
Abstract
BACKGROUND: Epiphora is an annoying symptom, embarrassing the patient both socially and functionally. The two widely accepted treatment modalities of epiphora resulting from obstruction of the nasolacrimal ductus are external and endoscopic dacryocystorhinostomy (DCR).
OBJECTIVE: The aim was to compare the results, operative time, and complications of external and videoendoscopic endonasal DCR performed between December 1994 and December 1998.
METHODS: In group 1, conventional primary external DCR with or without silicone tube intubation was performed in 79 patients (66 women and 13 men) with unilateral dacryocystitis. In group 2, endoscopic primary endonasal DCR with hammer-chisel removal of bone located over the lacrimal sac was performed in 51 eyes of 36 patients, 33 women and 3 men (15 bilateral procedures).
RESULTS: The follow-up period was 6 to 48 months (mean 25 months) after surgery. The age range was from 4 to 76 years (mean 38.5 years). The success rates of external and endoscopic hammer-chisel DCR were found to be 89.8% and 88.2%, respectively. A lower complication rate was observed in the endoscopic group, with minimal morbidity and shorter operative time compared with the external approach.
CONCLUSIONS: Hammer-chisel endoscopic DCR is practical, less traumatic, less time-consuming, and cosmetically more convenient than the external approach. The success rate of the endoscopic DCR procedure is comparable with that of traditional external DCR, and it also allows simultaneous correction of any intranasal pathology. Otolaryngol Head Neck Surg 2000;123:488-91.
To determine the success rates and complications of external and endonasal DCR, we prospectively evaluated the results of 115 patients who had undergone DCR for the treatment of nasolacrimal duct obstruction.
METHODS AND MATERIALS
A series of 115 patients (130 eyes) underwent surgical operation for distal nasolacrimal duct obstruction from December 1994 to December 1998. The results of 79 patients with unilateral dacryocystitis (79 eyes) operated on externally (group 1) were compared with those of 36 patients with dacryocystitis (21 unilateral + 15 bilateral = 51 eyes) operated on endonasally with endoscopic hammer-chisel DCR (group 2). In bilateral cases, each site was considered a separate eye.
In all patients included in this study, the diagnosis of lacrimal obstruction distal to the common canaliculus was made by dacryocystography. In group 1 the predisposing cause was nasal allergic rhinitis in 2 cases and trauma in 1 case, and in 76 cases it was idiopathic. In group 2, it was trauma in 1 case and nasal allergic rhinitis in 2 cases, and in 44 cases it was idiopathic. Four cases showed anterior ethmoidal and maxillary sinusitis. In initial evaluation, the presenting symptom was epiphora in 43 of 79 eyes (54.4%) and recurrent dacryocystitis in 36 (45.6%) in group 1. Of 51 eyes in group 2, 30 (58.9%) had epiphora and 21 (41.1%) had recurrent dacryocystitis, with 1 patient presenting with a concomitant periorbital cellulitis.
In preoperative assessment, all patients underwent a complete ophthalmic and ENT examination, and the lacrimal obstruction was confirmed by a lacrimal irrigation study. The radiologic assessment included lipiodol dacryocystography in all and CT in 13 cases. Particular attention was paid to intranasal pathologies, especially in group 2. Any sign of sinusitis or chronic mucosal inflammation would have required an ethmoidal or middle meatal surgery. In addition, in group 2 significant septal deviation (17 cases) that obscured the visualization of the lateral nasal wall was corrected simultaneously with endoscopic limited septoplasty to reach the sac area easily and to make postoperative care easier. In 4 cases with sinusitis a limited endoscopic ethmoidectomy and middle meatal antrostomy were simultaneously included in the treatment of NLD obstruction.
External operations were performed by ophthalmologists using the technique of Dupuy-Dutemps-Bourget.
SURGICAL TECHNIQUE
With the patient under general anesthesia, the nasal cavity was decongested for 5 minutes with cotton pledgets soaked in topical 2% lidocaine with epinephrine (1:100.000) and 0.025% xylometazoline. The lacrimal sac was irrigated before surgery with a mixture of saline solution and diluted antibiotics if it was infected. A 1-cm 2 area just anterior to the attachment of the middle turbinate on the lateral nasal wall was infiltrated with 2% lidocaine with epinephrine (1:100,000). The mucosa in this region was incised with a sickle knife and excised from the lateral nasal wall. Then, a chisel is placed just anterior to the maxillary line, and the lacrimal bone facing the lacrimal sac was fractured gently with a chisel. Once the bone facing the lacrimal sac was fractured, it is elevated by use of the maxillary crest as a hinge to dislocate the fractured bone. After removal of the fractured bone with a Blakesley forceps, identification and control of the intranasal position of the lacrimal sac were achieved in early cases by introducing a lacrimal probe through each canaliculus and gently pushing it while the surgeon looked through the endoscope. Once the exact location of the sac was verified by tenting of the medial wall of the sac by the lacrimal probe, the medial wall of the sac was incised with a sickle knife and excised with a Blakesley forceps or the flap placed inferiorly. In the endoscopic group, a 20-gauge light probe was used to delineate the exact location of the sac area at the beginning of the operation. This further facilitated the hammer-chisel technique bone removal by defining the precise location of the sac. Silastic tubes attached to the stainless-steel probes (Lacrimal intubation set, 5013; Visitec, Warks) were introduced in each canaliculus in all cases (as in group 1) and were retrieved under endoscopic visualization. Both ends of the silicone tubes were fastened with multiple knots intranasally and sutured to each other with a 5.0 Prolene suture and left in the nasal cavity until this silicone tube was removed. The operation was completed by removal of any remaining blood clots and secretions from the rhinostoma site.
In both groups, postoperative topical and broad-spectrum systemic oral antibiotics were administered. The nasal packings, if applied (applied only in simultaneous endoscopic septoplasty), were removed 48 hours after surgery. In addition, nasal saline irrigation 4 to 5 times a day for 1 week was performed to prevent crusting and to promote good mucosal healing. In the following period, the patient was seen several times for the first 15 days in the office to remove the accumulated crusts or to treat any granulation.
Complications of external DCR
RESULTS
Patients were followed-up for 6 to 48 months (mean 25 months) after surgery. In group 1 there were 66 women and 13 men from 4 to 76 years of age (mean 39.6 years). In group 2 there were 33 women (bilateral in 15 cases) and 3 men from 17 to 67 years of age (mean 37.8 years).
External DCR was successful in 71 of 79 eyes (89.8%) in group 1 and 45 of 51 eyes (88.2%) in group 2. The success rate was comparable between the two groups. Four patients who had endoscopic revision of the failed external DCR during this period were also included in this study. Success is defined as resolution of epiphora and chronic dacryocystitis as well as patent irrigation of the lacrimal system within 6 months after surgery. In 1 unilateral case in group 2, the irrigation of the lacrimal system was patent but not adequate; as a consequence, the patient had epiphora only on exposure to wind and cold.
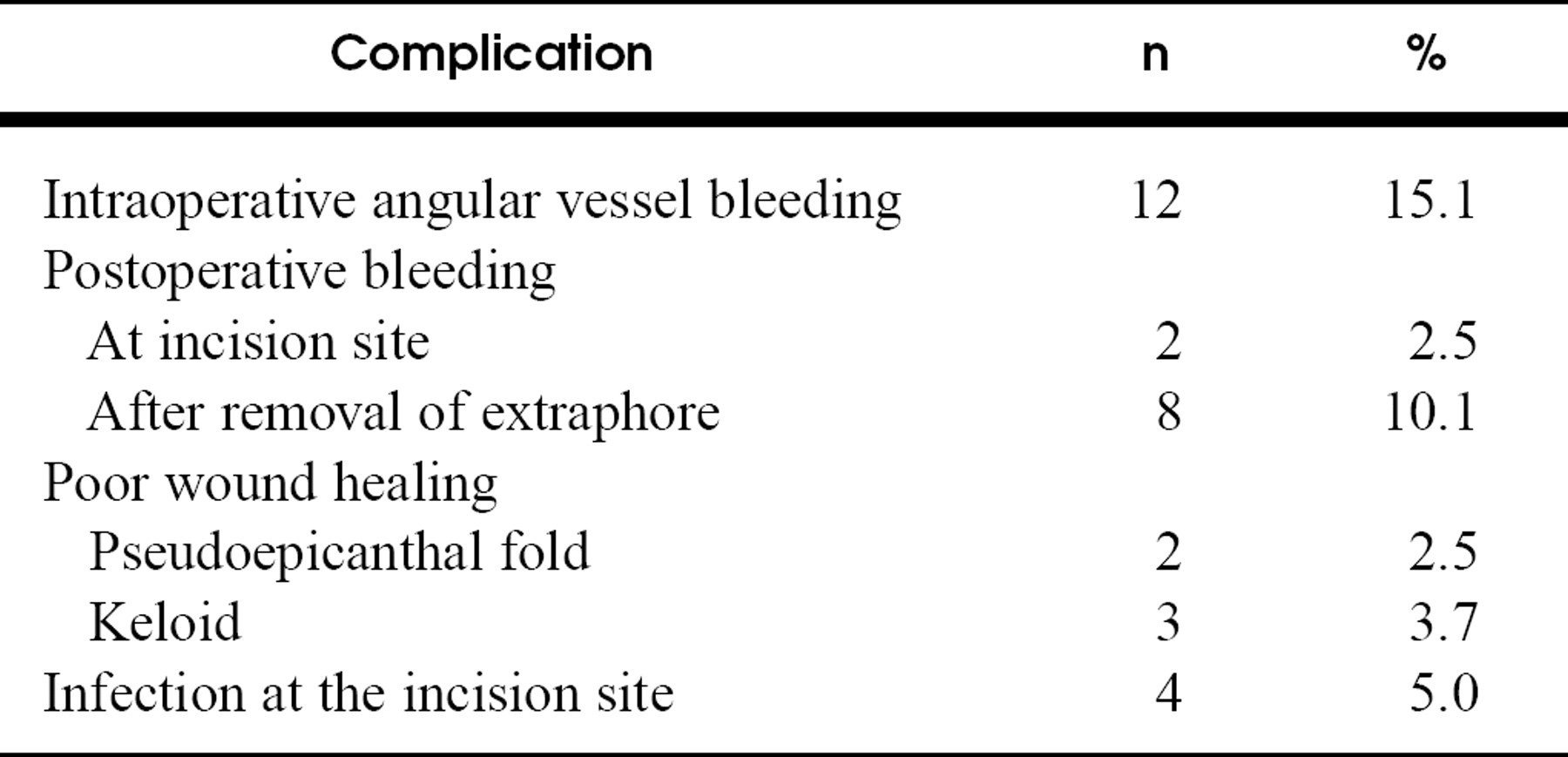
The tube remained in place longer in earlier cases (4-6 months) in both groups but generally was taken out within 2 to 3 months later according to the patient compliance and granulation formation at the ostium. In group 1, excessive intraoperative hemorrhage (from angular artery and vein laceration) occurred in 12 eyes, postoperative keloid formation in 3 eyes, and pseudoepicanthal fold in 2 eyes Table 1. On the other hand, in group 2 mild mucosal bleeding occurred in 8 cases but did not prevent a successful endoscopic hammerchisel DCR. In 3 cases little synechiae were observed between the middle turbinate and the lateral nasal wall or the septum, which were corrected at postoperative visits. The operative time was 50 to 120 minutes (mean 65 minutes) for group 1 and 15 to 105 minutes (mean 33 minutes) for group 2.
DISCUSSION
DCR is the treatment of choice for epiphora in cases of obstruction distal to the common canaliculus. DCR is performed through either an external (Toti's operation) or an endonasal endoscopic approach to make an anastomosis between the lacrimal sac and the nasal cavity. During the past several years, minimally invasive surgical techniques have been increasingly applied to a growing number of surgical specialties. Numerous technologic innovations, especially of endoscopic visualization systems, have made this possible. This especially is true for lacrimal duct surgery. During the past decade, procedures have been introduced that include endoscopic intranasal DCR with or without laser, microendoscopy of the lacrimal drainage system, and balloon dacryocystoplasty. 5,9 External DCR, however, still remains the most established reference treatment modality for NLD obstruction, with endonasal endoscopic DCR closely following it in success. Compared with those of the external approach, the advantages of intranasal DCR are minimal morbidity; less intraoperative bleeding; shorter operative time; preservation of pump function of the orbicularis oculi muscle, presaccal fibers, and medial canthal tendon 10 ; and a better cosmesis, which is important for some patients, especially in this female-dominant patient group. 11
Endoscopic DCR has been known to have some disadvantages, such as small opening size, high recurrence rate, and high equipment cost; it can also be difficult to learn. 12,13 Even with these disadvantages, the absence of an external scar, short recovery period, minimal morbidity (only to the intranasal rhinostoma opening), and low complication rate have made endoscopic DCR popular. Because of the minimal morbidity, 15 bilateral cases underwent surgery in the same sitting with excellent patient compliance. The endoscopic approach also allows diagnosis and management of the predisposing or concomitant nasal and paranasal sinus disorders. Three patients in this series were treated simultaneously for anterior ethmoidal and maxillary disease.
In endoscopic DCR, before the presumed sac wall is opened, it is important to determine the exact location of the sac intranasally to prevent any damage to the globe. To locate the sac before opening the medial aspect of the sac early in our endoscopic series, we tented the medial aspect of the sac by inserting a probe through the puncta. Lately, use of a 20-gauge endoilluminator inserted through the puncta has made it possible to identify the sac even before the bony window is opened and helps to locate exactly where the bony window can be opened safely.
Various endoscopic techniques have been used to remove lacrimal bone and the thick bone of the maxilla forming the anterior lacrimal crest. 12,14 Removal of the thick bone along the anterior edge of the lacrimal sac is important to achieve unobstructed lacrimal drainage. Use of the laser for this purpose necessitates sophisticated instrumentation and training and adds extra cost and its related potential complications and hazards. 13 Bone removal with the laser is tedious and has been associated with a higher rate of recurrence. Concomitant use of a drill or rongeur is advocated to obtain a larger rhinostoma and prevent reclosure. 12,14,15 The depth of laser penetration can also be unpredictable depending on many factors. Laser beam targeted to the globe is an overt risk and necessitates extra care to prevent any harm to the globe. 5
Drilling of the bone over the lacrimal sac is technically challenging because of the narrow confines of the sac location and because meticulous care is necessary to control a powered instrument. Metson et al 16 stated that drilling can be tedious and result in bleeding. Scarring of the ostium and errors in ostium location are the major causes of surgical failure. 14,17 In this study the hammerchisel endoscopic technique achieved a fast and practical removal of bone with no need for sophisticated, expensive instruments such as are needed for laser-assisted endoscopic surgery. Compared with drilling, this procedure was atraumatic and very simple and controllable.
Epithelial anastomosis and continuous fluid flow are necessary for maintaining a patent surgical rhinostoma, and both require silicone stent placement. 15 Three of the failures in the second group coincided with premature tube dislodgment. Regarding tube retention, Kong et al 12 suggested removal of the tube before 8 weeks to prevent granuloma formation. However, we had 3 failures accompanying 2 accidental and 1 intentional premature removals of the tube by patients. This suggests that the tube should be kept in place for at least 2 months. A strong relationship between tube retention and success has also been observed by Boush et al. 14 This issue needs to be studied further to define optimum time for tube removal. Most surgical failures occur between 2 and 6 months. 12,14,18 In this study closure of the osteotomy site with granulation tissue occurred in 7 eyes in group 1, and gradual closure of the rhinostoma site occurred in 6 eyes in group 2 between 1 and 2 months.
Revision of the primary external operations with the endoscopic technique is successful, but the success of endoscopic revision of the primary endoscopic DCR is controversial. Metson et al 16 reported reclosure of 4 endoscopic revisions of 5 failed endoscopic DCRs. Boush et al, 14 on the contrary, reported 5 successes in endoscopic revision in 6 primary endoscopic failures. In our cases, postoperative persistence of the patency was observed in 4 cases of external DCR failure, whereas in 5 endoscopic DCR failures that occurred early in group 2 and that were revised externally, 4 remained patent and 1 reclosed in a month.
The success rate of traditional primary external DCR with or without a mucosal flap is 85% to 99% 9,19,20 based on the experience of the surgeon. Our results in group 1 (89.8%) were similar to these values. On the other hand, the success rates of primary endoscopic laser/drill DCR series were reported to be 80% to 82%, 15,19 and our endoscopic DCR results (88.2%) were similar to the external results and to those of previous studies. 12,14,15,17,21 All endoscopic DCRs were performed by the same surgeon (Y.C.), who was previously experienced in endoscopic paranasal surgery, whereas the external approaches were performed by different surgeons including residents in training. Most of the failures in group 2 (4 of the first 12 eyes) occurred in the first 12 cases. This suggests a learning curve in endoscopic DCR, the external approach still remains the reference surgical technique for the treatment of NLD obstructions.
Endoscopic endonasal DCR is recommended as a primary surgery for NLD obstruction. In the case of a failed primary external DCR, with minimal intraoperative bleeding, short operative time, preservation of the lacrimal pump mechanism of the orbicularis oculi muscle, and cosmetic convenience, the success rate of endonasal endoscopic DCR compares with that of external DCR.