
Abstract
The effects of otolith stimulation on systolic blood pressure (SBP) and R-R interval fluctuations were investigated in 12 healthy subjects and 5 patients with loss of labyrinthine function. The vestibular otolith organs were stimulated by centrifugal forces, the constant rotation of a chair fixed outside of the rotation axis on the horizontal plane. The chair was fixed along the direction of centrifugal force (eccentric rotation (ECR)) or along the tangent line (eccentric lateral rotation (ECLR)). The ECR stimulates both the utricular and saccular maculae, whereas the ECLR stimulates only the utricular maculae. Spectral analysis showed that in the healthy subjects, low-frequency SBP increased significantly during ECR but not during ECLR. There was no significant increase in low-frequency SBP in patients with labyrinthine loss. In the R-R interval analysis, however, the low- and high-frequency components did not change significantly in the healthy subjects during ECR. Our findings indicate that stimulation of the otolith maculae, especially the saccular organs, predominantly produces augmentation of the α-sympathetic activities rather than cardiac sympathovagal outflow to the heart.
Spectral analysis of the R-R interval and arterial BP is an invaluable noninvasive tool, used successfully to quantitatively evaluate changes in neural activities in the sympathetic and parasympathetic branches of the autonomic nervous systems. In this study, movement of a rotational chair positioned away from the axis of rotation was used to stimulate the otolith organs: (1) centrifugal force along the naso-occipital axis (eccentric rotation [ECR]) stimulates both the saccular and utricular maculae, and (2) centrifugal force along the interaural axis chiefly stimulates the utricular maculae (eccentric lateral rotation [ECLR]). 10 The purpose of this study was to clarify the characteristics of otolith-autonomic responses by comparing the R-R intervals and BP power spectra across different linear acceleration conditions (ECR and ECLR) in healthy subjects and in patients with loss of bilateral labyrinthine function.
METHODS AND MATERIAL
The power spectra of the R-R intervals and systolic BP (SBP) were analyzed in 12 healthy subjects and 5 patients with loss of bilateral labyrinthine function. The healthy subjects were selected from volunteers from our laboratory staff who had no history of otologic or neurologic disease, no evidence of metabolic disease on routine blood examination, and no neurophysiologic deficits during physical examination. The mean age of the healthy subjects was 31 ± 8 years, mean SBP 123.4 ± 6.1 mm Hg, mean diastolic BP (DBP) 67.3 ± 4.7 mm Hg, and mean R-R interval 904 ± 39 ms. The patient group had bilateral otolith insufficiency as defined by rotational and caloric electronystagmography findings: (1) no VOR responses in the centric and eccentric pendular rotation tests, a useful technique used to evaluate otolith function 10 ; and (2) absence of bilateral caloric responses during ice-water irrigation at 4°C. The mean age of these patients was 36 ± 11 years, mean SBP 126 ± 8 mm Hg, mean DBP 69 ± 19 mm Hg, and mean R-R interval 879 ± 27 ms. No one was receiving an α- or β-blocker or any other medical treatment, and no one had cardiac, metabolic, or additional neurologic disease. The causes of otolith function loss were labyrinthitis (n = 3), congenital deficit of unknown origin (n = 1), and ototoxicity (n = 1). Patients were given a full explanation of the experimental procedure, and written, informed consent was obtained from each. This study was approved by the institutional review boards of Osaka University.
Effects of ECR
Studies were performed in a quiet, dark room. Subjects were seated upright in a rotational chair mounted on a computer-controlled direct drive motor (T-12008, Inland, UK). Each subject's body and head were restrained with shoulder and lap belt harnesses and a custom-built head holder. The chair was placed 0.9 m from the axis of rotation toward the subject's naso-occipital direction and rotated for 8 minutes at 20°/second, 50°/second, and 80°/second (ECR). It was then turned 90° along the direction of the tangent line and rotated again at the same velocities (ECLR). To identify any potential order effects, we did ECLR before ECR for 5 of the 12 healthy subjects. The linear centrifugal forces were 0.01g, 0.07g, and 0.17g. After the experiment, the subjects were asked about motion sickness symptoms (ie, nausea, vomiting, pallor, and sweating). None of them had any sign of motion sickness during or after eccentric rotation.
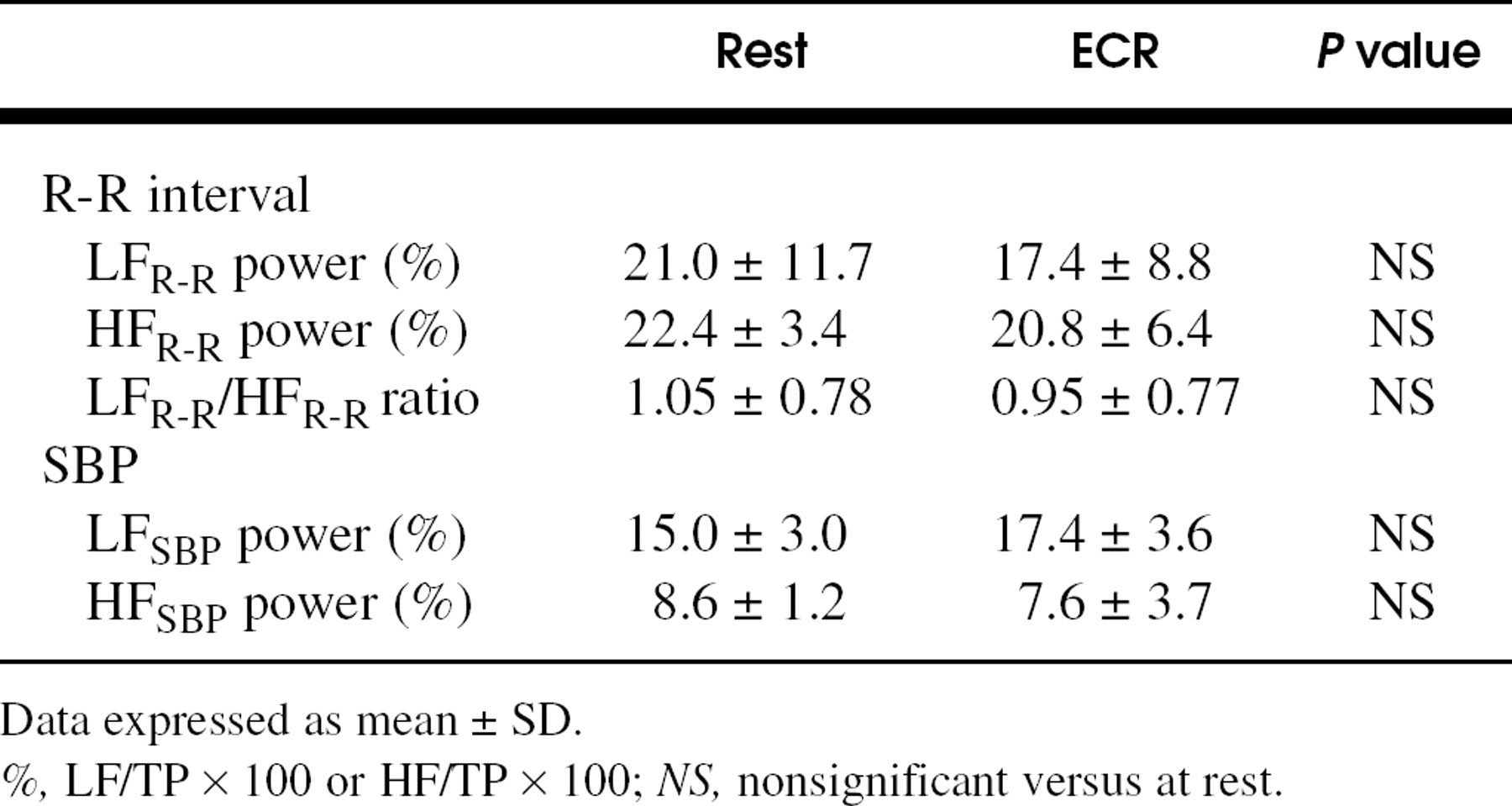
Power spectral analysis of the R-R interval and SBP variabilities in healthy subjects and labyrinthine-deficient patients in the resting condition
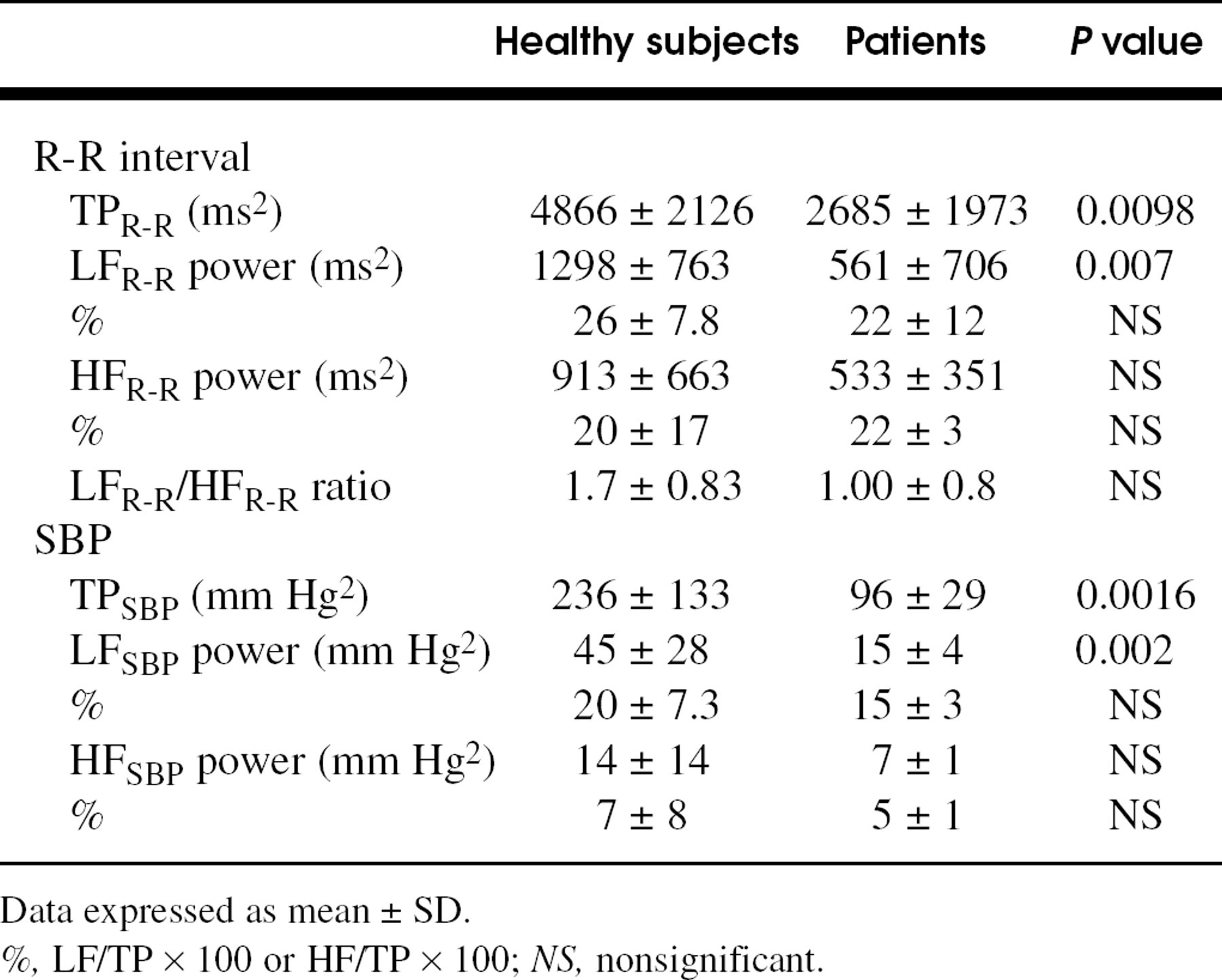
Data expressed as mean ± SD.
%, LF/TP × 100 or HF/TP × 100; NS, nonsignificant.
BP and heart rate (HR) were monitored continuously from the middle finger of the right hand with a Finapres device (model 2300; Ohmeda, Englewood, CO). Respiratory movements were monitored with a mercury-in-Silastic gauge connected to a plethysmograph. The subjects were instructed to listen to a tone given through a loudspeaker placed 3 m in front of them and made to maintain a fairly steady respiratory movement (10-12 breaths/minute).
After confirming the stability of the BP and R-R interval fluctuations, the analog output from the Finapres was connected to an analog/digital converter for the collection, storage, and analysis of the data by a personal computer (NEC 9801) equipped with Lab View software. The analysis of data during rotation eliminated the first minute after the start of rotation to minimize effects of the stimulation of the horizontal semicircular canals. Data were processed using an algorithm to detect both the SBP and DBP in a 1-second window. R-R was detected as intervals between consecutive R waves of the QRS complexes. Each distribution was analyzed by a fast Fourier transform algorithm on a 1024-point time series. The theoretical and analytical procedures have been fully described elsewhere. 11-13 The oscillation-scale frequency was analyzed at 0.5 Hz. The total variance (total power [TP]) from 0.01 to 0.5 Hz could be divided into 2 spectral components centered on different frequencies: ranges of 0.04 to 0.15 (low frequency [LF]) and 0.15 to 0.5 Hz (high frequency [HF]). The respective units of power density were as follows: R-R interval, ms2/Hz; and SBP spectrum, mm Hg2/Hz. Each component was expressed as a percentage of TP. In the analysis of the R-R interval, the LFR-R/HFR-R ratio was used as the index of cardiac sympathovagal balance.
Comparison of changes in the power spectra of the R-R interval
All statistical evaluations were made by a statistical analysis system. The analysis of variances was used for the statistical comparisons, and P values less than 0.05 were considered significant by the Scheffé F test.
RESULTS
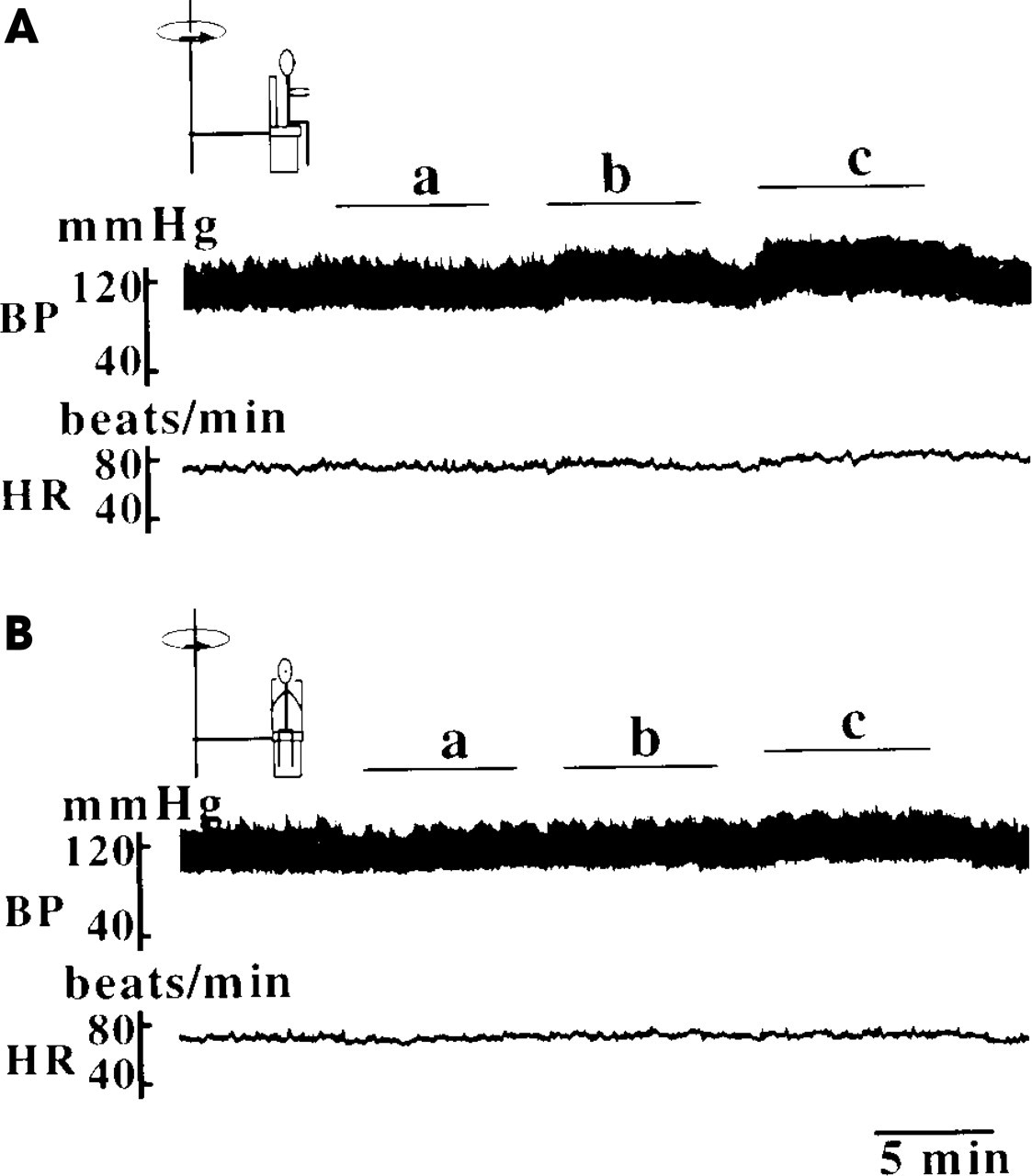
Results of the spectral analysis of the R-R interval and SBP variability at rest for both groups are shown in Table 1. The TP, LF power, and HF power of the R-R interval and SBP were significantly lower in the labyrinthine-deficient patients than in the healthy subjects, but the differences in LF and HF power expressed as a percentage of TP did not reach statistical significance. On R-R analysis, the LFR-R/HFR-R ratio did not show a statistically significant difference. Fig 1 shows the effects of ECR and ECLR on BP and HR in a healthy subject. When the subject was rotated eccentrically at velocities of 50°/second or more while facing outward, the increment in BP observed during rotation returned to the resting level within a few minutes after the rotation ceased (Fig 1 A), but when the same subject was rotated while facing in the tangential direction, the rise in BP was small even at 80°/second (Fig 1 B). The phenomenon was the same regardless of the order in which ECR and ECLR were carried out. No change in HR was observed during eccentric rotations, whereas the increase in BP was minimal.
Sequential changes in HR, DBP, and SBP in healthy subjects during ECR and ECLR (20°/second, 50°/second, and 80°/second) are shown in Table 2. In ECR, at 50°/second and 80°/second SBP and DBP rose significantly as compared with the resting condition (P < 0.01). In ECLR, the rises in SBP and DBP, even at 80°/second, were not significant. No statistically significant differences in HR were detected at any stimulus level.
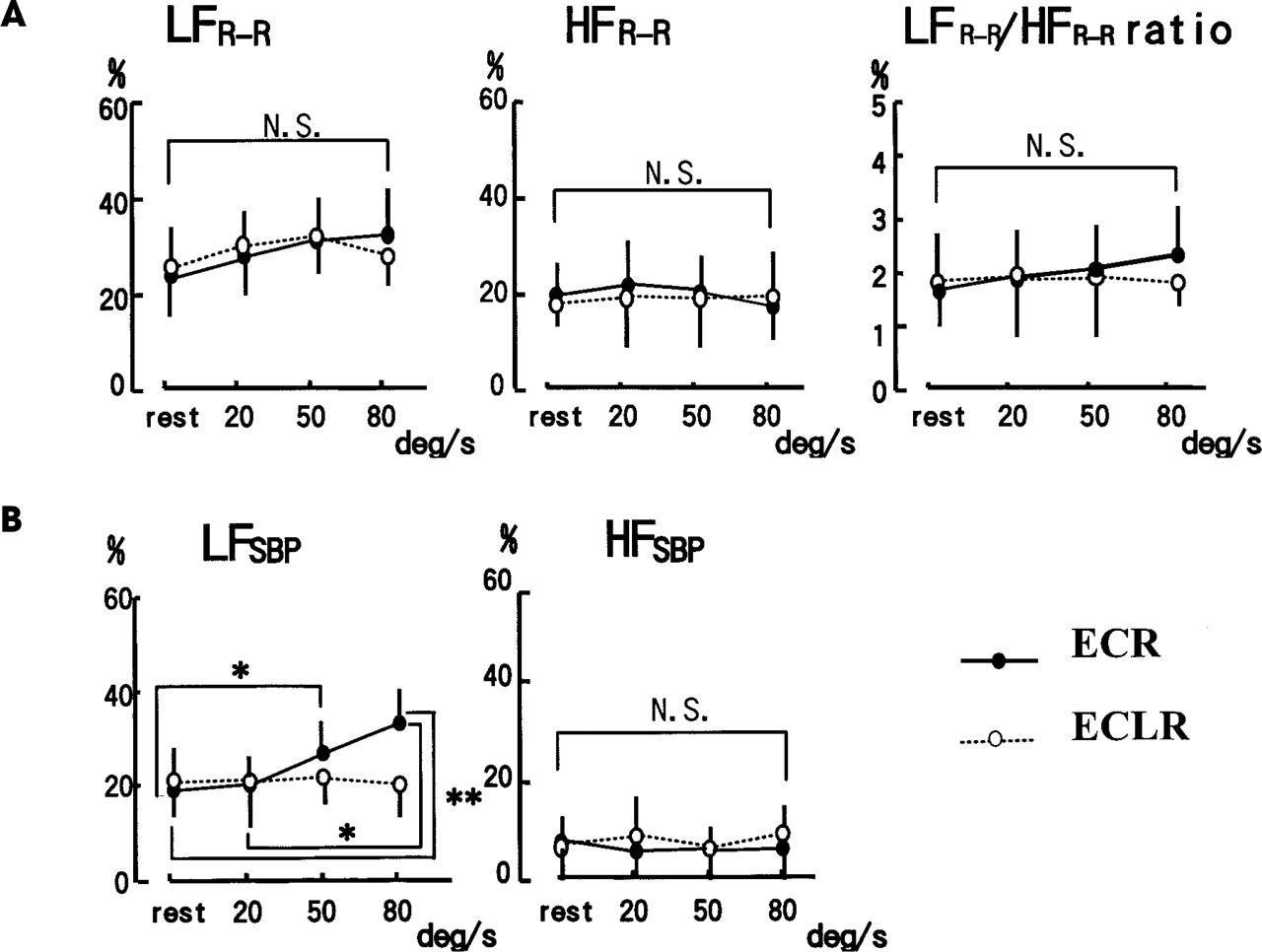
With respect to the spectral analysis of R-R intervals in the healthy subjects, the LFR-R power and the LFR-R/HFR-R ratio tended to increase as the ECR velocity increased, but the differences did not reach statistical significance (Fig 2 A). During ECLR, there were no significant differences in any of the R-R interval parameters. With respect to the spectral analysis of SBP variability, LFSBP power increased markedly during ECR at 50 and 80°/second but was much lower during ECLR (Fig 2 B). In contrast, HFSBP power did not change significantly during ECR or ECLR, remaining within 5% to 10% of TPSBP irrespective of the increase in rotation velocity.
Changes in HR, SBP and DBP in healthy subjects during ECR or ECLR
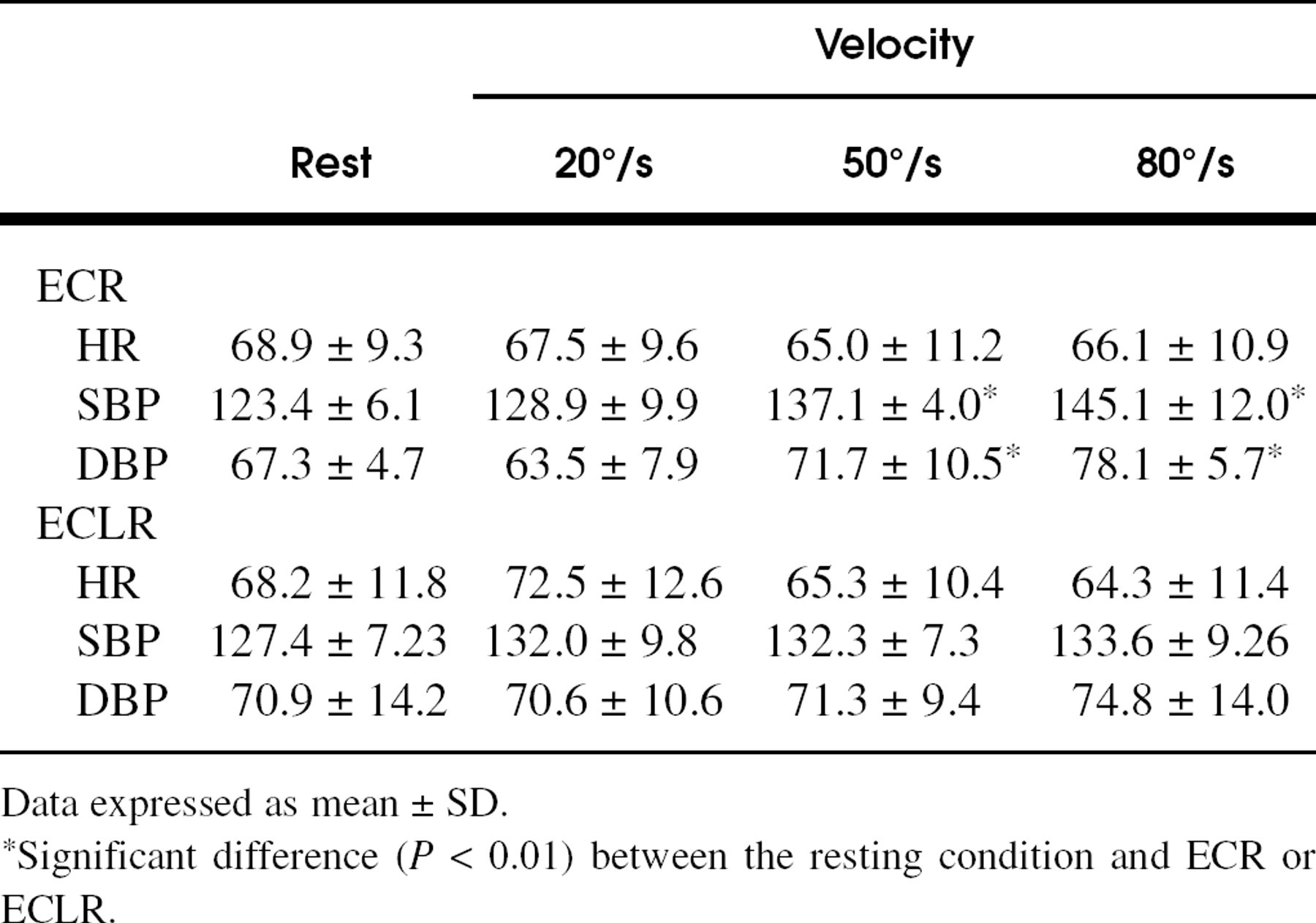
Data expressed as mean ± SD.
*Significant difference (P < 0.01) between the resting condition and ECR or ECLR.
There was no significant difference in BP or HR during the rest condition and ECR (80°/second) in the patients with bilateral labyrinthine function loss. Table 3 shows the power spectra of the R-R interval and SBP variability during ECR (80°/second) and at rest. ECR had no significant effect on the power spectra of LFR-R, HFR-R, LFSBP, and HFSBP.
DISCUSSION
This is the first study in which spectral analysis was used to compare changes in sympathetic and parasympathetic activities during otolith stimulation. In previously reported clinical studies, various parameters (salivation, respiration, BP, HR, and cardiac volume in R-R intervals) have been used to evaluate vestibuloautonomic responses in a microgravitational environment, 3,4,9 but it was difficult to determine whether the response was derived from simultaneous or separate excitation of the sympathetic and parasympathetic systems. Unlike those indexes, spectral analysis of variability in the R-R interval and BP provides considerable information about changes in the autonomic nervous system, including the sympathetic and parasympathetic systems. 11-13
At rest, the magnitudes of the TP, LF, and HF powers in the patients with otolith function loss were significantly small compared with those in the healthy subjects, indicating that patients may manifest a sign of autonomic dysfunction under specific circumstances. 14 Our study also has shown that LFSBP power is increased significantly during ECR. We believe, however, that this increment was not the result of emotional stress or the excitation of other receptors (ie, baroreceptors or myogenic receptors). The reasons for this are as follows: (1) we confirmed that there was not a significant increase in LFSBP power in patients with bilateral labyrinthine function loss during ECR; (2) in this study a mild centrifugal force (≤0.17,g) was used to avoid the occurrence of motion sickness shown by nausea, vomiting, pallor, and sweating; and (3) if the rise in LFSBP is related to mental stress, it usually should be accompanied by marked changes in cardiac sympathetic responses (LFR-R). 15 The rise in LFSBP power therefore presumably is derived from the excitation of otolith organs. In contrast, the LFR-R/HFR-R ratio in the R-R interval analysis, often used as an index of cardiac sympathetic modulation, did not increase during ECR. Stimulation of otolith organs, including the saccular and utricular maculae, therefore may preferentially excite the α-adrenergic system rather than the cardiac sympathetic system. 11
Power spectral analysis of R-R intervals and the SBP variabilities of patients with loss of vestibular function resting condition and during ECR (80°/second)
Data expressed as mean ± SD.
%, LF/TP × 100 or HF/TP × 100; NS, nonsignificant versus at rest.
The fact that the direction of linear acceleration differentially influenced autonomic responses is particularly interesting. The rises in BP induced by ECLR were considerably smaller than those induced by ECR. A similar discrepancy for the direction of linear acceleration has been reported for gastric motilities and gastric electromyography activities. 16,17 The remarkable change in autonomic response therefore appears not to be caused by the dual action of the utricle and saccule, but rather the saccular organs themselves are closely related to the excitation of sympathetic activity. 6
Although the mechanisms and pathways responsible for otolith-sympathetic reflexes have yet to be fully identified, we speculate that the otolith organs have multisynaptic connections with the brain stem structures related to cardiovascular regulation. 7,18 Yates and Miller 19 demonstrated that otolith vestibular stimulation induced excitation of the reticular neurons in the rostral ventrolateral medulla, an important source of excitatory inputs to sympathetic preganglionic neurons. In a clinical study, when the subject's head was flexed downward in the prone position, blood flow to the forearm and calf was reported to decrease rapidly, presumably as a consequence of the increase in sympathetic tone elicited by inputs from otolith receptors. 5
In summary, we showed that the otolith organs, in particular the saccular organs, have excitatory effects on sympathetic outflow. The probability is high that the otolith-sympathetic reflex effectively serves to maintain a more stable BP level for posture movements. 20
The Ninth International Facial Nerve Symposium will be held in San Francisco, CA, July 29-August 1, 2001, at the Hyatt Regency, San Francisco. The Program Chairman is Robert K. Jackler; the meeting is being held in collaboration with the University of California, San Francisco, and the Sir Charles Bell Society.
A program overview includes instructional courses, invited lectures, topical panel discussions, free papers, videotape, and CD-ROM sessions.
Call for abstracts: Please submit structured abstracts using the format specified in the guidelines for authors of the American Journal of Otology. Deadline for submission is March 1, 2001.
CME: 24 hours of category 1 credit accredited by the University of California, San Francisco.
Contact the Office of Continuing Medical Education, University of California, San Francisco, (415) 476-5808 or (415) 502-1795 (fax); e-mail,