
Abstract
ABSTRACT
OBJECTIVES: Bone-screw mandible fixation (BSMF) is evaluated as an alternative to intraoperative arch-bar maxillomandibular fixation before plating of mandibular fractures. BSMF is achieved by wire ligation of opposing bone-screws placed in the maxilla and mandible.
METHODS: A retrospective evaluation of 23 patients with 40 mandibular fractures who underwent man-dibular fracture repairs. BSMF was used instead of arch bars to ensure proper dental occlusion. All fractures were then plated, after which BSMF was removed before termination of anesthesia.
RESULTS: Normal occlusion was observed in 21 patients (91.3%), Class II malocclusion was noted in 1 patient (4.3%), and 1 patient was edentulous. No complications related to the use of BSMF were observed.
CONCLUSION: BSMF can serve as a viable alternative to arch-bar maxillomandibular fixation for obtaining temporary intraoperative occlusion. BSMF produces acceptable malocclusion rates and offers the advantages of decreased intraoperative time, lower risk for percutaneous and mucosal wire punctures, and ease of use.
Decreased risk of percutaneous wire and mucosal punctures and disease transmission risk to surgeon and patient alike.
1
,
6
–
9
Significant intraoperative savings in time and cost.
1
,
7
,
8
In our experience, ICBSF can be placed and removed in less than 15 minutes, whereas arch placement can take 45 to 100 minutes for placement and removal. Ease of application with acceptable proper occlusion attainment.
1
,
6
In considering these advantages, a new application of ICBSF was evaluated in obtaining proper intraoperative dental occlusion, before repair of fractures with mini-plates. In this study, ICBSF is used as a temporary intra-operative method of obtaining occlusion and not for closed reduction of mandibular fractures as in previous studies. 1 , 2 , 6 - 8 To our knowledge, no other studies have evaluated this method in obtaining temporary intraoperative occlusion. We call the reversible and temporary intraoperative use of the ICBSF technique, bone-screw mandible fixation (BSMF). We present our experience of using BSMF instead of arch bars, in obtaining temporary intraoperative dental occlusion before plating.
METHODS AND MATERIAL
A retrospective chart review of 23 patients with mandibular fractures treated at the Mount Sinai Medical Center of Chicago was undertaken. The same surgeon (A. A.) had treated all patients with the same technique. All patients underwent mandibular fracture repairs where BSMF was used to achieve proper occlusion before plating. BSMF involved the application of 4 Leibinger titanium intermaxillary fixation self-tapping screws (2.0 × 14 mm; Leibinger, Freiburg, FRG); 2 were placed above the tooth roots in the region of the lateral pyriform aperture of the maxilla, and 2 below the tooth roots medial to the mental foramen of the mandible. A stab incision made in the mucosa allowed for placement of the self-tapping bone-screws. These screws were then ligated together with 24-gauge ligature wire to achieve proper dental occlusion (Fig 1). The fractures were repaired with 3-dimensional titanium miniplates (Leibinger) of appropriate size as described by Farmand.10 With the fracture(s) plated, wire ligature and bone screws were removed atraumatically in the operating room before termination of anesthesia.
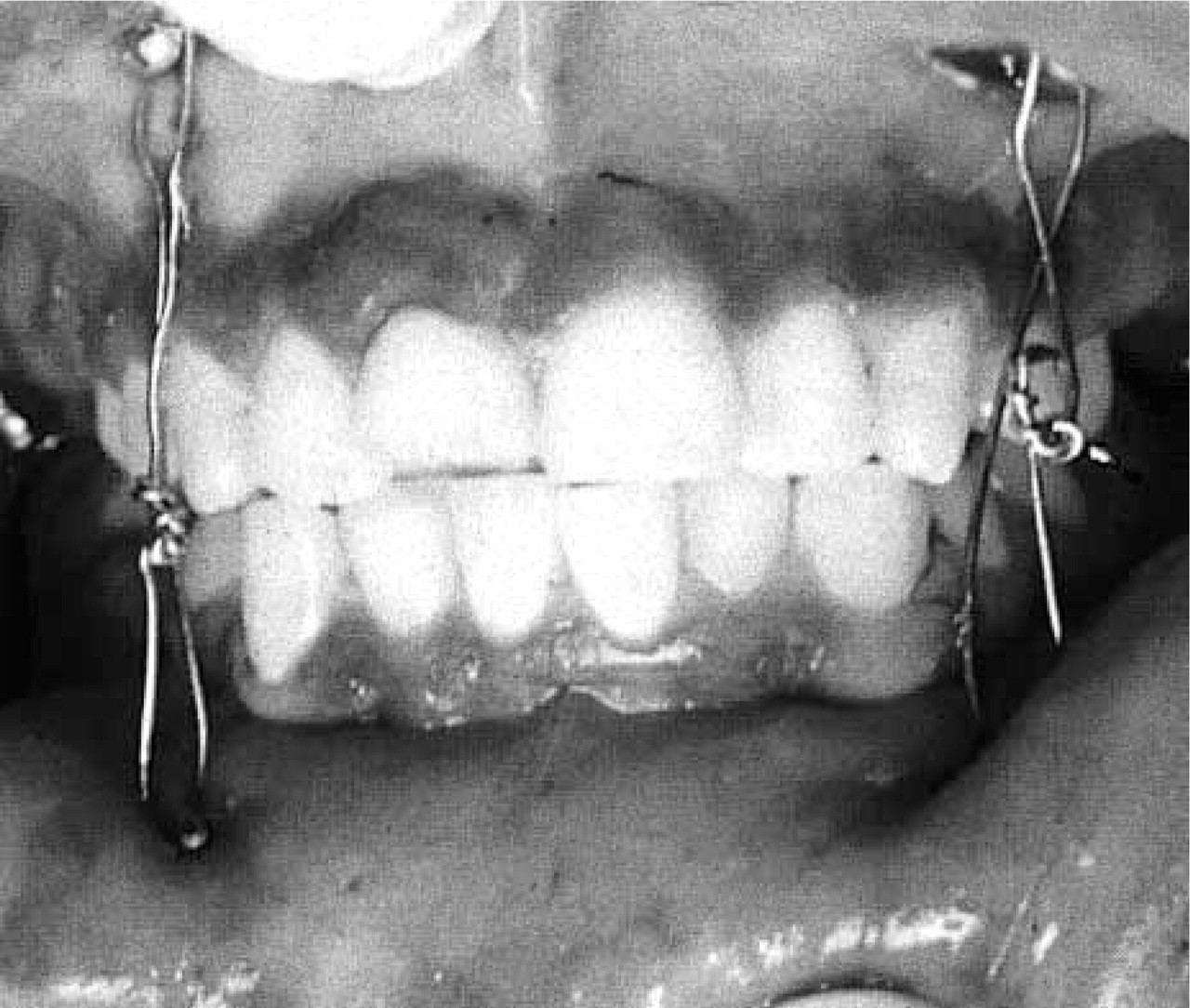
Bone-screw mandible fixation (BSMF).
RESULTS
Twenty-three patients had sufficiently complete charts and were entered into the study. Twenty (87.0%) patients were male, and 3 (13.0%) were female. Ages ranged from 17 to 70 years of age, with an average age of 32 and median age of 25 (Fig 2). Mechanisms of injury included assault in 8 (34.8%) patients, gun shot wounds in 6 (2.1%) patients, blunt injury in 6 (26.1%) patients, accidental falls in 2 (8.7%) patients, and motor vehicle accident in 1 (4.4%) patient (Fig 3). Seventeen (73.9%) patients had no fractures at other sites, 4 (17.4%) patients had extremity fractures, 1 (4.4%) patient had a zygomatic fracture, and 1 (4.4%) patient had a skull fracture.
Mandibular sites fractured numbered 40 in the 23 patients. Multiple mandibular fractures were observed in 14 (60.9%) patients; the remaining 9 (39.1%) patients had a single mandibular fracture site. Eleven (27.5%) patients had bilateral fracture sites. The fracture sites repaired occurred in all parts of the mandible with the parasymphysis (32.5%), body (27.5%), and ramus (17.5%) of the mandible accounting for most of the fractures (Fig 4).
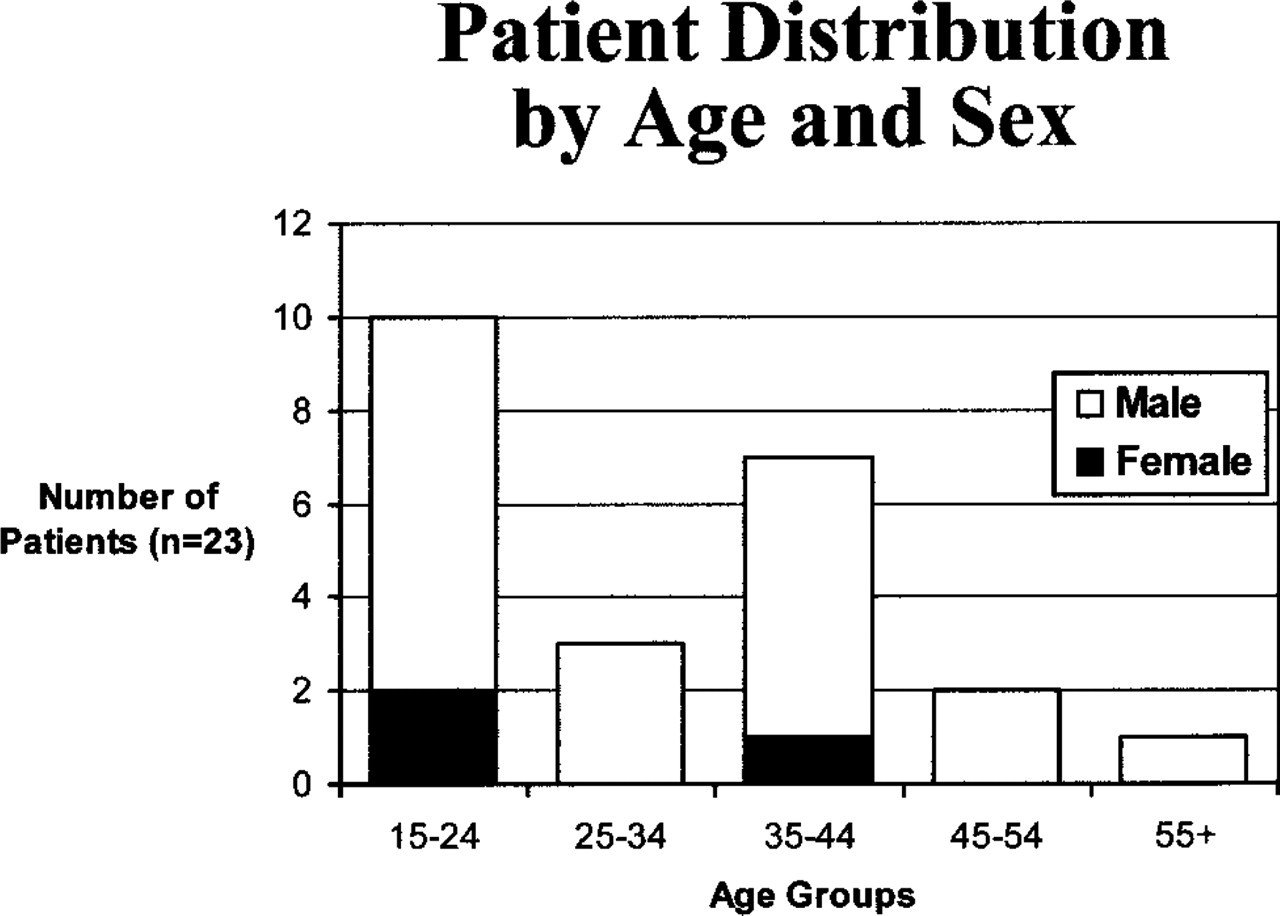
Patient distribution by age and sex.
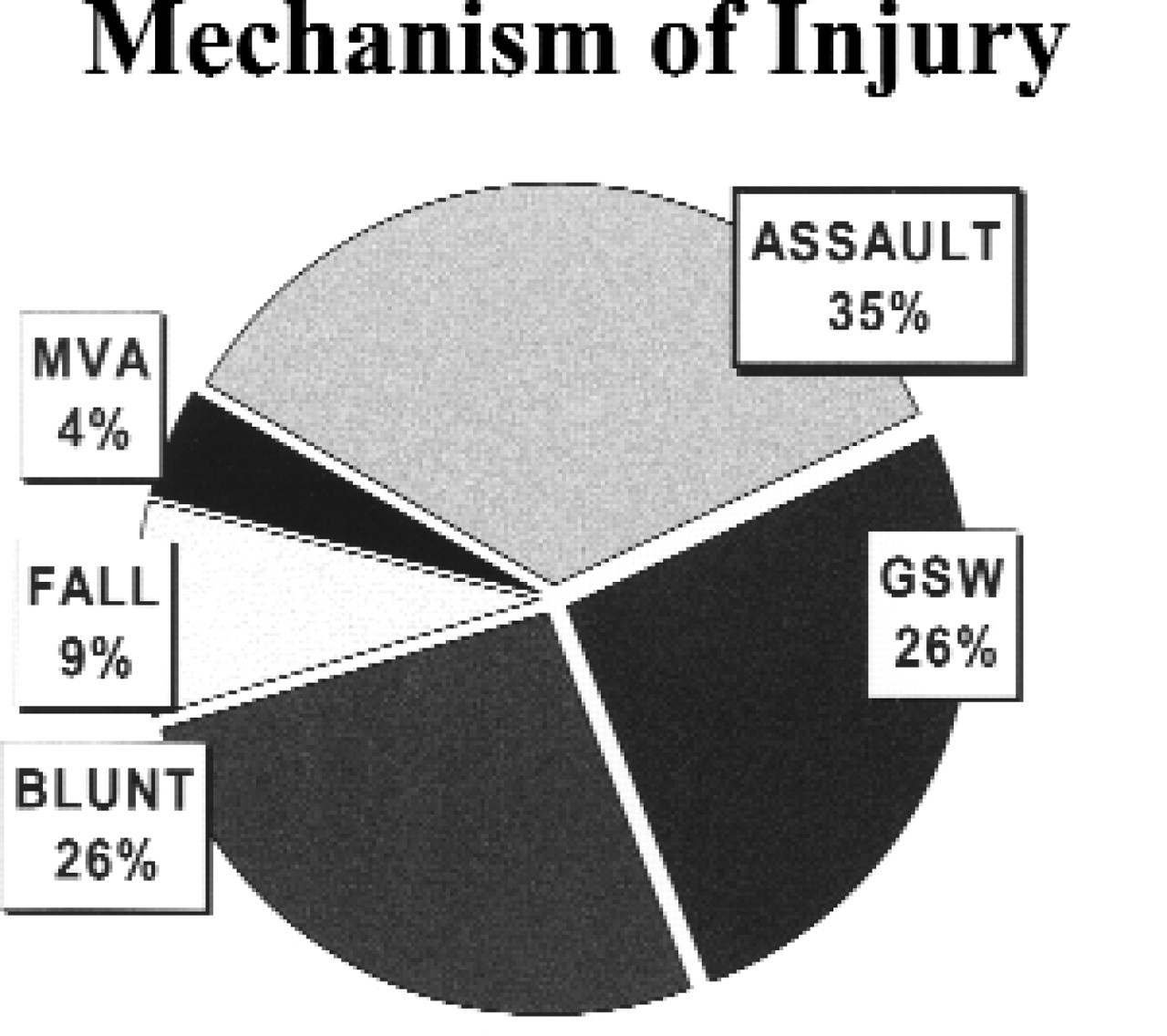
Mechanisms of injury (MVA, motor vehicle accident; GSW, gun shot wound).
Time to surgery ranged from 8 hours to 14 days, with an average time of approximately 3 days and median time to surgery of 2 days. Only 1 patient required tooth extraction as a result of a GSW injury to alveolar bone.
We observed 21 (91.3%) patients with normal occlusion, 1 (4.4%) patient with Class II malocclusion, and 1 (4.4%) edentulous patient (Fig 5). Nineteen (82.6%) patients were placed on clear or liquid diet postoperatively, and 4 (17.4%) patients were placed on a soft diet. Deficits in lower lip sensation to pinprick were observed in 5 (21.7%) patients; the remaining 18 (78.3%) patients had normal bilateral lower lip sensation. When eliminating those patients with preoperative lower lip numbness, 3 (14.3%) patients had deficits in lower lip sensation, and 18 patients (85.7%) had normal lip sensation.
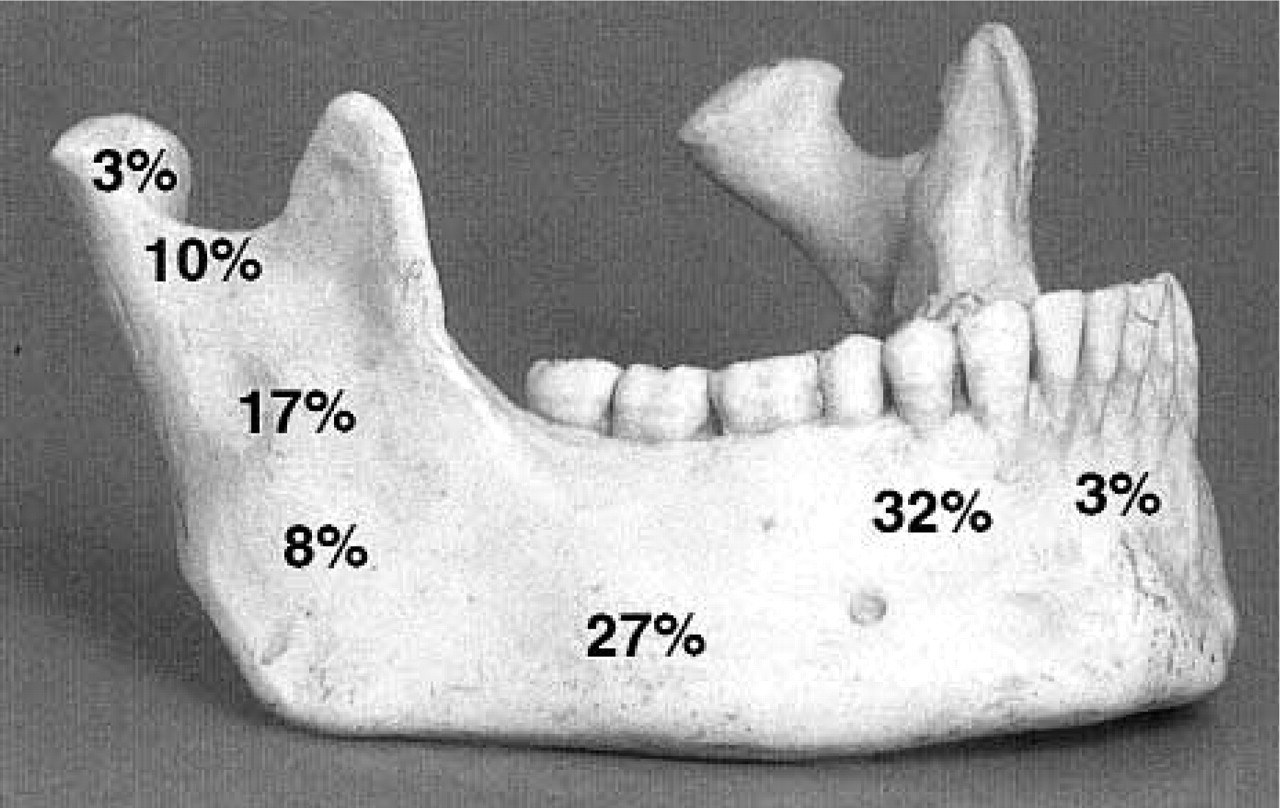
Distribution of mandibular fracture sites as a percentage of the total number (n = 40).
In all the cases reviewed, there was no incidence of percutaneous puncture injury to the surgical staff and no record of blood-borne disease transmission. No incidence of postoperative bleeding or infection was noted in relation to the cortical bone screw placement and removal. Seven (30.4%) patients were lost to follow-up. In the remaining 16 (69.6%) patients, follow-up dates ranged from 28 to 57 days postoperatively, with an average and a median follow-up at day 40. All patients at this follow-up encounter were observed to be tolerating a regular diet, without any history of oral infections, and no subjective complaints relating to the bone-screw placement sites. All the bone-screw sites were well healed, with mucosal tissue obscuring the actual screw placement sites.
DISCUSSION
The main goals in successfully treating mandibular fractures include: reduction of the fracture, stabilization of the fracture and the jaw, and achievement of proper postreduction dental occlusion. In the process of fully satisfying these criteria, it is also advantageous to use techniques that reduce the following: the risk of percutaneous transmission of blood-borne diseases, operating room and general anesthesia times, and hospital costs.
Arch bars, although used commonly, take a relatively long time to apply and remove, and place the surgeon in high risk for percutaneous wire punctures. BSMF can be placed in position by the ligation of only 2 wires. As such, its placement and removal involves a greatly reduced risk for percutaneous wire punctures. It is also easier to use and requires less time for its placement and removal compared with arch bars. BSMF placement and removal times were recorded in several cases and were found to be around 15 minutes. In our experience, arch-bar MMF placement and removal takes at least 45 to 60 minutes, and longer in some cases. Most importantly, our use of BSMF produced acceptable postreduction dental occlusion results with minimal observed complications.
Postoperative occlusion status.
As the data suggest, we used BSMF in patients with a variety of different mandibular fracture sites. We did not use it in patients with extensive comminuted mandibular fractures or multiple anterior mandibular arch fractures with floating segments.
The main question in this study was whether BSMF with its described advantages would yield acceptable (anatomically correct) postreduction dental occlusion results. Normal occlusion was observed in 91.3% of our patients. We used Angle's classification of occlusion status based on: position of the mesiobuccal cusp of the first maxillary molar to the buccal groove of the first mandibular molar, and the relationship of the maxillary and mandibular incisors. Subjective evaluation of dental wear facets did not change any patient's occlusion classification. None of the patients had a severe degree of malocclusion. One (4.4%) patient had Class II maloc-clusional status with no subjective complaints relating to mastication or dental discomfort. This patient had suffered bilateral mandibular fractures at the level of the left parasymphysis and right condyle. The sustained injuries were resulted from violent personal assault. In other patients with bilateral and/or multiple fracture sites, normal dental occlusion was achieved. The other patient (4.4%) was edentulous and without his dentures at the follow-up visit, rendering occlusion evaluation difficult. The dental occlusion status prior to injury was unknown in these patients.
In other mandibular trauma studies, observed maloc-clusion rates ranged from 3% to 7%. 6 , 11 – 13 In the treatment of mandibular fractures in 75 patients with plating alone (with intraoperative MMF), El-Degwi and Mathog et al 11 observed a 5.3% malocclusion rate. Edwards and David 13 in a comparative study of 217 patients treated with different plating systems found 13 (5.3 %) of all 217 patients treated required reoperation as a result of the malocclusion. Although our observed malocclusion rate of 4.4% is well within the range of malocclusion rates published in other studies, a larger number of patients may be necessary to attain a more accurate figure.
We observed no complications attributable to the placement or removal of the bone-screws. Excluding patients with preoperative lower lip numbness, we observed 3 (14.3%) patients with lower lip anesthesia. We do not believe BSMF was responsible for the lower lip anesthesia, as the screw placement sites were medial to the mental foramen in the mandible. In addition, during the placement of the bone-screws sufficient irrigation was used as to minimize thermal damage to adjacent nerves. Gordon et al 6 observed no lip anesthesia in 29 patients with mandibular fractures treated solely with intraoral cortical bone-screw fixation (ICBSF) placement for 6 weeks. We used the same screw placement sites as described by Gordon et al.6 In other published studies, 1 , 2 , 7 where the same bone-screw placement sites were used for ICBSF, no reports of lower lip anesthesia were made. In conjecturing an explanation for the observed lower lip anesthesia, several may be plausible: iatrogenic injury from plating the fractures, nerve injury from bone segment movement during fracture reduction, previously unrecognized traumatic nerve injury, or stretching nerve injury from lip retraction.
CONCLUSION
We present BSMF as a viable alternative to arch-bar MMF for obtaining temporary intraoperative occlusion. BSMF produces acceptable malocclusion rates while offering the advantages of decreased intraoperative time, lower risk for percutaneous and mucosal wire punctures, and ease of use. BSMF can be especially useful in settings where issues of blood-borne disease transmission and operative time management and cost are of greater concern. BSMF is contraindicated in patients with extensive comminuted mandibular fractures or multiple anterior mandibular arch fractures with floating segments. Prospective randomized studies in the future can further elucidate the use and efficacy of this method, as well as more specific guidelines for its use.