretion together with the availability of intravenous calcitriol, the possibility of inhibiting PTH secretion and avoiding parathyroidectomy may become a reality. 1 Nevertheless, approximately 5% of these patients may still need parathyroidectomy, 2 especially in the event of severe clinical signs and symptoms. In 1960 Stanbury et al 3 for the first time described subtotal parathyroidectomy in patients with chronic renal failure. During the last 3 decades subtotal parathyroidectomy or total parathyroidectomy with autotransplantation of parathyroid gland tissue has become the preferred surgical approach. Nevertheless, recent data from Kaye et al 4 have caused researchers to question such a procedure and have cast a favorable light on the use of total parathyroidectomy.
Parathyroidectomy is indicated in patients with chronic renal failure and secondary HPT who have severe pruritus, extensive soft tissue calcification, calciphylaxis, bone pain, muscular weakness, spontaneous fractures, significant mental disturbance, and biochemical disorders, such as a serum calcium level greater than 11 mg/dL and a calcium phosphate product greater than 70 mg/dL.
The surgical options include total parathyroidectomy with or without autotransplantation of parathyroid tissue and subtotal parathyroidectomy.
METHODS AND PATIENTS
Between November 1992 and March 1997, 30 patients with chronic renal failure and secondary HPT underwent parathyroidectomy at the Department of Otorhinolaryngology, “La Paz” Hospital. Autotransplantation of parathyroid tissue was performed in 25 of the patients of this series. The clinical and biochemical evolution after surgery and the recurrence rate were analyzed retrospectively.
The patients ranged in age from 28 to 70 years (mean 53.5 ±11.6 years, median 53 years). Sixteen patients were women and 14 were men. All were receiving chronic maintenance dialysis.
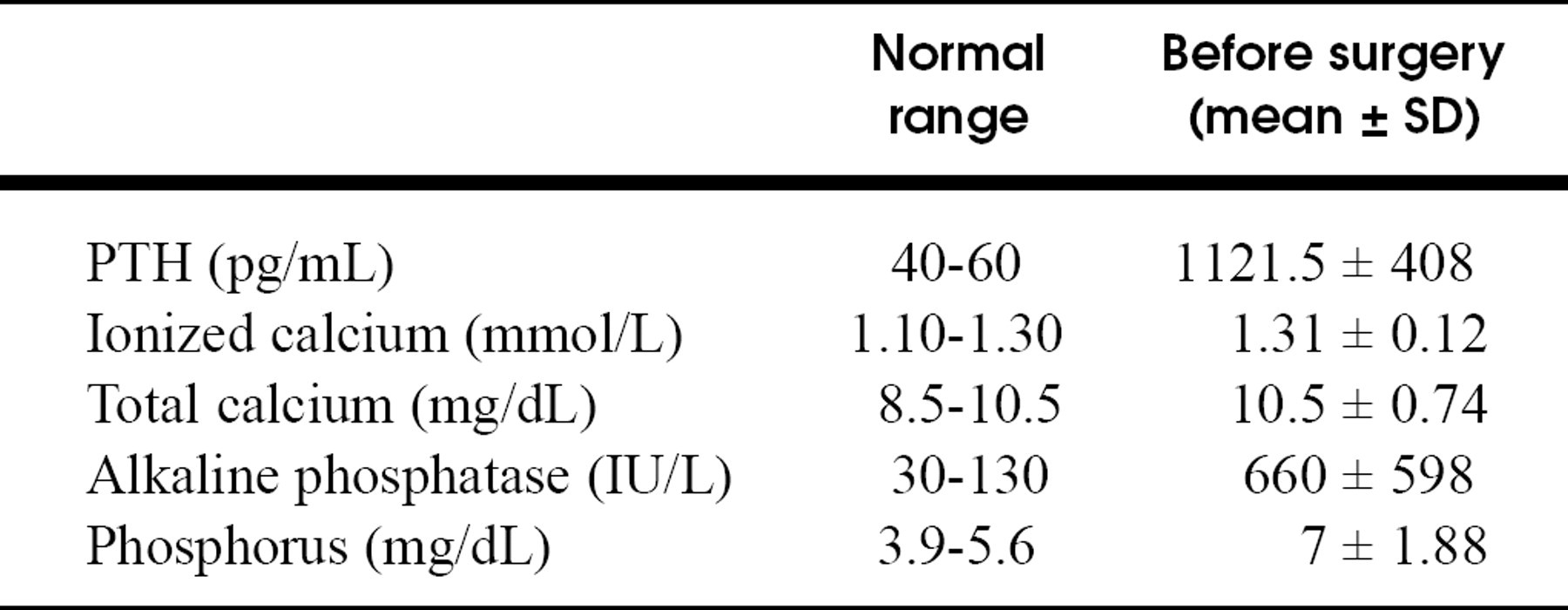
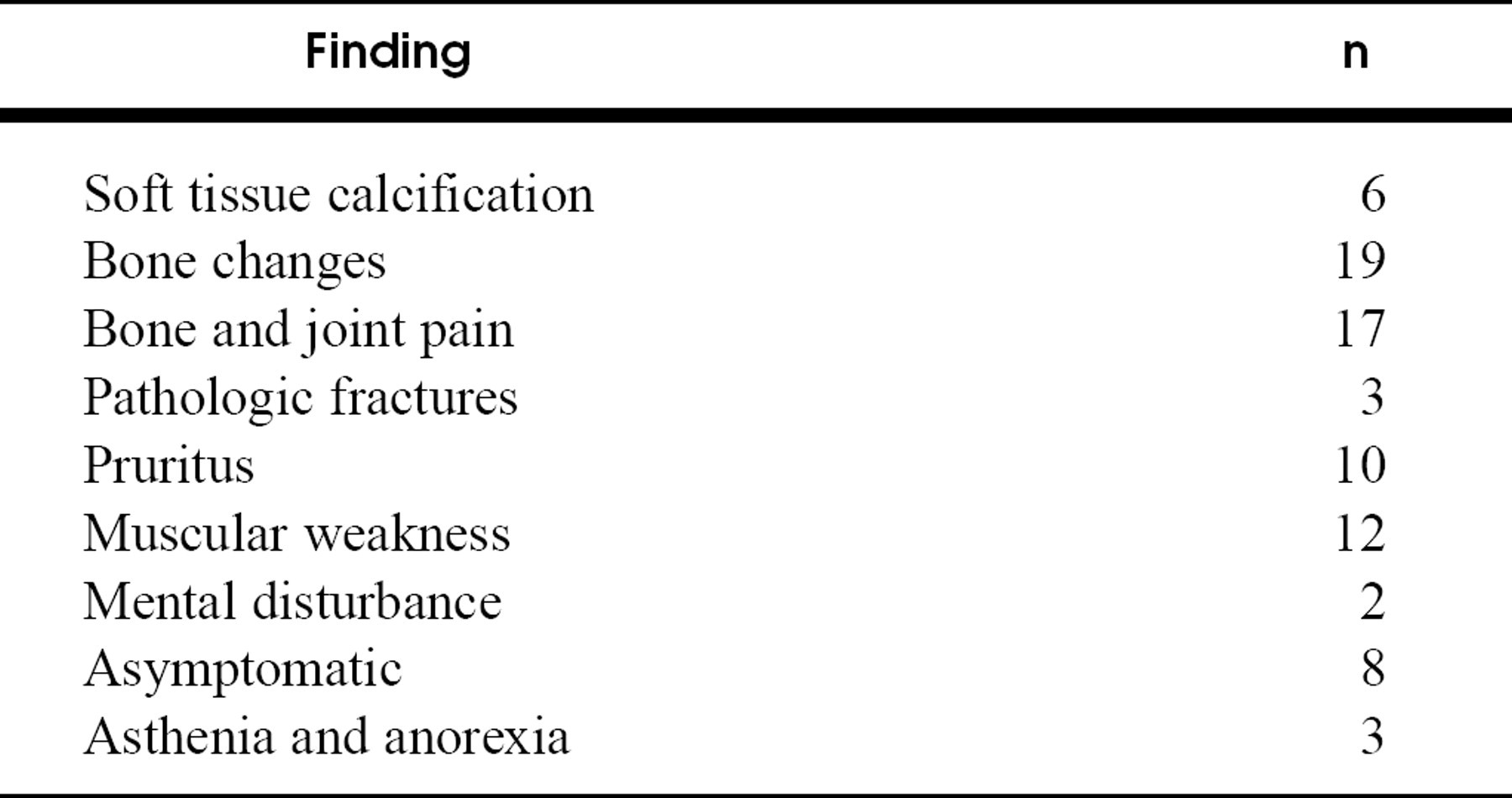
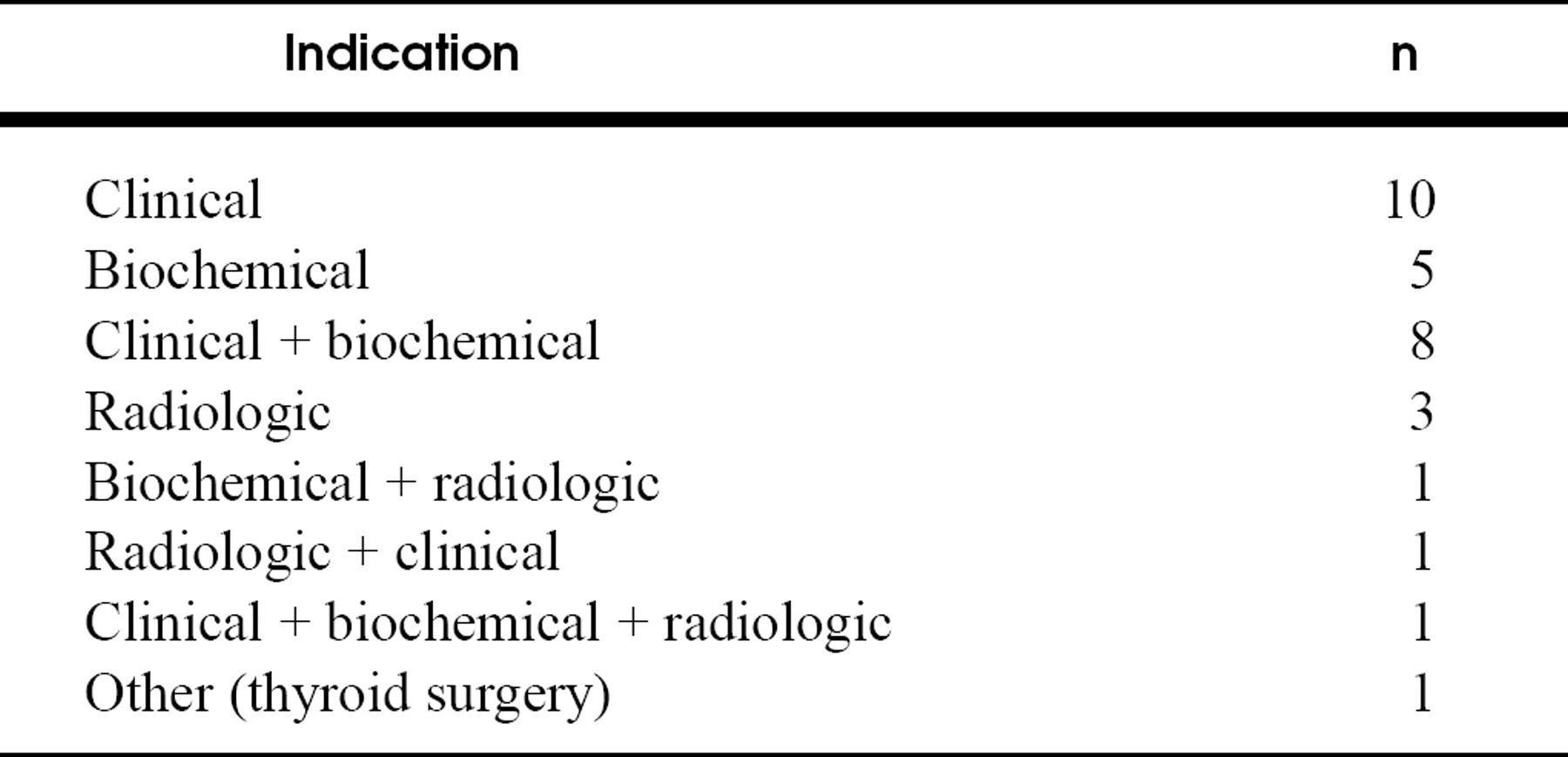
Most of the patients had signs of severe secondary HPT, which included high levels of PTH (Tables 1 and 2), bone pain, severe pruritus, osseous erosions, and vascular and soft tissue calcifications (Table 3). Patient symptoms were the main indication for parathyroidectomy in 20 cases (Table 4).
Preoperative versus postoperative laboratory and clinical findings were compared 1 and 2 years after parathyroidectomy.
RESULTS
The surgical technique was total parathyroidectomy with autotransplantation to the sternocleidomastoid muscle in 14 patients and to the brachioradialis muscle in 11. Autotransplantation was performed by implanting ten 1 × 3 mm parathyroid slivers into the recipient muscle in an area about 5 × 5 cm. Five patients underwent total parathyroidectomy without autotransplantation. During surgery, it is imperative that all parathyroid glands be identified: 4 glands were identified in 25 patients, 3 glands were visualized in 4 patients, and interestingly, 5 glands were localized in 1 patient. All excised glands were verified histologically.
Preoperative laboratory findings
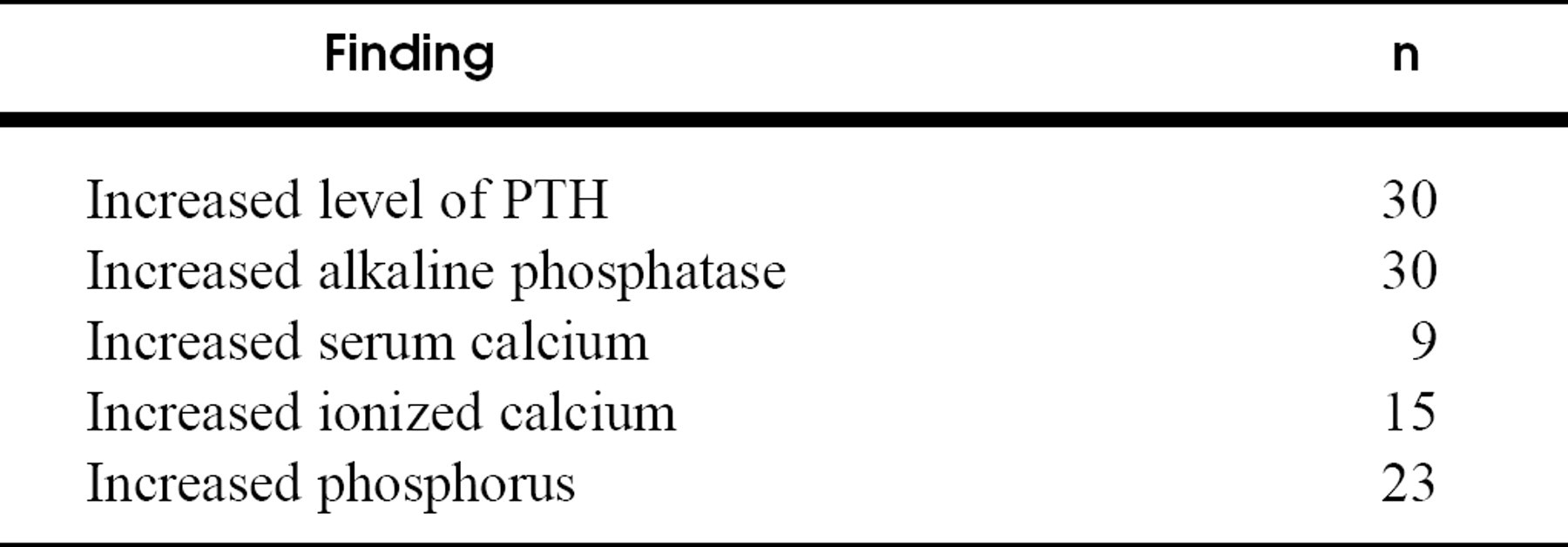
Biochemical measurements (n = 30)
Preoperative clinical and radiologic findings
A transient recurrent nerve palsy developed in 1 patient. No septic complications were noticed in the neck or the forearm wound. Oral or intravenous calcium administration was always needed to correct hypocalcemia during the first postoperative days to avoid tetany and convulsion.
Follow-up ranged between 12 and 60 months, with 18 patients being followed up for 2 years. In most patients there was a rapid decrease in serum ionized calcium and PTH levels during the first postoperative month, as well as a remarkable clinical improvement.
Indications for parathyroidectomy
Biochemical measurements after parathyroidectomy
Clinical findings after parathyroidectomy
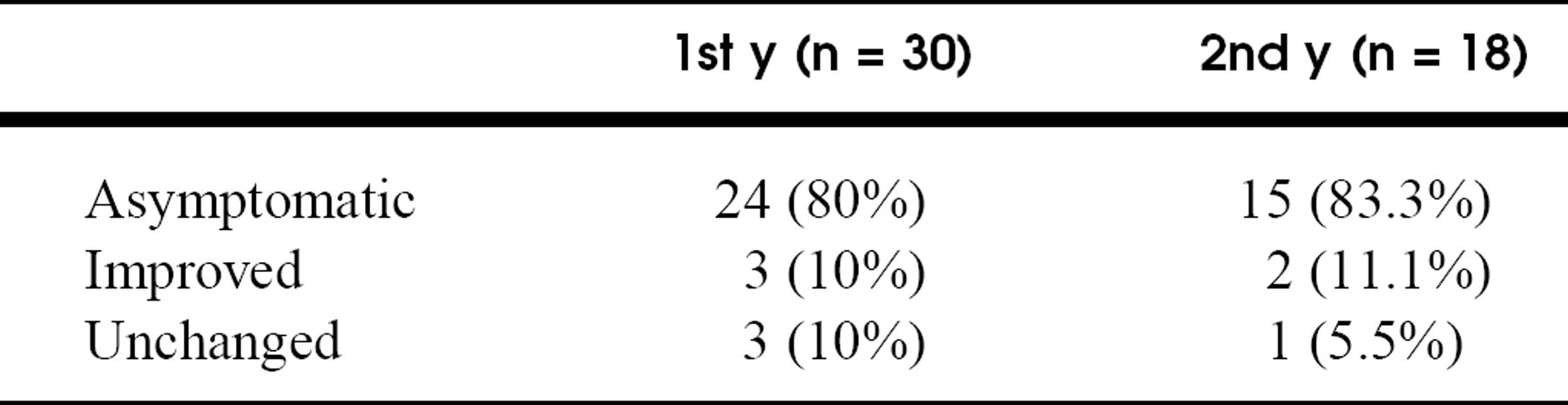
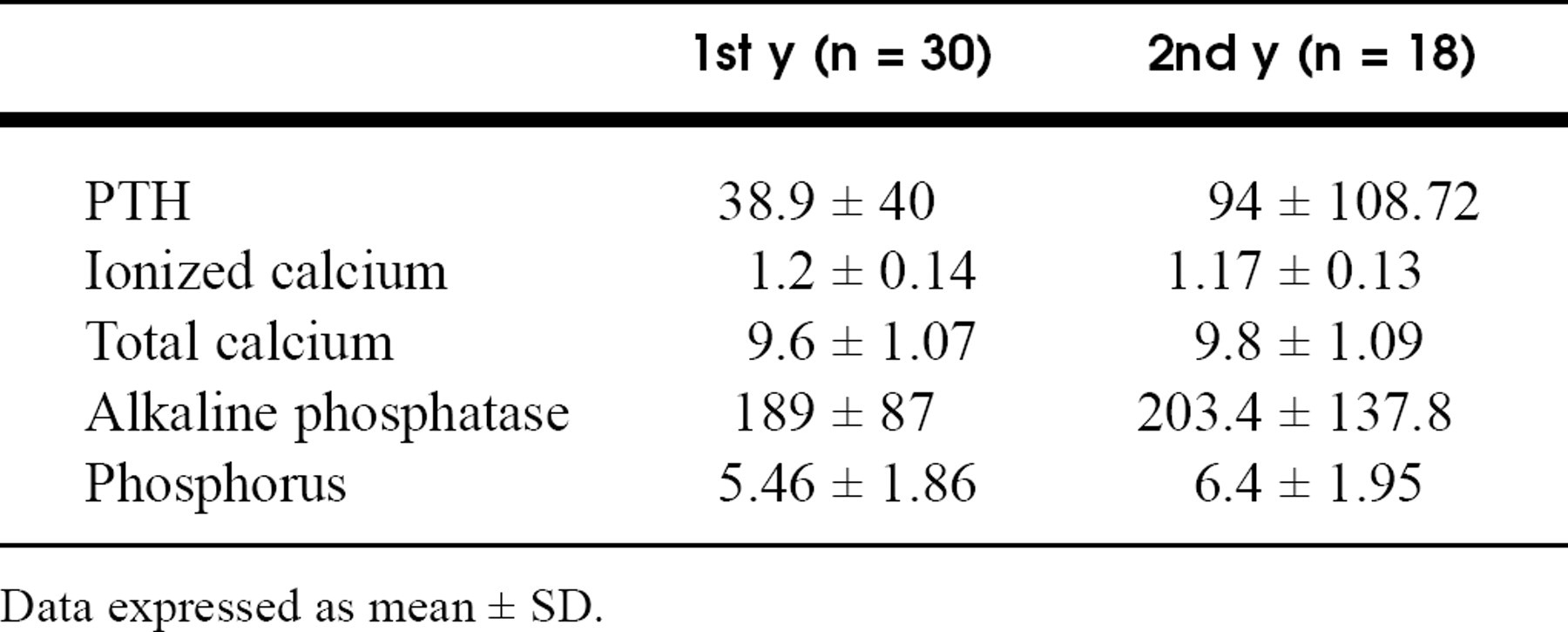
Within the first postoperative year, all of the biochemical measurements became normal except for the plasma alkaline phosphatase level, and 24 patients remained asymptomatic. Symptoms improved in 3 patients, and the clinical findings remained unchanged in 3 cases. The mean biochemical measurements 1 and 2 years after parathyroidectomy are detailed in Table 5.
Within the second year after surgery, 15 patients were asymptomatic (Table 6). The mean biochemical values have slightly increased in 18 of 30 patients, except for the level of serum ionized calcium, which has continued to decrease.
No recurrent secondary HPT was detected during the first postoperative year. In the second year, 3 patients had a reappearance of the symptoms, abnormal laboratory parameters, and radiologic signs. These patients had undergone total parathyroidectomy with autotransplantation to the sternocleidomastoid muscle and required a second operation. One of them underwent a third operation with mediastinal exploration. Histology of all tissue removed from the graft site revealed hyperplasia.
DISCUSSION
The main disadvantage of subtotal parathyroidectomy is the persistence or recurrence HPT because of inadequate parathyroidectomy. Persistent secondary HPT can be defined as the persistence of the typical symptoms, laboratory parameters, and radiologic signs within 6 months. A later occurrence of symptoms and signs of secondary HPT should be classified as recurrence.
During the last 2 decades, total parathyroidectomy with or without autotransplantation of parathyroid gland tissue has become the standard surgical approach. Autotransplantation is made to the sternocleidomastoid muscle or to the forearm, and this technique avoids the risks of hypoparathyroidism. 5 The benefit of total parathyroidectomy and autotransplantation to the forearm is the resection of parathyroid tissue with only local anesthesia, 6 in cases of recurrence.
Total parathyroidectomy without autotransplantation avoids recurrent HPT, but the remineralization of bone is not possible in the absence of PTH. In addition, the patient must undergo lifelong supplemental treatment with vitamin D analogs and oral calcium, which is an expensive treatment.
Although each procedure has its advocates, the most important factor in the outcome of surgery is to have a highly skilled surgeon experienced in parathyroid surgery. Knowledge of the embryologic development and the normal anatomy of parathyroid glands remains the most important point in the strategy of parathyroid surgery. Intraoperative identification of the recurrent laryngeal nerve is mandatory in surgery of the parathyroid glands and thyroid gland.
CONCLUSION
The results of this series confirm that total resection of hyperplastic parathyroid glands with autotransplantation remains a successful surgical procedure for patients with chronic renal failure and secondary HPT.
We thank Thomas J. McDonald, MD, for his editorial assistance with the preparation of this manuscript.