
Abstract

Patient selection is most crucial to minimize complications. Recent series have reported the incidence of these complications to be between 5% and 18%. 1 Despite improvement in the technique and surgical armamentarium of most nasal surgeons, rhinoplasty remains a procedure with known propensity for serious and life-threatening complications. An unusual complication is a false aneurysm of a branch of the facial artery that has developed at the site the lateral osteotomy after rhinoplasty.
CASE REPORT
A 20-year-old woman had an external nasal deformity and no symptoms of nasal obstruction. She was taking no medications, had no history of excessive or prolonged bruising, and had a negative family history for bleeding tendencies. Preoperative evaluation included a complete blood cell count and urine analysis, both of which were normal. The endonasal transcartilaginous approach was used. After removal of the bony hump, the periosteum of the lateral nasal wall was elevated through a stab mucosal incision at the level of the pyriform aperture. Medial and lateral osteotomies were then completed. No excessive bleeding was noticed during the course of the operation. The anterior nasal cavity was packed with a petroleum jelly pack. The patient received antibiotic prophylaxis and 30 mg of dexamethasone divided in 3 doses during the first 24 hours after surgery. Fourteen days after surgery a 1 × 1 cm bulge was noted on the left lateral nasal wall, just superior to the alar crease (Fig 1). The mass was soft, nontender, and compressible, and it had a bluish discoloration. No bruit could be heard. Using a 10-mL syringe, fresh blood was retrieved from the mass. External carotid angiography with a selective left facial arteriogram showed a 0.7-cm false aneurysm of the lateral nasal branch of the facial artery (Fig 2). Consequently, the aneurysm was embolized with Gelfoam. Follow-up of the patient for 8 weeks showed progressive regression of the mass. At 3 months after embolization no mass could be seen or palpated.

Bulge on the left lateral nasal wall (arrow).
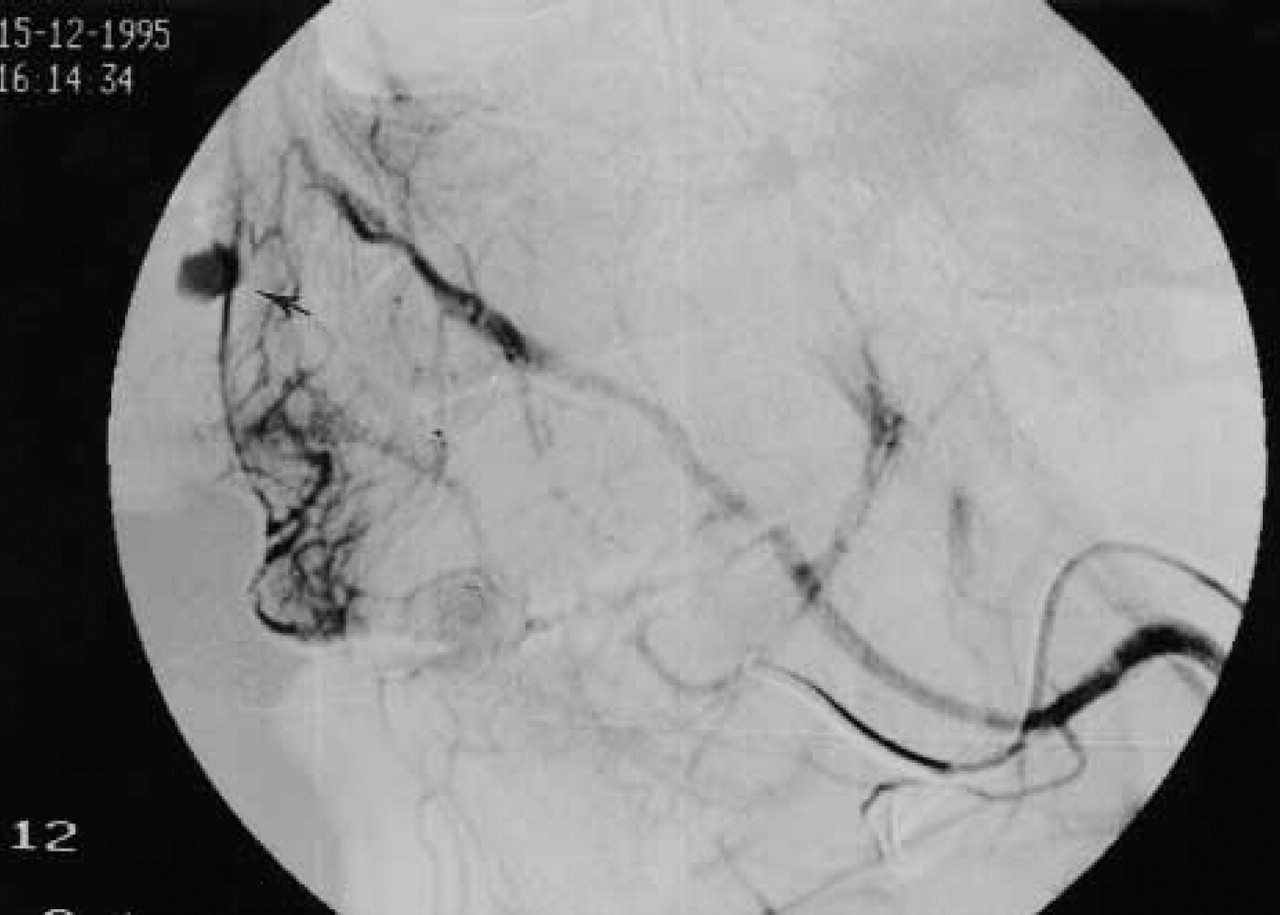
Selective left arteriogram showing a 0.7-cm false aneurysm (arrow).
DISCUSSION
There is an increasing body of literature on several maneuvers developed to improve patient satisfaction after rhinoplas-ty. 2 However, many complications may still be encountered. These include hemorrhage, hematoma, infection, periostitis, edema, ecchymosis, and skin bruises. 3 One rare but interesting late complication is the development of a false aneurysm of one of the branches of the facial artery. A similar complication after a motor vehicle accident was reported by Partridge and Saliva. 4 The diagnosis was made by Doppler ultrasonography, and the aneurysm was repaired surgically. There is no report, however, of a false aneurysm of the external lateral nasal wall after rhinoplasty.
The blood supply to the external nose is derived from the internal maxillary artery, the facial artery, and the ophthalmic artery. The facial artery, also known as the external maxillary artery, probably provides the major blood supply through its several branches. It crosses the border of the mandible anteriorly and turns superiorly and medially to give branches to the upper and lower lips before terminating as the angular artery near the medial canthus. The superior labial artery branch goes to the lower border of the alae and base of the nose as well as to the septum, where it joins the ophthalmic artery of the internal carotid artery. The angular artery also connects with the ophthalmic artery. The internal maxillary artery, also known as the infraorbital artery, sends small branches that communicate with the external maxillary arteries supplying the lateral wall and the dorsum of the nose. A small branch of the opthalmic artery, the supraorbital branch, contributes to the blood supply of the root of the nose. The course of a lateral osteotomy may intersect the course of the branches of the facial artery. It can be started high or low on the pyriform aperture edge and courses cephalad along the thicker bone of the ascending process of the maxilla. At the level of the infraorbital rim, the lateral osteotomy curves anteriorly just above the medial canthal plane. Potential sites of vascular injury during lateral osteotomies can occur at the level of the nasal artery along the cephalic course of the osteotomy, or at the level of the angular artery anterior to the medial canthus.
An aneurysm is by definition an abnormal dilatation of an artery or vein. A false aneurysm, or pseudoaneurysm, develops at the site of the arterial injury, be it sharp or blunt. The artery is not completely transected, and consequently the arterial flow is maintained beyond the site of the injury, and no thrombosis or retraction occurs. In these cases the systemic arterial pressure will cause a pulsating hematoma that may expand with time because the wall of the false aneurysm is deficient in elastic fibers. Symptoms of compression of adjacent structures may occur. Preoperative embolization and surgical excision are the treatments of choice in high-flow malformations. Sclerotherapy is effective in low-flow lesions. 5 Transarterial vessel occlusion has become a valuable primary and adjunctive treatment for symptomatic congenital and acquired head and neck vascular anomalies. Although optimal placement of the occlusive material into the nidus of the lesion is required for permanent embolic obliteration to be successful, complex proximal vasculature may prevent adequate catheter positioning. In our case, transarterial embolization was sufficient to induce thrombosis of the pseudoaneurysm with concomitant regression of its size.