
Abstract
Reconstruction of tracheal defects continues to be a difficult problem in head and neck surgery. In this study, to evaluate the outcomes of tracheal reconstruction with a nonautogenous material, we used solvent-dehydrated human costal cartilage in 3 different forms: graft, neovascularized graft, and prefabricated free flap. Thirty-five Sprague-Dawley rats were distributed into 3 groups with 10 animals in groups 1,10 in group 2, and 15 in group 3. Surgically created tracheal defects were repaired with a free cartilage graft in group 1, and a piece of cartilage was neovascularized for 3 weeks in the inguinal region and then used as a fibrovascular tissue-coated cartilage graft in group 2. In group 3, the neovascularized cartilage was transferred to the defect as a prefabricated free flap based on a vascular pedicle containing femoral vessels. Four weeks later, the tracheal reconstruction specimens were evaluated with light microscopy to determine cartilage survival, infection, and epithelial regrowth. The most favorable outcomes were obtained in group 3, where the material was used as a prefabricated neovascularized free flap.
The ideal grafting material for the airway should be a well-vascularized graft, allowing rapid development of mucosa and resistance to infection, resorption, and scarring once it is transferred to the contaminated airway environment. Even in large airway defects, both free and revascularized perichondrial and periosteal grafts have resulted in complete re-epithelization and subsequent bone formation, with stenting applied initially until osteogenesis or chondrogenesis can occur. 7-9 The evolution of microvascular free-tissue transfer has expanded the variety of donor sites and improved the quality of composite tissue grafts available for reconstruction of tracheal defects. 10 With the fairly recent refinement of “flap prefabrication,” there is the possibility of manipulating living tissues and combining those that do not occur together naturally to create a transferable free flap on a reliable, induced vascular pedicle. 11,12 Pregrafting of the flap permits preintegration of the tissue in the flap before its actual transfer, thus obtaining a stable combination that does not occur in normal anatomy. 13 In our study we used solvent-dehydrated human costal cartilage to reconstruct tracheal defects. The cartilage was applied to the tracheal defect in 3 forms: free graft, prefabricated graft, and prefabricated free flap. This allowed us to evaluate the wound healing, adaptation to the recipient site, and surgical outcome of this nonautogenous material in 3 different reconstruction techniques.
METHODS AND MATERIAL
Approval was obtained from the ethics and animal use committee at the Baškent University School of Medicine. The study was conducted on 35 adult male Sprague-Dawley rats weighing between 500 and 650 g. The rats were separated into 3 groups, with 10 animals in group 1, 10 in group 2, and 15 in group 3. The animals were anesthetized by intramuscular injection of a 0.4-mL mixture of ketamine (44 mg/kg) and xylazine (5 mg/kg). Additional injections of 0.2 mL were used as needed to maintain adequate anesthesia and analgesia. An intramuscular injection of a second-generation cephalosporin (Cefobit 100 mg) was administrated to the upper extremity just before the procedure for antimicrobial prophylaxis, and 15 mg twice daily was continued for the next 5 days. The dehydrated human costal cartilage (Tutoplast, dehydrated human costal cartilage sterilized by γ-irradiation) was rehydrated for 12 hours in sterile physiologic serum before the procedure and was then cut into small pieces of approximately 4 × 6 × 2 mm.
Experimental Group 1
The anterior neck region of the 10 animals was shaved, and the skin was surgically prepared with 10% povidone-iodine solution. A vertical incision was made through the skin and the panniculus carnosus. The trachea was exposed on dissection through the strap muscles. A rectangular window of about 3 × 5 mm was made in the anterior wall of the midportion of the trachea. The defect was then closed with a piece of human costal cartilage, which was prepared as a rectangular 2-mm-thick block, slightly larger than the window on the tracheal wall. This was sutured with four 9-0 nylon sutures, one per corner. The strap muscles were reapproximated, and the wound was closed with 4-0 interrupted sutures. Four weeks later the animals were euthanized with an intracardiac injection of potassium hydroxide, and their tracheas were harvested for histopathologic evaluation.
Experimental Group 2
The groin regions of 10 rats were shaved, and the skin was surgically prepared with povidone-iodine solution. A skin incision was made on the groove between the leg and abdomen. After dissection of the panniculus carnosus, the inguinal fat pad was exposed. This pad was cut circumferentially on its medial, lateral, and superior borders and was then elevated as an inferiorly based flap containing the inferior epigastric vessels. A 4 × 6 × 2 mm piece of human costal cartilage was placed over the inferior epigastric vessels, and the fat flap was reapproximated to its original position and fixed with one 6-0 nylon suture. Wounds were closed with 4-0 interrupted silk sutures. After 3 weeks of revascularization, the animals were anesthetized as above, and the neck and groin regions were prepared as before. The graft was found below the inguinal fat pad and dissected out with newly grown fibrovascular envelope around it. A procedure similar to that used in group 1 was performed to open a tracheal window, and the defect was repaired with the neovascularized cartilage graft fixed with four 9-0 nylon sutures. Four weeks later the animals were euthanized with an intracardiac injection of potassium hydroxide, and their tracheas were harvested for histopathologic evaluation.
Experimental Group 3
A neovascularized cartilage graft was prepared for each of the 15 animals with a procedure similar to that for group 2. After 3 weeks the animals were anesthetized again, and their neck and groin regions were prepared as above. After an incision was made in the groin, the inguinal fat pad and the neovascularized cartilage graft were dissected off the tight musculature along with the epigastric vascular pedicle by use of an operating microscope and microsurgical instruments, and the femoral vessels were doubly ligated just distal to the epigastric vessels. The superficial inferior epigastric vascular pedicle was dissected with the femoral artery and vein along their length to the inguinal ligament and then ligated with 9-0 nylon and divided. A vertical incision was made through the skin and the panniculus carnosus in the anterior neck region. On the left side of the neck, the common carotid artery and one of the large neck veins were located by dissection with an operating microscope and microsurgical instruments. The strap muscles were excised to gain better exposure to the trachea. The flap was brought to the neck, and the proximal end of the femoral artery was anastomosed to the common carotid artery in an end-to-side fashion, while the femoral vein was end-to-end anastomosed to the dissected neck vein with 10-0 interrupted nylon sutures. Lidocaine (2%) and warm heparinized Ringer's solution were used for irrigation. After control of hemorrhage and evaluation of vessel patency, a 3 × 4 mm rectangular defect was made on the anterior wall of the midportion of the trachea. The neovascularized cartilage was approximated to the defect with the fat flap and was then fixed to the left edge of the defect with two or three 9-0 nylon sutures. The cartilage was then flipped over the defect, and two or three 9-0 nylon sutures were placed on the right side to fix the flap as an airtight cover. The wound was then closed with 4-0 interrupted silk sutures. Four weeks later the animals were anesthetized as before, and the neck region anastomoses were explored under an operating microscope. After patency tests were carried out on the arterial and venous anastomoses, the animals were euthanized with an intracardiac injection of potassium hydroxide, and their tracheas and accompanying flaps were harvested for histopathologic evaluation.
Specimens were stained with hematoxylin-eosin, and histopathologic evaluation was performed under light microscopy at x40 to x230 magnification.
All histopathologic examinations were performed by the same pathologist (B.D.), and infection, cartilage resorption, and luminal epithelization were assessed with a blind procedure. A semiquantified scoring system was used for assessing epithelial regrowth, and it was judged with a 3-grade scale ranging from 1 (inadequate or absent) to 3 (complete). In the statistical analysis of re-epithelization of the tracheal lumen, cases with inadequate or absent epithelization were compared with cases with moderate or complete epithelization. Also, only severe infections and total or near-total cartilage resorption were regarded as infection and resorption. The histopathologic results of all 3 parameters (infection, cartilage resorption, and luminal epithelization) were evaluated for statistical significance with the Pearson χ2 test. The computer program PC-SPSS (version 7.5) was used in the analysis.
Clinical and histopathologic evaluation of the 3 groups of animals throughout the study
RESULTS
In 2 animals from group 2 and 1 from group 3, cartilage grafts were found to be resorbed after the first stage of neovascularization, and these animals were excluded from the study. One animal in group 1 and 4 in group 3 died during the surgeries. Two animals from group 3 were also excluded from the study because both arterial and venous anastomoses were found to be thrombosed on exploration. As a result, histopathologic evaluation was performed in 9 group 1, 8 group 2, and 8 group 3 specimens. Specimens harvested from the animals that survived reconstructive operation underwent histopathologic assessment for infection, resorption of cartilage graft or flap, and epithelial regrowth. Varying severity of infection was seen in 6 of 9 (67%) group 1 specimens, 4 of 8 (50%) group 2 specimens, and 2 of 8 (25%) group 3 specimens. As well, total resorption of the cartilage graft was seen in 5 of 9 (56%) specimens from group 1 and 2 of 8 (25%) specimens from group 2. None of the 8 group 3 specimens showed such resorption, the cartilage in this group having been transferred as a free vascularized flap. In group 1 the epithelial regrowth in the tracheal lumen was found to be inadequate or absent in all 9 specimens. In group 2 the epithelial regrowth was found to be inadequate or absent in 4 (50%) and moderate in remaining 4 (50%) specimens. Although there was no cartilage resorption, the epithelization was found to be inadequate or absent in 2 (25%), moderate in 2 (25%), and complete in 4 (50%) specimens of group 3. The results of the study are summarized in Table 1.
DISCUSSION
For reconstruction of tracheal defects up to approximately 6 cm in size (less in elderly patients), end-to-end anastomosis is still widely considered the method of choice. It is the consensus that prosthetic reconstruction should be avoided wherever possible. According to Neville et al 14 the ideal prosthesis should be air tight and flexible but not collapsible, completely incorporated into the host tissues with minimal inflammatory reaction, noncarcinogenic, and able to permit ingrowth of respiratory epithelium along the lumen. Among these characteristics, regrowth of normal-looking respiratory epithelium over the prosthesis is regarded as a key ingredient for successful reconstruction. Although more encouraging results have been reported with staged approaches, which involve burying the prosthesis in a subcutaneous pocket before tracheal resection, the epithelium in these cases is generally not confluent throughout the prosthetic lumen. Nelson et al 15 achieved good long-term results with relatively short prostheses (≤3 cm long). More favorable outcomes have been reported with autogenous tissue reconstruction modalities, which result in various degrees of donor deformity and morbidity depending on the method chosen. 8-10
In this study we used a nonautogenous material—solvent-dehydrated, γ-irradiated human costal cartilage—to reconstruct surgically created tracheal defects in rats. Human costal cartilage is a hyaline cartilage, and it possesses a number of favorable characteristics, being firm and constant in form and easy to handle and cut into the desired shape with a sharp knife. Attempts involving direct transplantation of cartilage from a cadaver as an allograft or xenograft, which contains cells, have resulted in rejection and usually complete resorption of the transplant. In solvent preservation of human cartilage, chondrocytes are destroyed and washed out by multiple washings in highly concentrated saline solution, and the original structure of the cartilage is preserved through gentle, progressive dehydration. Sterilization is achieved with γ-irradiation. The process leaves no deleterious residue and eliminates antigenic properties. Also, all tissue procured meets stringent specifications during donor screening and laboratory testing to reduce the risk of infectious disease transmission and bacterial infection. In one animal study, Fini et al 16 found that allogenous grafts were always as well preserved and well integrated with the surrounding tissue as autogenous grafts. In clinical practice, Rettinger 17 has extensively investigated the basis, preservation, and clinical use of cartilage transplants in head and neck surgery and has reported no significant difference between preserved and fresh cartilage with regard to resorption, infection, or distortion. Chaffoo and Goode 18 reported the successful use of irradiated human cartilage for reconstruction of the nose. To our knowledge there have been no reports published to date on tracheal reconstruction with solvent-dehydrated human costal cartilage.
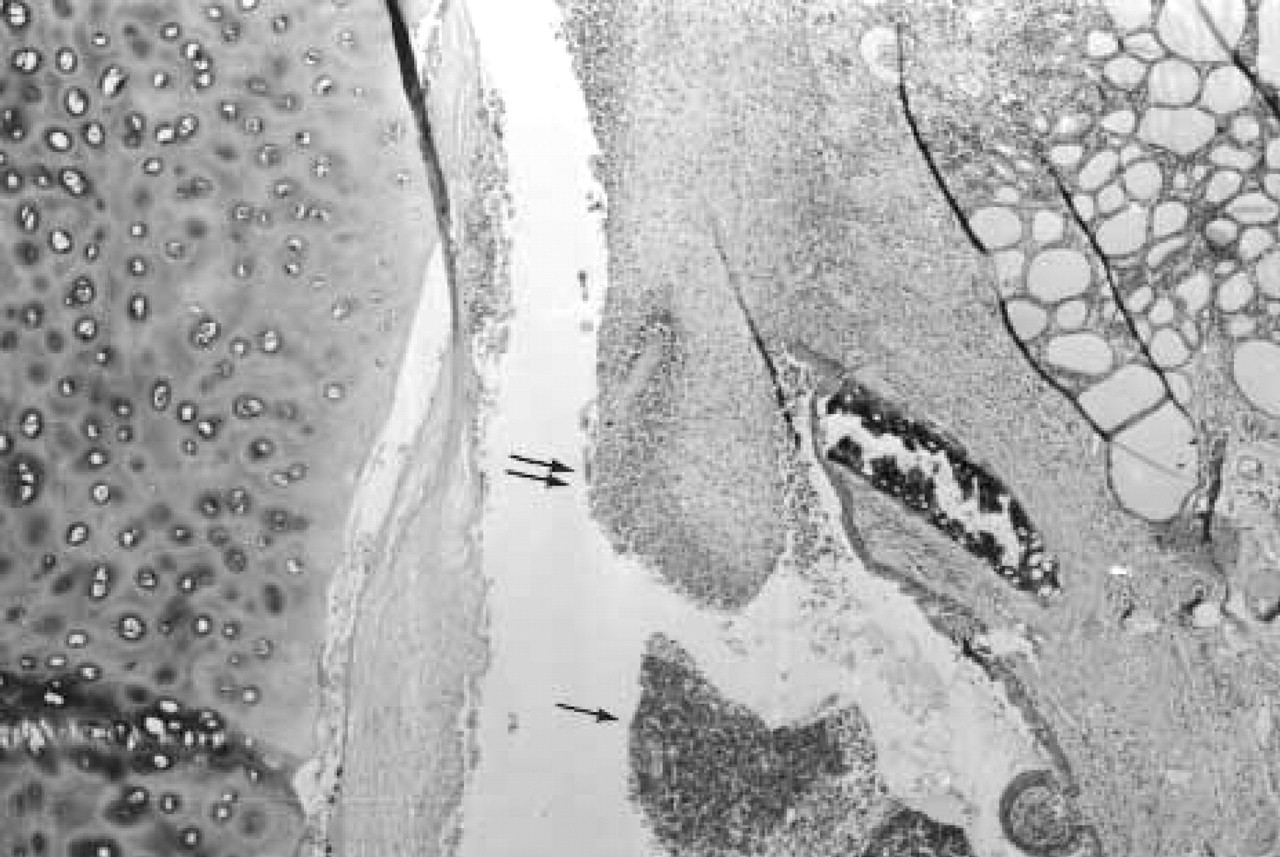
Bacterial colonization (single arrow) and prominent leukocyte infiltration and granulation tissue (double arrow), with inadequate epithelization on the luminal surface of the cartilage graft in a group 1 specimen. (Hematoxylin-eosin; original magnification x40.)
Our study found total cartilage resorption in 5 of 9 (56%) animals in group 1, where the cartilage was used as a free graft. Although the cartilage survived in the other 4 animals from this group, the epithelization on the inner surface was found to be inadequate or absent in all specimens, and there was prominent leukocyte infiltration and granulation tissue surrounding the graft (Fig 1). In 6 of the 9 animals (67%) (4 of whom had total graft resorption) there was excessive bacterial growth, polymorphonuclear leucocyte infiltration, and abscess formation localized in the tracheal defect (Fig 2). These findings identify infections as the primary cause of cartilage loss, as opposed to shortcomings in sterile surgical technique or antibiotic prophylaxis. These results indicate that the use of cartilage as a graft is not a reliable method with regard to epithelization, infection, and resorption in reconstruction of the trachea, which is necessarily performed in a contaminated surgical field. In 2 of the 10 (20%) group 2 animals, the cartilage grafts resorbed after the first stage. In the other 8, grafts were found to be well covered with fibrovascular tissue. Evaluation of the tracheas 4 weeks after reconstruction revealed severe infection in 4 of 8 specimens (50%), 2 of which showed total graft resorption and all with inadequate or absent regrowth of epithelium. Although the epithelization was found to be moderate in 4 of 8 specimens in this group (Fig 3), it was not confluent throughout the lumen in any of the specimens. Infection was considered the major cause of failure in this group. Although the staging approach had a positive effect on epithelization, the risk of graft infection and resorption remained a serious problem.
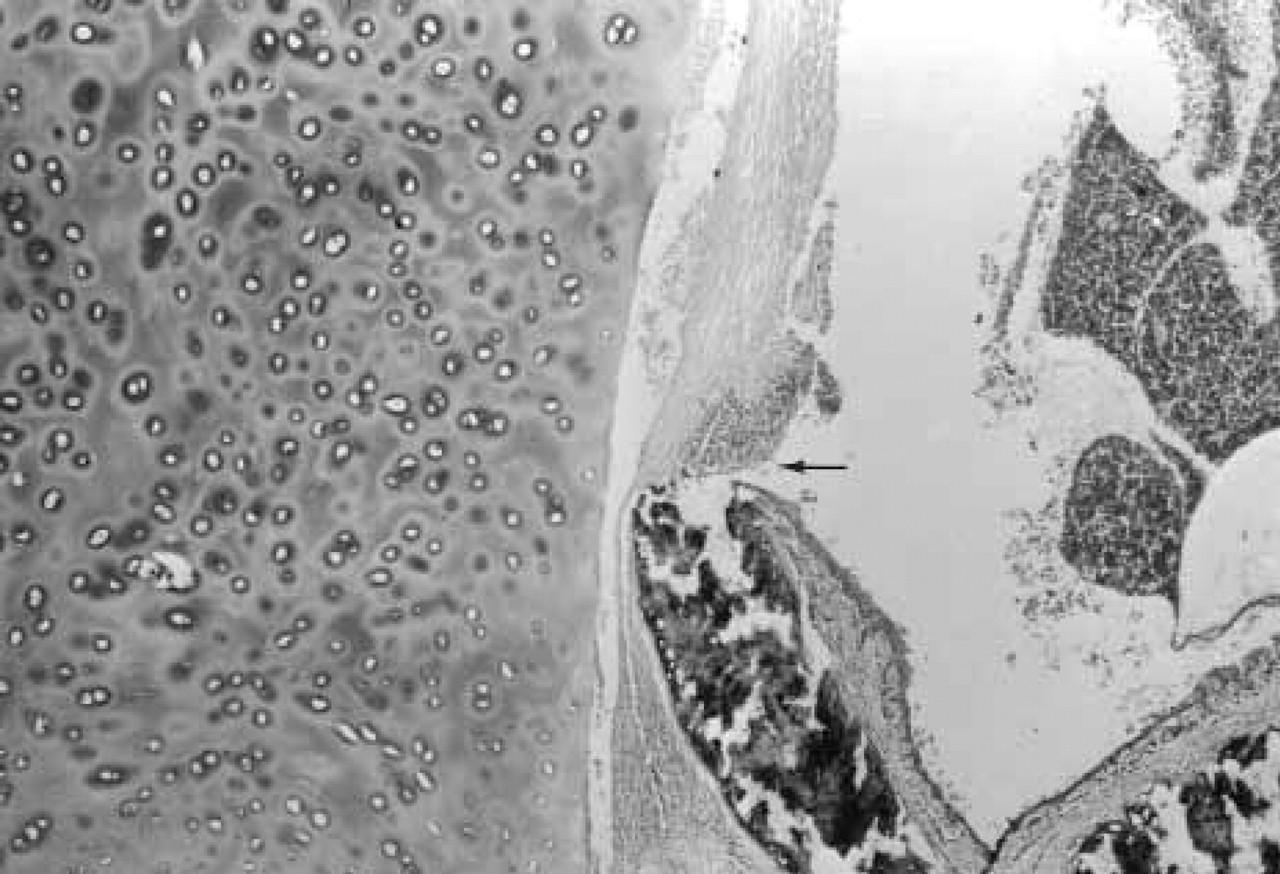
Excessive bacterial growth, polymorphonuclear leukocyte infiltration, and abscess formation with resorption of the graft (arrow) localized at the tracheal defect. (Hematoxylin-eosin; original magnification x40.)
The most favorable results were achieved in the surviving animals of group 3, where a free prefabricated neovascularized cartilage flap was used to reconstruct the trachea. Three of 15 animals, 1 with cartilage resorption at the first stage and 2 with thrombosed anastomoses, were excluded from the study. Four animals died during the microvascular flap operation. No cases of total cartilage loss were observed in any of the remaining 8 animals. Two of the 8 specimens (25%) showed moderate granulation tissue, bacterial growth, and abscess formation behind the flap, as well as partial cartilage resorption with inadequate epithelization on the luminal side. The other 6 specimens (75%) had good wound healing, had moderate or complete epithelization of the lumen, and showed no evidence of infection or granulation tissue formation (Fig 4). The statistical analysis of these data revealed that while there was no significant difference regarding the infection rates between group 3 and other 2 groups (χ2 = 0.114), the cartilage resorption rate was found to be significantly lower (χ2 = 0.032) and re-epithelization was found to be significantly better (χ2 = 0.014) in group 3. This result is consistent with findings in the literature of reported successful results with composite microvascular grafts in tracheal reconstruction. 9,14
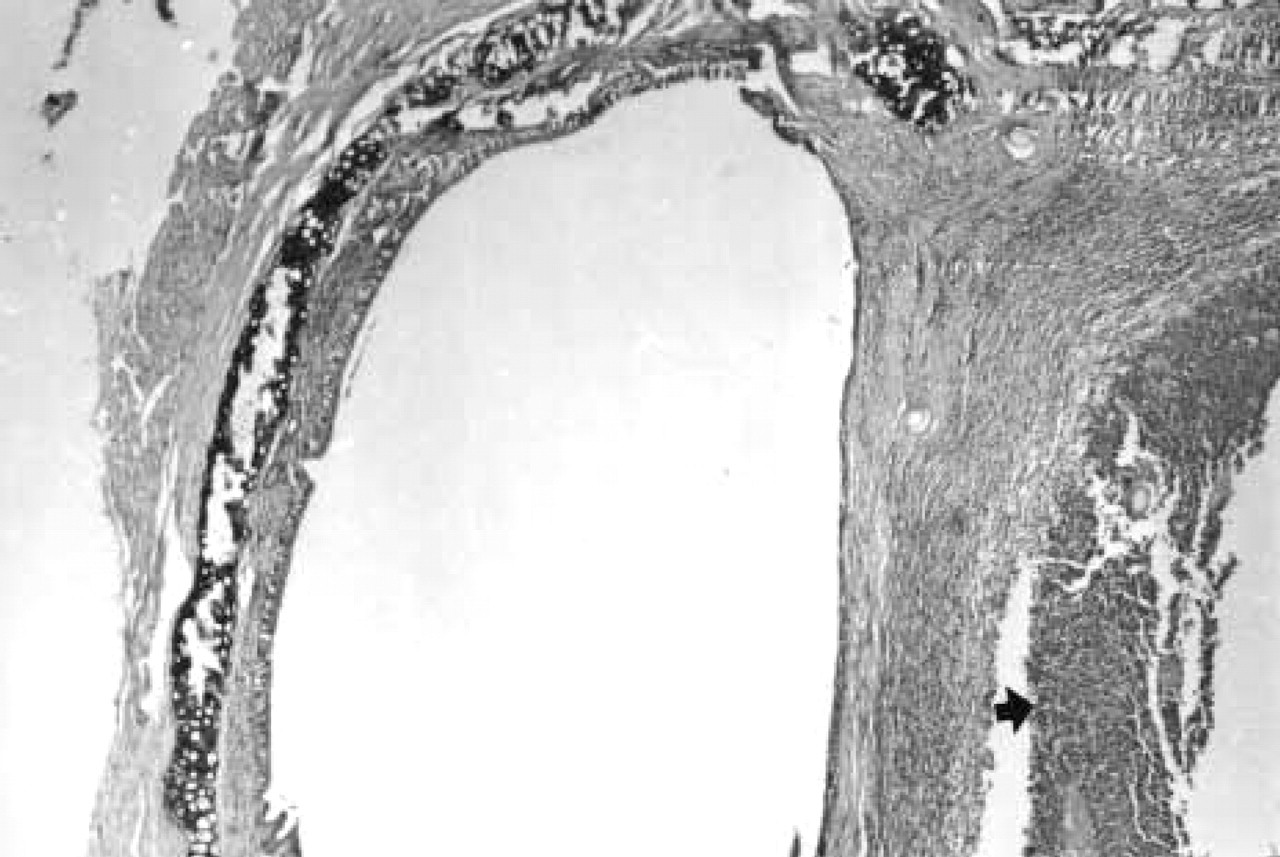
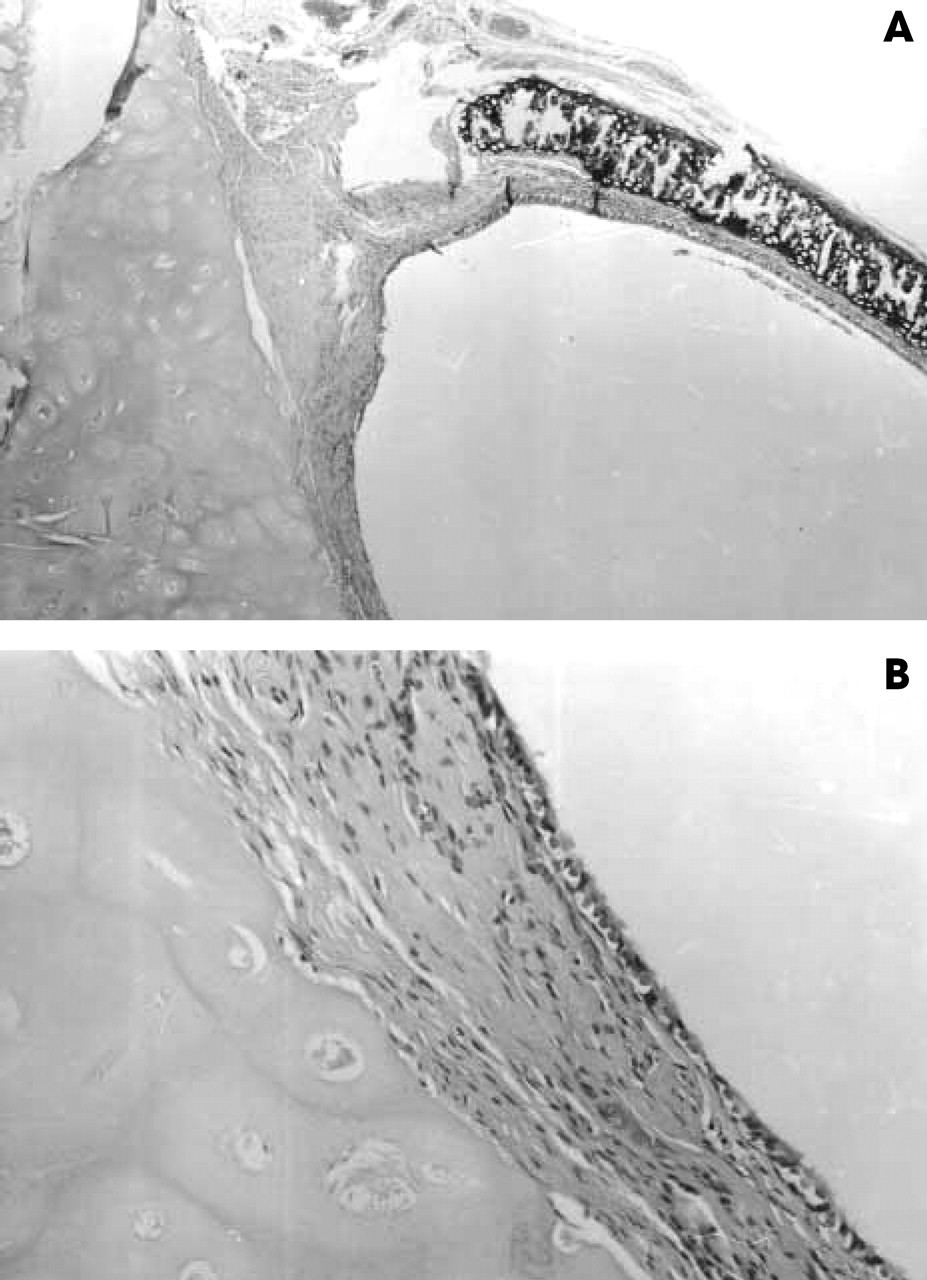
One of the specimens from group 2, where the cartilage was transferred to the neck after 3 weeks of prefabrication. Neovascularized cartilage graft covered the defect, but epithelization was not confluent throughout the lumen (arrow). (Hematoxylin-eosin; original magnification x40.)
In a contaminated area such as the trachea, infection of the reconstruction site is a major factor that can prevent wound healing, mostly through granulation tissue formation and inadequate epithelization. The advantages of vascularized tissue transfer, such as resistance to infection and necrosis, and high reliability in wound healing are well known in head and neck surgical reconstruction. Flap surgery also can be performed on irradiated or heavily scarred areas where grafting techniques have little chance for success. 9 Local, regional, and distant free flaps have been used in experimental tracheal reconstruction, and in almost all cases, such attempts have required the reconstructive technique to involve some skeletal element. 8-10,13,19 In free flap reconstruction of the trachea with prefabricated costal cartilage flap, the stability and support of the tissue are adequate for tracheal reconstruction, and there is no need for autogenous cartilage or bone tissue harvesting for supportive purposes, which is the major advantage of this technique. In group 3 no resorption was found in cartilage grafts of the 8 animals after the second stage. This means that once the cartilage graft is covered with connective tissue and does not undergo major resorption in the first stage, it is highly probable that it will preserve these characteristics when transferred as a vascular free flap. This provides an opportunity to monitor the graft before the final operation and to predict the outcome of the reconstruction.
Although this reconstruction method can be used in the clinical field with prefabrication of the allograft cartilage in well-known donor sites like the temporoparietal fascia or radial forearm, because of its drawbacks, like technical difficulties of microvascular surgery, considerable infection, inadequate epithelial regrowth (20% and 25% consecutively for vascular flap cases), and cartilage resorption (total of 12% after the first implantation stage), it can be considered an alternative when more reliable or easy to perform treatment modalities fail. Also the use of allogenous cartilage should be among the armamentarium of a surgeon dealing with tracheal reconstruction when it is impossible to obtain enough autogenous material or it is important to avoid morbidity during the harvesting procedure.
Good wound healing between cartilage flap and native trachea with complete epithelization of the lumen, without any evidence of infection or granulation tissue formation in one of the group 3 specimens.
Another disadvantage of use of solvent-dehydrated human cartilage is its propensity for infection during the rehydration process, which requires about 12 hours just before use. This could have been the reason for the high infection rate seen in our study. The manufacturer has eliminated this negative aspect with the recent introduction of an already rehydrated sterile product.
CONCLUSION
Reconstruction of large tracheal defects remains a problem in head and neck surgery. Although various techniques are presented in the literature, the most encouraging results have been achieved with autogenous tissue transfers used as composite microvascular flaps. In tracheal reconstruction, the use of dehydrated human costal cartilage, which is a nonautogenous graft, is an alternative method that eliminates the cartilage or bone donor-site deformity of other reconstruction techniques. However, because of technical difficulties, considerably high infection rates, and luminal epithelization problems, which were encountered even with the most favorable prefabricated neovascularized free flap form, this method is not considered a first-line treatment option for tracheal reconstructive surgery.