
Abstract
PURPOSE: Our goal was to characterize the dynamics and bacterial interaction of the aerobic and anaerobic flora of nasal discharge of children at different stages of uncomplicated nasopharyngitis.
METHODS AND PATIENTS: Serial semiquantitative nasopharyngeal (NP) and quantitative nasal discharge (ND) cultures were taken every 3 to 5 days from 20 children in whom purulent discharge eventually developed (group 1), and a single culture was obtained from a group of 20 who had only clear discharge (group 2).
RESULTS: Aerobic and anaerobic bacteria were isolated from all NP cultures. Bacterial growth was present in 8 (40%) NDs of group 2. Only 7 (35%) of the clear NDs of group 1 showed bacterial growth; the number increased to 14 (70%) at the mucoid stage and 20 (100%) at the purulent stage. It declined to 6 (30%) at the final clear stage. The number of species and total number of organisms increased in the NDs of group 1. Group 1 patients had higher recovery rates of Streptococcus pneumoniae and Haemophilus influenzae in their NP cultures than group 2 patients (P < 0.05). During the purulent stage, Peptostreptococcus species were isolated in 15 (75%), Fusobacterium species in 10 (50%), Prevotella species in 9 (45%), H influenzae in 8 (40%), S pneumoniae in 6 (30%), and β-hemolytic streptococci in 5 (25%) of group 1 NDs. This was higher than their recovery in the clear stages of both groups and the mucoid stage of group 1. A total of 8 organisms capable of interfering with the growth of potential pathogens were isolated from the NPs of group 1, as compared with 35 from group 2 (P < 0.001).
CONCLUSIONS: The development of purulent nasopharyngitis is associated with the pre-existing presence of potential pathogens and the absence of interfering organisms.
Purulent nasopharyngitis is commonly found in children with upper respiratory tract infections. The nasal discharge in children is generally initially clear and watery; however, in cases that progress, it becomes viscous, opaque, and discolored (white, yellow, or green). Usually, without specific therapy, the purulent discharge resolves or becomes watery again before disappearing. 1 Most previous microbiologic studies 2 – 4 of the purulent nasal discharge used techniques for the recovery of only aerobic and facultative anaerobic bacteria. The role of strictly anaerobic bacteria, which have been recovered in many other upper respiratory tract infections, 5 was therefore relatively unexplored. Furthermore, all previous studies described the microbiology of the purulent stage of nasopharyngitis and did not explore the dynamics of the infection.
The nasopharynx of healthy children is generally colonized by relatively nonpathogenic aerobic and anaerobic organisms, 6 some of which possess the ability to interfere with the growth of potential pathogens. 7 – 9 The organisms with interference potential include aerobic α-hemolytic streptococci (mostly Streptococcus mitis and Streptococcus sanguis), anaerobic streptococci (Peptostreptococcus anaerobius) and Prevotella melaninogenica. 10
Conversely, carriage of potential respiratory pathogens such as Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis increases significantly in otitis media-prone children and in the general population of young children during respiratory illness. 11 The role of nasopharyngeal colonization by organisms with interference capability and development of purulent nasopharyngitis were not previously studied.
The purpose of this study was to characterize the aerobic and anaerobic bacterial flora of nasal discharge obtained from children at different stages of uncomplicated nasopharyngitis. A correlation was made between the bacterial flora and the eventual course of the illness. It also investigated the relationship between colonization of the nasopharynx with organisms with interfering capability and the subsequent development of purulent nasopharyngitis.
METHODS AND PATIENTS
Children seen consecutively in the pediatric clinic for acute nasal discharge were included in the study. Serial nasopharyngeal (NP) and nasal discharge (ND) cultures were taken from the children every 3 to 5 days if they were still symptomatic or if the quality of discharge had changed. Fourteen additional children who did not fulfill these criteria were not included in the study. Included in the final analysis were the first 20 children in whom purulent discharge had developed (group 1) and had at least 4 consecutive cultures, 1 at each stage of the illness: the clear secretion stage (days 1–4), mucoid discharge stage (days 4–7), purulent discharge stage (days 6–13), and clear stage (days 9–15). Patient whose symptoms did not clear within 15 days were not included. The children in the other group were the first 20 who had only a clear nasal discharge and did not enter a purulent stage (group 2). These patients had only a single nasopharyngeal and secretion culture.
Microbiology of 40 children with nasal discharge
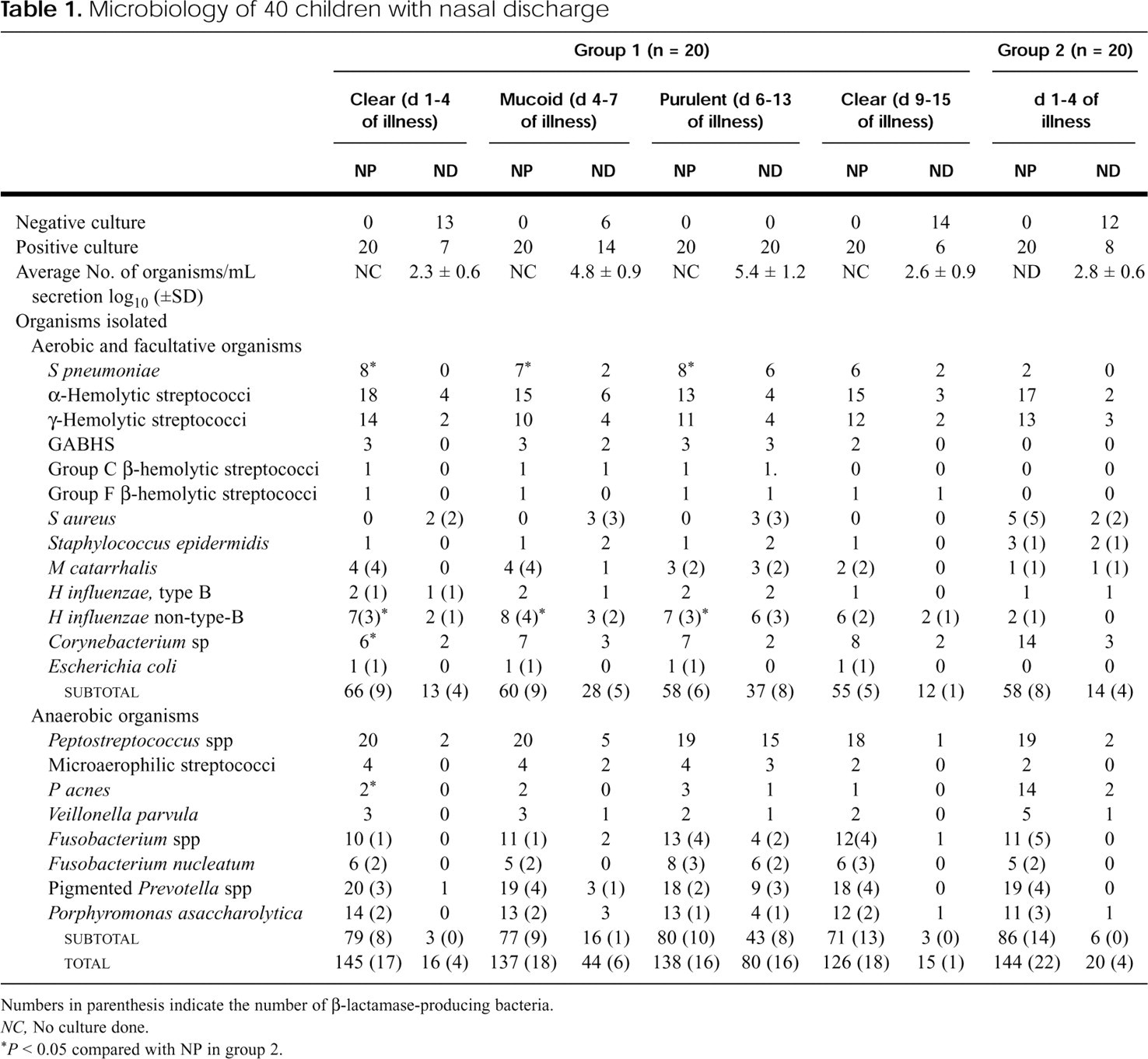
Numbers in parenthesis indicate the number of β-lactamase-producing bacteria.
NC, No culture done.
∗ P < 0.05 compared with NP in group 2.
Patients ranged in age from 8 months to 9 years (average 4 years 6 months), and 27 were girls. Six children in group 1 and 5 in group 2 attended a day care center. Patients were included in the study if they had no evidence of a nasal foreign body and had received no antimicrobial therapy within the previous 4 weeks. Excluded were patients who had or were suspected of having any other respiratory tract infection that would justify antimicrobial therapy. These included sinusitis, otitis media or purulent pharyngitis, bronchitis, or pneumonia.
Nasal secretions were aspirated into a sterile container by use of a plastic catheter. The secretions were rinsed from the catheter with 2 mL of sterile saline solution and were immediately processed for quantitative cultures for recovery of aerobic and anaerobic bacteria. 12 , 13 NP samples were obtained by sterile cotton swabs that were immediately processed for semiquantitative cultures for aerobic and anaerobic bacteria.
Recovery of organisms with interference capability from the nasopharynx of children in the first NP culture
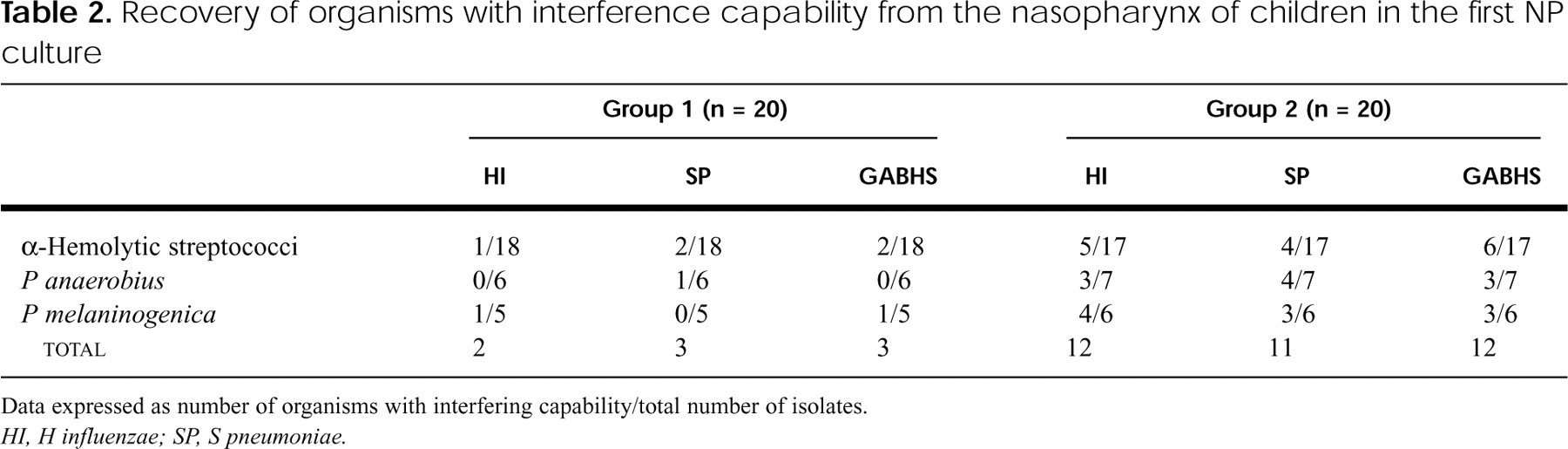
Data expressed as number of organisms with interfering capability/total number of isolates.
HI, H influenzae; SP, S pneumoniae.
Sheep blood (5%), chocolate, and MacConkey agar plates were inoculated for the isolation of aerobic organisms. The plates were incubated aerobically at 37°C (MacConkey agar) and under 5% CO2 (blood agar and chocolate agar) and examined at 24 and 48 hours. For anaerobic cultures, the specimens were inoculated onto prereduced vitamin K1-enriched Brucella blood agar, onto blood agar containing kanamycin and vancomycin, into an anaerobic blood plate containing phenylethyl alcohol, and into enriched thioglycolate broth. These media were incubated in GasPak (BBL Microbiology Systems) jars at 37°C and examined at 48 and 96 hours of incubation at 37°C. The thioglycolate broth was incubated for 14 days. Anaerobic bacteria were identified by techniques described previously. 12 Aerobic bacteria were identified with conventional methods. 13
β-Lactamase activity was determined on 5 colonies of each morphological type by the chromogenic cephalosporin analog 87/312 method. 14 Statistical analysis was done with the Student t test of independent means.
To test for interference, the inhibitory activities of 3 types of organisms known to possess inhibitory activity 7 – 10 were evaluated: α-hemolytic streptococci, P anaerobius, and P melaninogenica. Their inhibitory activity was tested against one strain each of a recent clinical isolate of S pneumoniae, H influenzae, and group A β-hemolytic streptococci (GABHS).
The inhibitory activity of each strain recovered from each patient was individually tested against the test organisms with Steer's steel pin replicator as previously described. 15 In brief, minidrops of log-phase broth cultures of vitamin K1-enriched Brucella media were transferred with the pin replicator to blood or chocolate (for H influenzae) agar plates and allowed to dry for 15 minutes at room temperature. A sample of a log-phase broth culture of the patient's strain (the target strain) was applied adjacent to each of the isolated strains, and the plates were incubated in 5% CO2 or anaerobically (for P melaninogenica) at 37°C for 48 hours.
RESULTS
The patients in group 1 had higher rates of recovery of S pneumoniae and H influenzae in their initial NP cultures than those of group 2. Aerobic and anaerobic microorganisms were isolated from all NP cultures (Table 1). Bacterial growth was present in only 8 (40%) NDs of group 2. Even though only 7 (35%) of the clear group 1 NDs showed bacterial growth, the number increased to 14 (70%) at the mucoid stage and 20 (100%) at the purulent stage. The number of positive cultures declined to 6 (30%) at the final clear stage in group 1.
The number of species and total number of organisms isolated (per milliliter) also increased over time and then declined in the ND of group 1. The average number of organisms increased from log10 2.3 (±0.6) at the clear stage to 5.4 (±1.2) at the purulent stage and then declined. Similarly, the number of bacterial species recovered increased from 16 (clear stage) to 80 (purulent stage).
During the purulent stage, Peptostreptococcus species were isolated in 15 (75%), Fusobacterium species in 10 (50%), Prevotella species in 9 (45%), S pneumoniae in 6 (30%), and β-hemolytic streptococci in 5 (25%) of group 1 NDs. This recovery rate was higher than the rate at the clear stages of both groups and the mucoid stage of group 1. Staphylococcus aureus was isolated in ND and not in the NP in group 1, and the number of isolates did not vary between the stages of the infection. It was, however, recovered from NP and ND of group 2. Propionibacterium acnes and Corynebacterium species were isolated in higher numbers in group 2 NPs than in group 1 NPs (P < 0.05).
β-Lactamase production was noted in isolates of H influenzae, M catarrhalis, S aureus, Fusobacterium species, Prevotella species, and Porphyromonas asaccharolytica.
Although there were no differences in the recovery of α-hemolytic streptococci, Peptostreptococcus species, and Prevotella species, the recovery of those with interfering capabilities differed among the groups. A total of 8 interfering organisms were isolated from the first NP culture of group 1, as compared with 35 from group 2 (P < 0.001) (Table 2).
DISCUSSION
The results of this study confirm, as was previously shown, the recovery of the potential oropharyngeal pathogens S pneumoniae, H influenzae, and β-hemolytic streptococci in more than 75% of patients with purulent nasal discharge. 16 – 20 This report illustrates for the first time the rare recovery of these organisms in patients in whom purulent nasal discharge did not develop. It also illustrates, for the first time, that the development to a purulent stage is associated with the pre-existing presence of these organisms in the NP of the patients. This was associated with a decrease in the recovery of organisms with interfering capabilities in these patients. In contrast, patients in whom potential respiratory pathogens are not colonized, but in whom interfering bacteria or nonpathogens such as P acnes and Corynebacterium species are colonized, are not prone to development of purulent nasal discharge.
In addition to the higher recovery of the above aerobic organisms during the purulent stage, several anaerobic organisms were also found in more than 75% of the patients, confirming our previous observation. 18 These included Peptostreptococcus species, Fusobacterium species, and pigmented Prevotella and Porphyromonas species, all members of the oral flora. Because their increased recovery was associated with isolation of S pneumoniae, H influenzae, and β-hemolytic streptococci, their role in the inflammation may be secondary.
The presence of organisms with interfering potential may play a role in the prevention of respiratory infection. Bernstein et al 9 found a significantly greater number of colonies of α-hemolytic streptococci in the adenoids of non-otitis-prone children than in the adenoids of otitis-prone children. In contrast, they concomitantly recovered a higher number of non-type-B H influenzae in the otitis-prone group than in the non-otitis-prone group. These findings suggest the potential protective nature of α-hemolytic streptococci with inhibitory activity in preventing otitis media.
The ability of the indigenous normal nasopharyngeal flora to inhibit colonization with potential pathogens has been studied previously. 7 – 9 , 21 , 22 α-Hemolytic streptococci has been found to inhibit colonization in patients and in vitro growth of a variety of pathogenic bacteria. These include S pneumoniae, GABHS, and S aureus. 7 – 9 , 21 , 22 The production of bacteriocin and other inhibitory substances that suppress some bacterial growth or utilization of nutrients in the nasopharyngeal environment essential for the potential pathogens may explain this phenomenon. 23 Organisms other than α-hemolytic streptococci may also interfere with the growth of potential pathogens. 10
The cause of nasopharyngitis in our patients was not completely determined because no viral cultures were taken. However, the recovery of several aerobic and anaerobic bacteria not generally found as part of the nasal flora, in patients with purulent nasopharyngitis, may signify their potential pathogenic role. The concomitant presence of these organisms in the inflamed pharynx supports the concept of a generalized inflammation that also involves the nasal spaces.
Controversy exists regarding the management of purulent nasal discharge. Some clinicians regard it as a self-limited phase of viral infection, which does not require specific therapy, whereas others recommend performing nasal culture to detect GABHS and initiation of antimicrobial therapy if the nasal discharge continues for more than 10 days. 24
Todd et al 4 attempted to modify the progress of purulent nasopharyngitis by using cephalexin. Although some bacterial strains susceptible to cephalexin were identified, the clinical outcome was not affected. However, because the antibacterial spectrum of cephalexin is limited, these researchers suggested the need for further studies to investigate the therapy of nasopharyngitis with antimicrobial agents with wider spectra of activity.
Steinweg 25 studied children with either clear or purulent nasal discharge and found no difference in the duration of illness or rate of complication. Wald 24 reported a small study of 13 patients with purulent nasal discharge who were treated with either amoxicillinclavulanate or placebo. Five of the 6 who were given the antimicrobial had complete resolution of their infection within 10 days, compared with only 2 of the 7 given placebo (P < 0.05).
Kaiser et al 26 studied the efficacy of amoxicillinclavulanate compared with placebo in 300 adults with nasal congestion and rhinorrhea. They found that of the 61 patients whose cultures tested positive for S pneumoniae, H influenzae, and M catarrhalis, the antimicrobial therapy produced a significant clinical response in all. However, no difference was noted in the response of the patients without these organisms. The authors concluded that these potential pathogens were the cause of the symptoms in this subgroup of patients. However, in a commentary to that study, Wise 27 cautioned clinicians from routinely administering antimicrobials to patients with the common cold because such an approach would only increase the resistance to antimicrobial agents in the community and would provide only minimal benefit to the patients.
Although an association was found in our study in children between the pre-existing NP colonization with potential pathogens and uncomplicated purulent nasopharyngitis, no evidence exists to date that administration of antimicrobials will shorten the illness. Further studies are needed to explore whether prevention of colonization by vaccination, active colonization of the oropharynx by interfering organisms, or utilization of antimicrobials can provide the patients with clinical benefit and prevent complications.
We thank J. Perry for laboratory support and Joanie Pietrafitta for secretarial support.