
Abstract

Posterior epistaxis that originates from traumatic pseudoaneurysm of the intracavernous portion of the internal carotid artery (ICA) is a life-threatening clinical situation. An effective modality of treatment for these potentially life-threatening lesions is endovascular embolization utilizing detachable coil and/or detachable balloon occlusion of ICA. 1
There is a debate as to the safety of endovascular occlusion of an aneurysmal sac with preservation of the parent artery. Crow et al 2 suggested this technique may be hazardous in the treatment of psuedoaneurysm due to the fragile nature of the wall of the aneurysm that may not support the embolic device. However, some authors 3,4 have proposed a new device and technique for intrasaccular aneurysm occlusion with preservation of parent artery flow.
This report describes the endovascular obliteration of a traumatic pseudoaneurysm of the cavernous ICA with Guglielmi Electrolytically Detachable Coils (GDC) (Target Therapeutics Inc, Fremont, CA) in a 54-year-old man at our hospital. At first, the pseudoaneurysm was completely obliterated with GDC coils. This obstructed pseudoaneurysm was recanalized on postembolization day 15, so the total occlusion of ICA was performed utilizing the detachable coil and balloon.
CASE REPORT
A 54-year-old man with a head trauma from a fall 5 months earlier presented with repeated episodes of massive epistaxis. He was transferred from another hospital for management of vigorous epistaxis, which had developed 30 minutes before. The sudden bleeding resulted in loss of consciousness and hypotension with a systolic blood pressure of 60 mm Hg. Fluid resuscitation was achieved, and nasal packing temporarily stopped the bleeding. He had been treated at another hospital for a basal skull and femur fracture related to his fall. Following this injury, right-sided blindness developed with no light reflex. A brain CT scan revealed a fracture line in the medial wall of the right orbital apex and a mass shadow in the right sphenoid sinus cavity with bone erosion. A pseudoaneurysm was connected to the right side of the sphenoid sinus wall. The diagnosis was confirmed by carotid angiography, which showed an 8 × 11 mm contrast-filled aneurysm in the right intracavernous portion of ICA.
After informed consent had been obtained, GDC coils were introduced into the aneurysmal sac using a transfemoral approach. The detachable component of coil was 40 cm in length and made of platinum. Five GDC coils were successfully introduced into the pseudoaneurysmal sac of ICA. The pseudoaneurysm was successfully obliterated while preserving the patency of ICA (Fig 1A ).
A repeat angiography after 15 days showed a recanalizing pseudoaneurysmal sac and the psuedoaneurysmal sac was enlarged (Fig 1B ). The GDC coils within the aneurysmal sac were displaced distally. The pseudoaneurysm was enlarged at the base portion of the sac. After balloon occlusion test, endovascular occlusion of the entire right side lumen of ICA was performed with 1 coil distal to and 1 detachable balloon proximal to the pseudoaneurysm. Follow-up at 8 months demonstrated no symptoms of epistaxis or any neurologic deficit.
DISCUSSION
Traumatic pseudoaneurysm can be treated in different ways. Detachable balloon occlusion of the ICA above and below the aneurysm can be easily accomplished and carries a relatively low complication rate. 1 However, preocclusion determination of cerebrovascular sufficiency should be tested by the inflation of a balloon for at least 5 minutes before permanent placement. The incidence of ischemic complications with carotid artery ligation is reported to be as high as 41%, if an ICA-ECA bypass is not performed first. 5
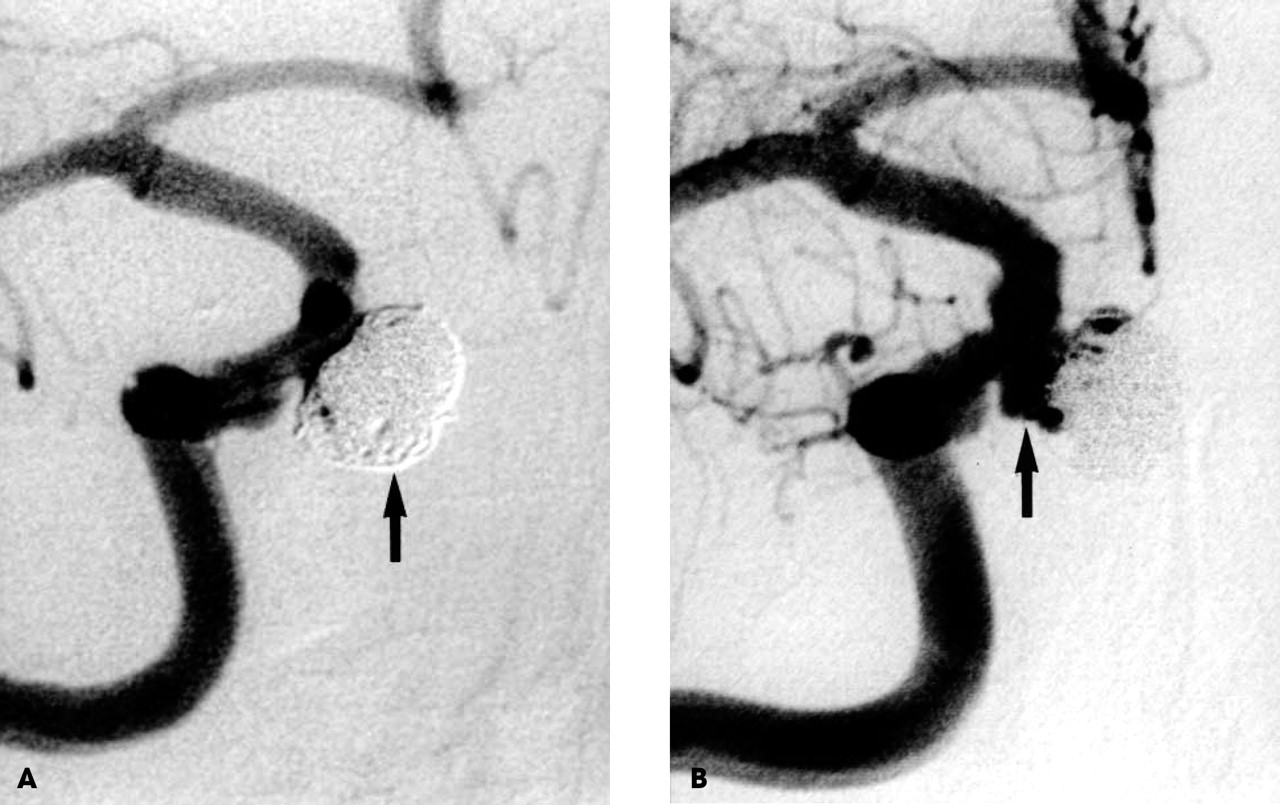
A, Arteriogram after embolization of the aneurysm cavity with 5 GDC coils (arrow), the 8 × 11 mm aneurysm appears occluded and the internal carotid artery remains patent. B, Arteriogram 15 days after intrasaccular GDC coil embolization demonstrates revascularized aneurysm (arrow) and laterally displaced GDC coils.
The intrasaccular aneurysmal detachable balloon technique has disadvantages as the internal shape of the aneurysm may be different from the shape of the detachable balloon used. Complete obliteration of the aneurysm may be impossible, and improper size selection of balloon compared with the aneurysm may lead to disastrous results.
A newly developed GDC coil consists of a very soft detachable platinum coil and delivery wire. 3,4 Reports 3,4 are that it can permit intracranial anuerysm obliteration while maintaining patency of the parent artery. If the lumen of the pseudoaneurysm can be occluded while maintaining patency of the internal carotid artery, the balloon occlusion test can be abandoned.
In this case, angiography 15 days after embolization using GDC coils demonstrated that the pseudoaneurysm was enlarged and the embolization materials were displaced laterally. As a result of our experience, the intrasaccular obliteration of an ICA pseudoaneurysm using detachable coils is not recommended. Complete ICA obliteration may be a safer and more reliable treatment for traumatic pseudoaneurysm.