
Abstract
INTRODUCTION: Adults with a common cold often have paranasal sinus effusions detected by computed tomographic (CT) scans. There are no comparable data for children. The purpose of this study was to document the sinus CT findings in children with short-duration purulent rhinorrhea.
DESIGN: Thirty Children, 3 to 12 years of age (median age, 7 years), with purulent rhinorrhea for a mean duration of 5 days (and always less than 9 days) were enrolled in the study. The children were otherwise well. Institutional Review Board (IRB)-approval was obtained before enrollment of the first patient. Informed written consent was obtained from each child's parent. CT imaging of the maxillary and ethmoid sinuses was obtained on the day of the initial visit (occasionally, the following day). Follow-up CT scans were obtained from cooperative children/parents, 3 to 4 weeks later.
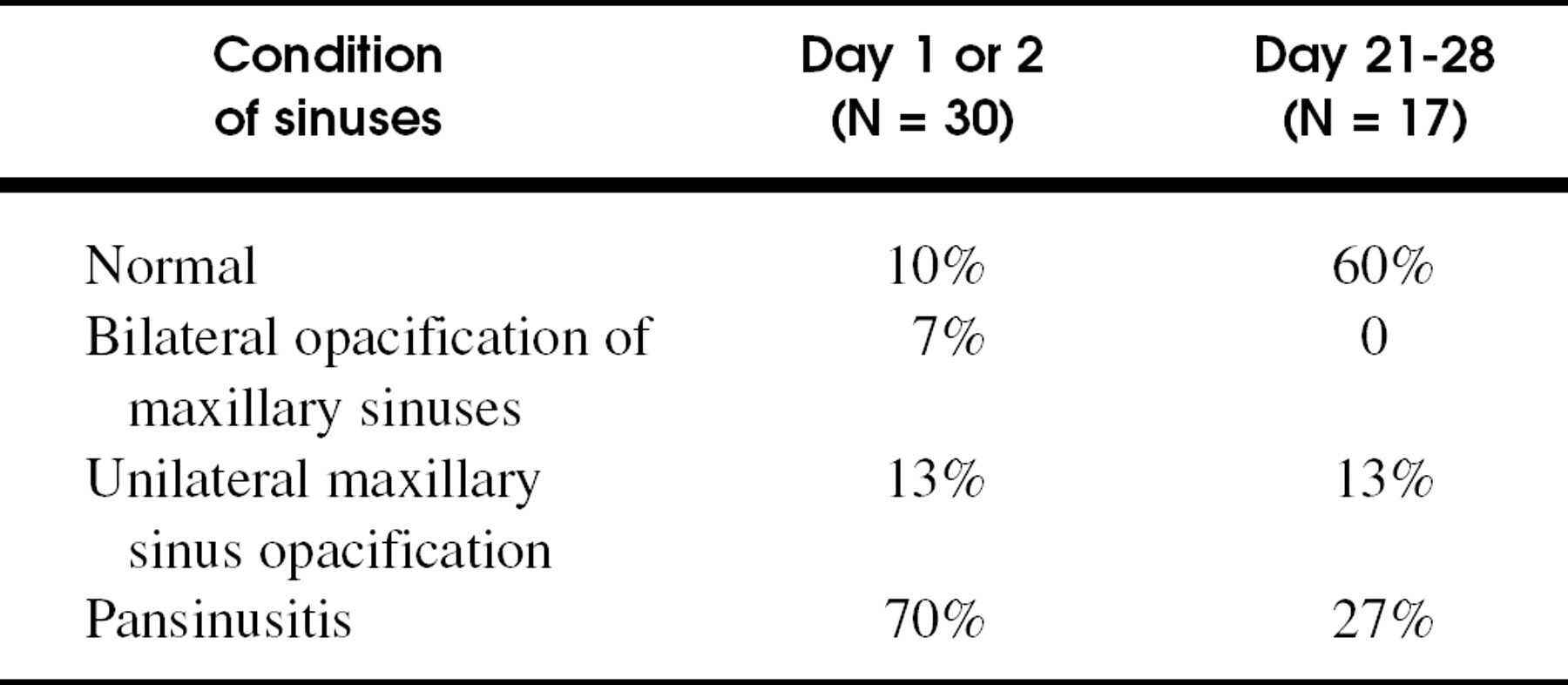
RESULTS: Opacification or an air/fluid level in the maxillary sinuses was seen in 27 (90%) of 30 study children at study entry. Ethmoid sinuses were not opacified without opacification of a maxillary sinus. Three weeks later, 24 of 27 study children, who had positive CT scans on study entry, improved clinically. Of 17 follow-up CT scans, 10 (58%) normalized, 4 had improvement of bilateral disease, and 3 improved with unilateral disease. None appeared worse than baseline.
CONCLUSIONS: Pansinus opacification (ethmoid and maxillary sinuses), on CT scans in children with short-duration purulent nasal drainage was seen in 70% of children. An additional 20% had isolated maxillary sinus effusions (10% had no effusion). Three-week follow-up CT scans on 17 children were normal in 60% and improved (partial clearance) in 40%. In this patient population, the decision to treat with antibiotics should be made on clinical grounds alone.
Purulent rhinorrhea of short duration is often part of the natural history of the common cold, and antibiotics are considered as injudicious treatment. In 1997, the American Academy of Pediatrics and the Centers for Disease Control and Prevention (CDC) published joint good clinical practice guidelines for the diagnosis and management of uncomplicated acute sinusitis. 1 According to these guidelines, the diagnostic criteria for acute noncomplicated sinusitis are rhinorrhea, of any quality, for at least 10 days' duration, often accompanied by frequent coughing, malaise, and fever. The bacteriology and maxillary sinus imaging of rhinosinusitis has been studied extensively. 2-11
Before distribution of the CDC/AAP Guidelines, antibiotics were prescribed for as many as 65% of children who presented to their family physician or general pediatrician with purulent nasal discharge of a few days' duration. 2 Antibiotics were and are prescribed because of parental request or pressure or because of a physician's diagnosis of complicated upper respiratory infection (URI) or acute sinusitis. 2,3 By the fifth day of a common cold caused by rhinovirus, CT scans show maxillary sinus changes in 80% of adults. These CT findings improve within 2 weeks and do not require antibiotic therapy. 4 There are no comparable studies in American children.
In the present study, we obtained thin-section, direct coronal plane CTs of the maxillary and ethmoid sinuses and ostiomeatal complexes in a group of children who presented with purulent nasal discharge of short duration. Radiologists were told only that the children were part of a clinical study of purulent rhinorrhea. One of the purposes of this study was to learn if CT scans from children with purulent rhinorrhea of short duration showed similar changes as the adult population. This study was undertaken before the publication of the CDC-AAP Good Clinical Practice Guidelines for the diagnosis and management of rhinosinusitis. 1
METHODS
Patients
Children between 3 and 12 years (median age, 7 years), who presented to their pediatrician with purulent nasal discharge were eligible for the study. Written informed consent was obtained from the accompanying parent. One very cooperative 2 ½-year-old child was included as a 3-year-old. The children were otherwise healthy. None of the study group had pneumatic otoscopic signs of acute otitis media. Four children (13%) had purulent rhinorrhea for more than 48 hours but less than 3 full days (mean duration of purulent rhinorrhea, 60 hours). The others had at least 72 hours of copious purulent rhinorrhea before study entry. Anterior rhinoscopic examination in all cases revealed copious mucopurulent secretions in the inferior and/or middle meatus. Exclusion criteria were (1) antibiotic use within the previous 72 hours; (2) concomitant acute otitis media; (3) serious, hyperacute sinusitis (ie, periorbital eyelid swelling or fever greater than 39.9°C, at the time of entry); (4) a positive rapid test for group A streptococcal antigen; (5) physical signs of lobar consolidation or of alveolar infection (rales); (6) symptoms suggestive of chronic sinusitis (eg, chronic purulent rhinorrhea, chronic stuffy nose, and halitosis); (7) administration of oral or topical decongestant during the study; and (8) major craniofacial syndromes.
A solution of 20 cc of normal saline was flushed into the more superior nostril of the supine patient with the ear up. The purulent effluent was collected into a plastic sealable (Zip-Lock) bag held under the dependent nostril. The purpose of the nasal lavage was diagnostic (determination of the quantity and character of nasal drainage) and therapeutic to clear out the nose and nasopharynx of thick secretions. At least 5 cc of thick, opaque, green/yellow nasal secretion and at least 10 neutrophils (and fewer epithelial cells) per high-powered microscopic field were required for study entry. Microscopic examination was performed immediately on site.
A rapid streptococcal antigen test was performed on a pharyngeal swab, and those children with positive results were excluded from study entry. Within 4 hours (in 2 cases, the next day), high-speed, thin-section, coronal view computed tomographic (CT) scans were obtained without prior sedation of the child. Approximately 50% of the study group were treated with cefuroxime axetil after obtaining CT scan results. Selection to placebo group or cefuroxime group was made on a computer-generated table of random numbers. A reevaluation visit was scheduled between day 3 or 4 of the study. If the child developed hyperacute sinusitis with facial or eyelid edema and pain, or he or she did not improve by the 8th day after onset, antibiotics were prescribed. All children who failed to have either of the criteria were given a prescription for a 10-day course of antibiotics and the parents instructed to use saline nose drops, oxymetrazoone (0.05%) for 3 days, and nasal suction. A study nurse telephoned all failures within 24 and 48 hours to assess the status of the child and the need for in-office evaluation. Telephone reminders were made at days 11 through 14 and also at the 3-week mark for all study patients to assess clinical status and to remind parents of children whose initial CT scan had been positive to bring their child in for a follow-up CT scan. The Western Institutional Review Board (WIRB, Olympia, WA), a research IRB with expedited evaluation approved this protocol. We have used WIRB on many previous clinical studies of antibiotics. We did not seek permission from our local hospital IRB. All specimens were objectively verified to be yellow, green, or a mixture of the 2 colors by comparing the color of the purulent material in the plastic bag with gradations of colors from a commercially obtained sheet of yellow or green paint chips (Benjamin Moore Company, Montvale, NJ).
Sinus CT results on study entry and at follow-up
CT Image
Five-slice, thin-section, noncontrast, direct coronal CT imaging of the nasal and paranasal sinuses was performed, usually within 4 hours and always within 24 hours of the initial visit. Radiologists were located in a distant address and were blinded to the clinical results other than that the children were part of a study of purulent rhinorrhea. Thickening of the mucous membrane alone (without accompanying opacification or air/fluid level), was not considered a criterion for abnormality. Evaluation of adenoid size was not requested. If the initial CT scan showed opacification or an air-fluid level, a second CT scan was scheduled approximately 3 weeks later unless the parent declined the follow-up CT. The CT images were interpreted by a board-certified radiologist and confirmed by 2 experts in the field of sinus disease at the University of Virginia.
RESULTS
Thirty-one children (17 male), who met all entry requirements were enrolled from March 1995 to February 1998. One boy withdrew from the study within 24 hours, leaving data from 30 patients available for analysis. Before the onset of purulent rhinorrhea, 23 children had a prodromal of serous or mucus rhinorrhea for 1 (n = 4) to 7 (n = 3) days (median, 2.5 days). Seven children had an abrupt onset of purulent rhinorrhea without a serous or cloudy mucoid prodrome. Fever was documented at home or in the office in 6 children, ranging from 38.0° to 39.3°C. Of the 27 children with abnormal CT scans on study entry, 13 were treated with cefuroxime axetil suspension and 14 were given placebo suspension (treatment arm based on table of random numbers and double-blinding of parents and physician was done in every case). Follow-up scans were obtained from 7 placebo-treated and from 9 cefuroxime axetiltreated children.
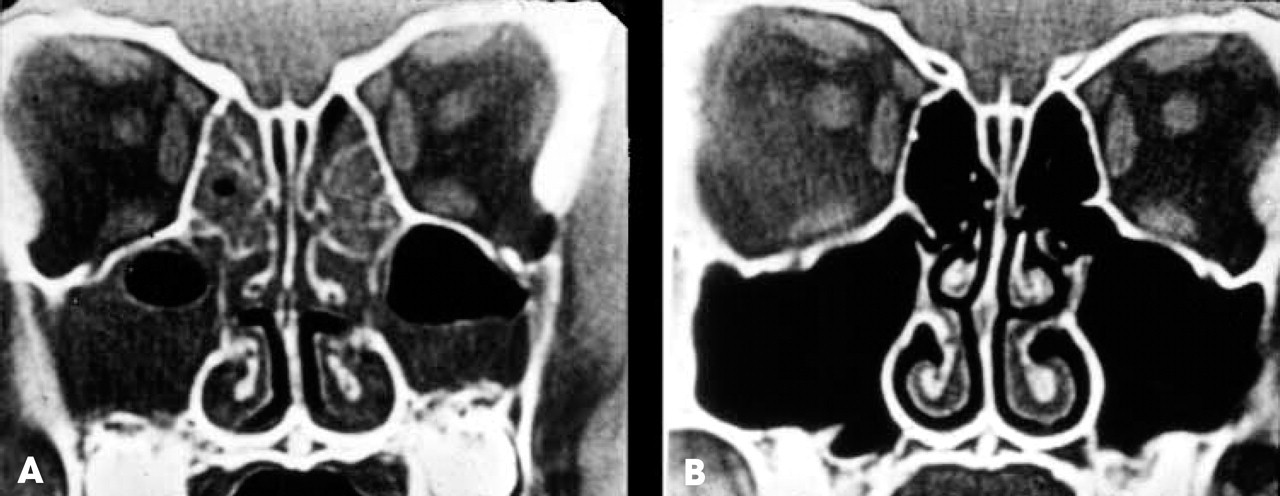
A, CT scan on study entry. Bilateral maxillary sinus effusions have air-fluid levels. Left maxillary sinus is almost completely opacified. B, CT scan 3 weeks later shows complete clearing of the maxillary and ethmoid effusions.
CT Images
Of the 30 children who underwent the initial CT, 21 (70%) had marked bilateral sinus opacification or air/fluid levels involving ethmoid and maxillary sinuses. One (3%) child had CT evidence of only bilateral maxillary sinus effusions. Five (17%) children had unilateral maxillary sinus effusions (Table 1). Three (10%) CT scans were normal on day 1. Seventeen of 27 children with sinus effusions on their entry CT scan had follow-up CT scans taken at 21 to 28 days after entry into the study (Table 1 and Fig 1). Ten (58%) of the 17 showed complete resolution of the effusion demonstrated on the initial CT scan (Fig 1). The 7 children with persistent sinus effusions on follow-up all showed clinical and radiographic improvement in at least 1 sinus. Of 7 placebo-treated children who had follow-up CT scans, 5 had been treated with antibiotics within 2 weeks of entry into the study because of worsening of clinical symptoms or persistence of profuse purulent rhinorrhea for 8 or more continuous days. Of 9 cefuroxime axetil-treated children who had follow-up CT scans, 5 (56%) had complete clearing of the effusion and 4 had some improvement on CT.
DISCUSSION
Our study documented CT scan-proven maxillary and often ethmoid sinus effusions in this pilot study of children with acute purulent nasal discharge of short duration. However, the nasal flush may have contributed to or been the sole cause of maxillary sinus effusions.
The CT image abnormalities from the study group usually normalized within 3 weeks by follow-up CT scan. Although there was no statistical difference in antibiotic-treated group and placebo-treated group for this parameter, there was a trend in favor of clearing or improvement by the antibiotic-treated group. Gwaltney et al 11 found positive sinus CT scans in 75% of 14 adult volunteers with the common cold. According to Gwaltney et al, the CT abnormalities in our study patients were more likely to show complete opacification of the maxillary or ethmoid sinuses than CT images of adults with common colds.
Deficiencies of Study
The most important deficiency of this study is the absence of microbial information from inside the maxillary sinus. The number of children who had CT scans without the prior saline solution flush is small. As such, it does not give a clear answer to the concern that the maxillary sinus effusions were iatrogenic as a result of reflux of saline solution into the maxillary sinus. Although it seems that children with complaints of purulent rhinorrhea are encountered every day in a busy pediatric practice, this study took 3 years for a single pediatrician to enroll 30 evaluable children. This is because we selected for those with profuse, green or yellow thick nasal discharge, required signed parental consent, and insisted on at least an initial CT scan. Children younger than 3 years with 1 exception were usually excluded from participation because they could not sit still during the CT scan that was not an ultra fast model.
We urge caution in interpretation of these data to mean that antibiotics are necessary to treat children with short-duration purulent rhinorrhea. This is not our intent.
CONCLUSION
In children with short-duration (mean duration, 5 days) purulent rhinorrhea, CT scans often demonstrate opacification and/or air fluid levels. Opacification of the maxillary or ethmoid sinuses means that there is liquid, not necessarily containing bacteria, in the sinus cavity. CT scans need to be ordered with discrimination and may not be useful to direct antibiotic therapy for purulent rhinorrhea. The diagnosis of acute sinusitis should be made according to guidelines published by the CDC/AAP. These guidelines clearly state that the presence of green or yellow color to nasal mucus is not a reason to diagnose acute sinusitis. To this we can add that viscosity, color, or CT-validated maxillary or ethmoid sinus effusion are not sufficient evidence to diagnose bacterial sinusitis in children with short-duration purulent rhinorrhea.
David Parsons, MD, Gregory Hayden, MD, and Ellen Wald, MD, generously gave critique of this manuscript. Jack Gwaltney, MD, reviewed each of the CT scans.