Abstract

DISCUSSION
Facial nerve dehiscence is not an uncommon occurrence. Baxter 1 studied 535 temporal bones and found the incidence of facial nerve dehiscence to be 55%, with most located in the tympanic segment (91%). Fewer than 9% were located in the mastoid segment, and dehiscences rarely involve the labyrinthine segment or the area of the geniculate ganglion. Of dehiscent tympanic segment facial nerves, 83% were adjacent to the oval window, with 26% of facial nerves protruding from the canal. Embryologically, the facial canal is derived from 2 structures: the primordial otic capsule and Reichert's cartilage (second branchial arch). 2 Although ossification of these structures begins during gestation and is completed by the end of the first year of life, incomplete ossification results in exposure of part, or all, of the facial nerve.
CHL, as a result of marked protrusion of the facial nerve and contact with the incudostapedial joint and stapes superstructure, has been documented by many surgeons. 3 Dehiscence of the tympanic segment of the facial nerve is neither frequently considered nor frequently found as a cause of CHL. However, aside from this patient's pars flaccida retraction pocket, the remainder of her history, physical examination, audiometry, and intraoperative finding were typical for a patient with a dehiscence of the tympanic segment of the facial nerve. Heightened preoperative and intraoperative vigilance should prevent any iatrogenic facial nerve injuries to an exposed facial nerve.
Footnotes
Appendix
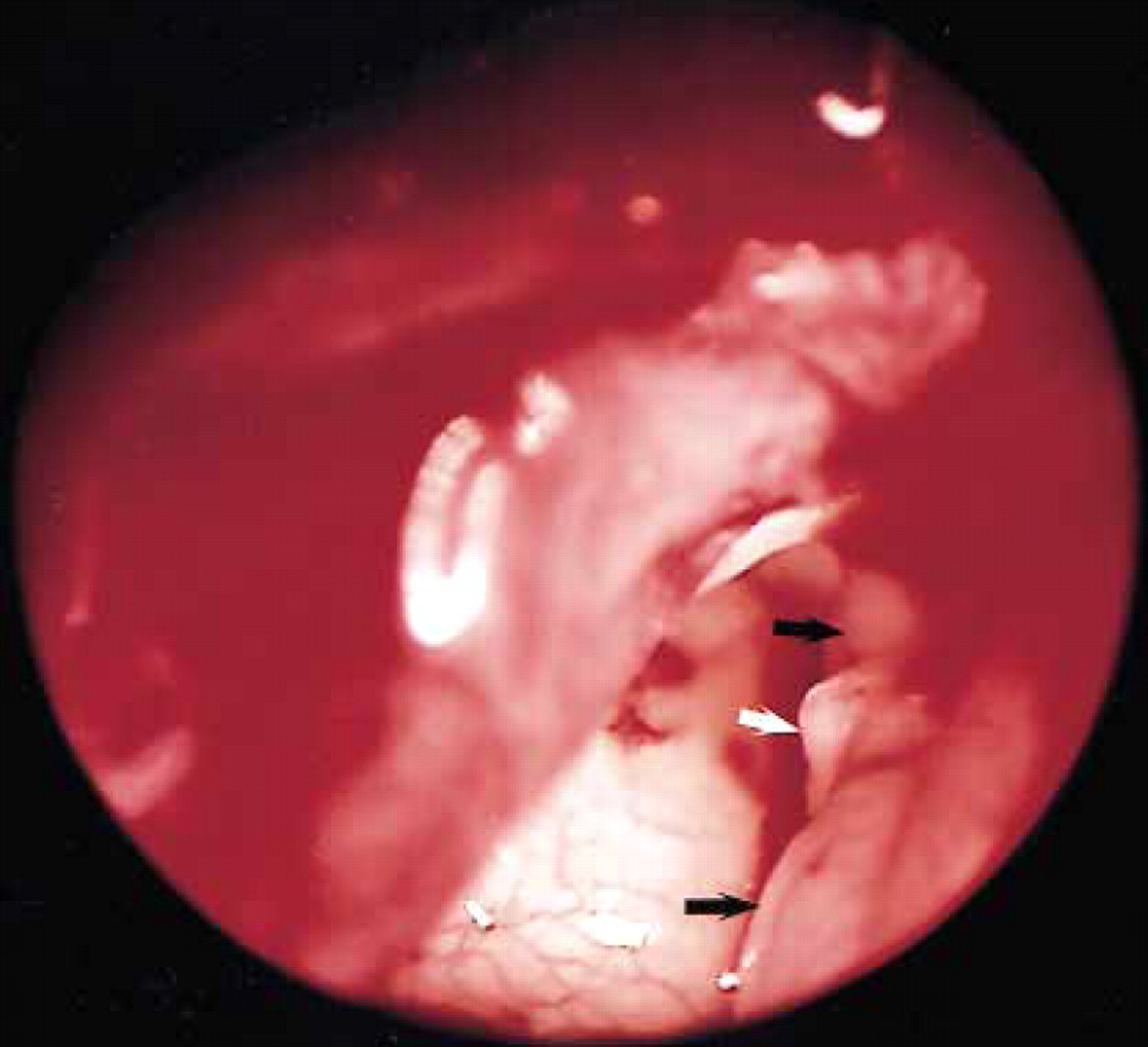
Transcanal view with a 4-mm 0° degree rigid oto-scope showing a completely dehiscent tympanic seg-ment of the facial nerve (black arrows) crossing under-neath the lenticular process of the incus and abutting the stapes superstructure (white arrow).