
Abstract
OBJECTIVE: To compare 5-, 7- and 10-day duration of antibiotic therapy for acute otitis media (AOM) in children.
STUDY DESIGN AND SETTING: Prospective nonrandomized 1-year evaluation of 3 treatment durations for AOM in a private pediatric setting. Outcomes assessed at 14 ± 4 days after start of therapy with clinical response categorized as cure, improvement, or failure.
RESULTS: A total of 2172 children were studied; 46.4% were ≤2-years-old. Antibiotics used were amoxicillin (61.9% of patients), trimethoprim/sulfamethoxazole (11.7%), cephalosporins (14.2%), amoxicillin/clavulanate (5.2%), and macrolides/azalides (4.8%). No overall difference in outcome was observed comparing the 5-day (n = 707), 7-day (n = 423), or 10-day (n = 1042) treatments, including children ≤2-years-old. However, in the subset who had an episode of AOM in the preceding month, outcome differed; 5-day treatment was followed by more frequent failure than 10-day treatment (P < 0.001). In logistic regression analysis, variables identified as contributing to a cure were: >2-years-old (P < 0.0001), no AOM in the preceding month (P = 0.07), or preceding 12 months (P = 0.03).
CONCLUSIONS: Our study supports the transition from 10 to 5 days for standard AOM antibiotic treatment duration in most patients. A 10-day regimen may be superior in children who have experienced an episode of AOM within the preceding month, a known risk factor for resistant bacterial infection in the otitis-prone patient.
Rising antibiotic resistance among bacteria that cause AOM is an important national concern 4 that might be helped through a reduction in overall antibiotic consumption. In addition, there is an increased realization that patient compliance with antibiotic therapy of acute respiratory infections often follows a path of adherence only until a clinical response occurs (typically 2 to 3 days) and perhaps an additional day or 2. 5 Thus, a shortened course of therapy may have been the typical treatment course for decades, albeit not at the physician's prescription. In this context, our group practice undertook a prospective 1-year evaluation of 3 antibiotic treatment durations for AOM.
METHODS AND MATERIALS
Patient Selection
Any child diagnosed with AOM by 1 of the 6 coinvestigators of the Elmwood Pediatric Group, Rochester, NY, and not enrolled in a pharmaceutical company-sponsored trial was eligible for inclusion in the analysis. The study was conducted for patients seen from January 1, 1996, to December 31, 1996. The diagnosis of AOM was based on 1 or more acute symptoms (otalgia, irritability, fever, sleeplessness, ear pulling) as well as 3 of 5 signs of AOM: (1) a full or bulging tympanic membrane (TM) with impaired mobility by pneumatic otoscopy; (2) purulent or cloudy middle ear effusion; (3) obscured TM landmarks; (4) discoloration of the TM (such as redness or yellow/gray); and (5) opacification or thickening of the TM.
Patients were excluded from analysis if they had a ruptured TM, a tympanostomy tube in their infected ear, significant gastrointestinal disorders that could effect oral antibiotic absorption, immunodeficiency, or other chronic medical conditions of concern.
Interobserver Reliability
All the physician investigators in the study are experienced in performing pneumatic otoscopic examinations. Four investigators (M.E.P., S.M.M., M.L.M., and W.H.) who contributed more than 80% of the patients studied perform in-office tympanocentesis and are validated otoscopists. To assess interob-server reliability, all participated in a diagnostic accuracy testing session (Outcomes Management Educational Workshops on “Diagnostic Accuracy in Acute Otitis Media”). Otoendoscopic video footage of tympanic membranes was viewed from 11 patients, including pneumatic otoscopy examinations, and rated each as normal, AOM, otitis media with effusion (OME), or retracted TM but otherwise normal. Agreement on normal was 100%, on AOM was 83%, on OME was 67%, and on retracted TM otherwise normal was 67%.
Microbiologic Investigations
None of the children evaluated in the study population of this report had a tympanocentesis performed in order to avoid any confounding therapeutic benefit of this drainage procedure. However, in 1996, tympanocenteses were performed on other children in the practice. This allowed characterization of the pathogens causing AOM and their antibiotic sensitivity in our practice. AOM isolates were identified by standard techniques. Streptococcus pneumoniae were screened with an oxacillin disk test. Isolates with a zone size <20 mm were assessed for penicillin susceptibility by MIC determination according to the National Committee for Clinical Laboratory Standards. 6 Beta lactamase production was determined for all Haemophilus influenzae and Moraxella catarrhalis by a nitrocephin-base test.
Antimicrobial Therapy
After a review of the literature by one of us (M.E.P.), 1 it was agreed within the group that during the 1996 year, 1 physician intended to prescribe 5-days duration of antibiotics as a routine, 2 preferred to use 7-days duration as their routine and 3 preferred to remain with 10-days duration, with a few exclusions (see earlier in this article). Compliance was assessed by parents’ report.
The selection of the antibiotic was at the discretion of the prescribing physician. Criteria for selection followed guidelines previously described. 7 In brief, amoxicillin (40 mg/kg/ day divided 3 times daily) was first-line therapy for children with recently untreated AOM; trimethoprim-sulfamethoxazole and erythromycin ethylsuccinate/sulfisoxazole were alternative first-line agents for presumed or documented penicillin-allergic patients. All other antibiotics with an AOM indication were considered second-line; they were used when children had a recent treatment failure after use of a first-line agent, a track record of 2 failures with a first-line treatment in the preceding 6 months or persistent AOM. 7 Antibiotic dosage was according to the package insert.
Outcome Evaluations
Patients were scheduled for follow-up pneumatic otoscopy evaluation 14 ± 4 days after starting treatment or sooner if symptoms suggested persistent AOM or another AOM episode. The clinical response was categorized as: (1) cure = clinical symptoms and signs of AOM were resolved, including resolution of middle ear effusion; (2) improvement = clinical symptoms resolved and otoscopic findings normalized except for persistence of middle ear effusion; and (3) failure = persistence of 1 or more symptoms and 2 or more signs of AOM. Clinical success was defined as cure + improvement. Patients who did not return for follow-up were categorized as clinical successes because if symptoms had occurred the child would have been brought back to our group for examination. Patients were considered unevaluable if they failed to complete the assigned duration of therapy (usually because of adverse taste, gastrointestinal side effects, or rash) or they reported poor compliance. Failure to complete the antibiotic course because of an inadequate clinical response was classified as a failure.
STATISTICAL ANALYSIS
Data were analyzed with SAS 6.10 software, and all results are reported for the evaluable patient population. The clinical responses (cure, success, and failure) were analyzed using 3 methods for testing the differences among the 3 treatment durations for AOM. First, χ 2 tests were performed for comparisons of treatment duration according to patient age, antibiotic selection, and earlier episodes of AOM. Second, a multivariate logistic regression model was fitted to the data with sex, age groups (≤2-years-old versus ≥2-years-old), antibiotic therapy (first-line antibiotic therapy versus second-line therapy) and prior episodes of AOM (within the preceding 1 month and 12 months) as factors and treatment duration as fixed effects. P values for the tests of fixed effects were reported and odds ratios and 95% confidence intervals were calculated for each variable. Tests for contrasts were used for pair-wise comparisons between treatment duration groups. Third, for those who failed treatment, Kaplan-Meier analysis was used to compare the times until failure in the 3 treatment duration groups. The time until failure was assessed from the beginning of treatment until 60 days later. For patients who failed before the end of treatment, this time was calculated as the ratio of the time on treatment divided by the assigned duration of treatment. For patients who did not have a follow-up and were in the “presumed success” category, a follow-up visit time was taken to be ≥ 60 days and censored. The Kaplan-Meier estimates were constructed and a log-rank test was used to test for the difference in the times until failure in the treatment duration groups. A P value of ≤0.05 was considered significant for all tests.
Patient population
RESULTS
Patient Population Demographics, Antibiotic Treatment, and AOM History
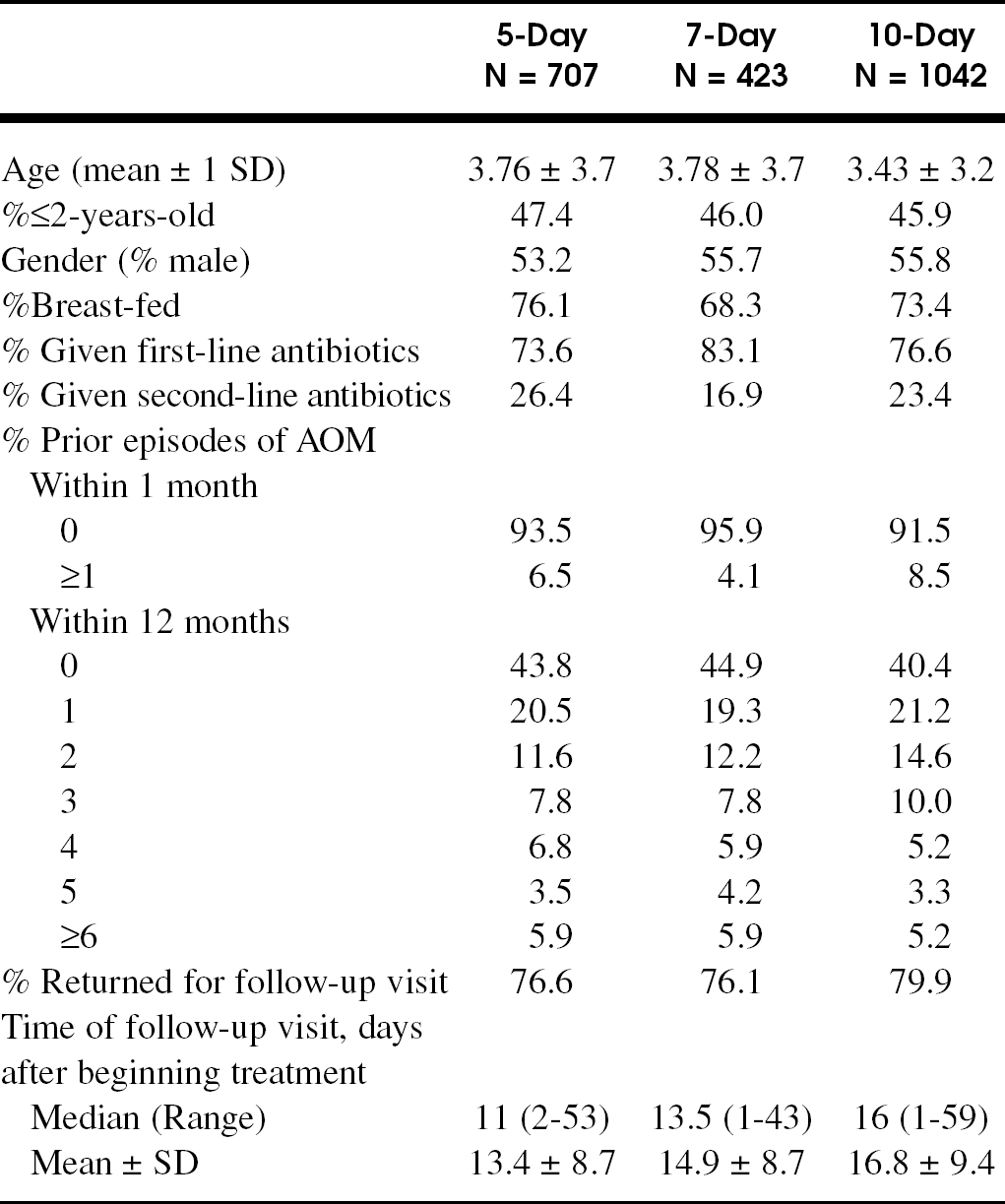
Of 2570 children with AOM seen by the 6 co-investigators, 2314 (representing 90% of AOM patients seen) were included in the study population; 256 children were excluded because they participated in pharmaceutical company-sponsored trials, had a ruptured tympanic membrane, a tympanostomy tube in the infected ear, significant vomiting or diarrhea, or had tympanocentesis performed. A total of 2172 (93.9% of 2314) were evaluable; 142 patients were unevaluable because of a failure to complete the duration of assigned antibiotic treatment (n = 33, 5-day treatment; n = 21, 7-day treatment; or n = 60, 10-day treatment) or poor antibiotic compliance (n = 28). Overall, the study population consisted of 55% males; 46.4% of the children were ≤2 years of age; and 73.3% were breast fed. A description of the patient population distribution among the 3 treatment duration groups is presented in table 1.
Antibiotics chosen for therapy of AOM and clinical outcome
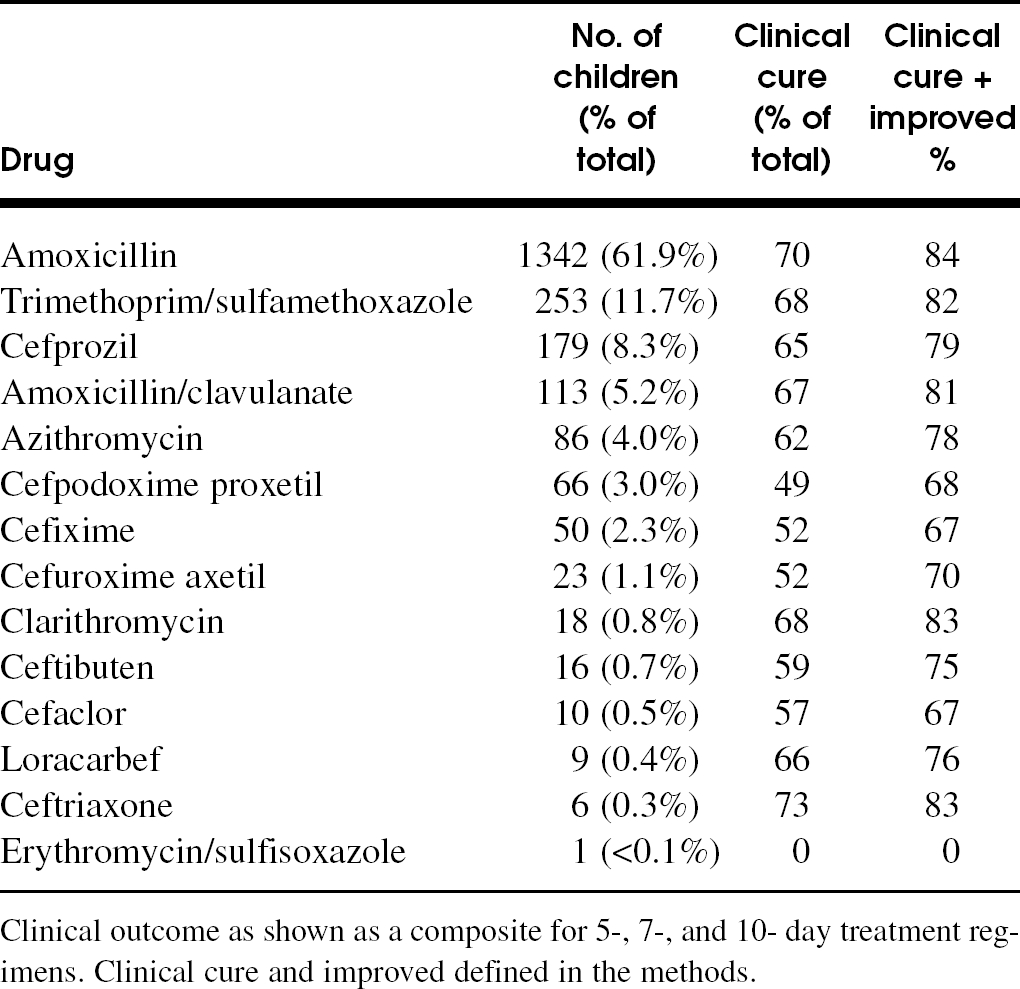
Clinical outcome as shown as a composite for 5-, 7-, and 10- day treatment regimens. Clinical cure and improved defined in the methods.
Clinical efficacy of 5-, 7- and 10-day antibiotic regimens in the treatment of AOM, according to antibiotic selection
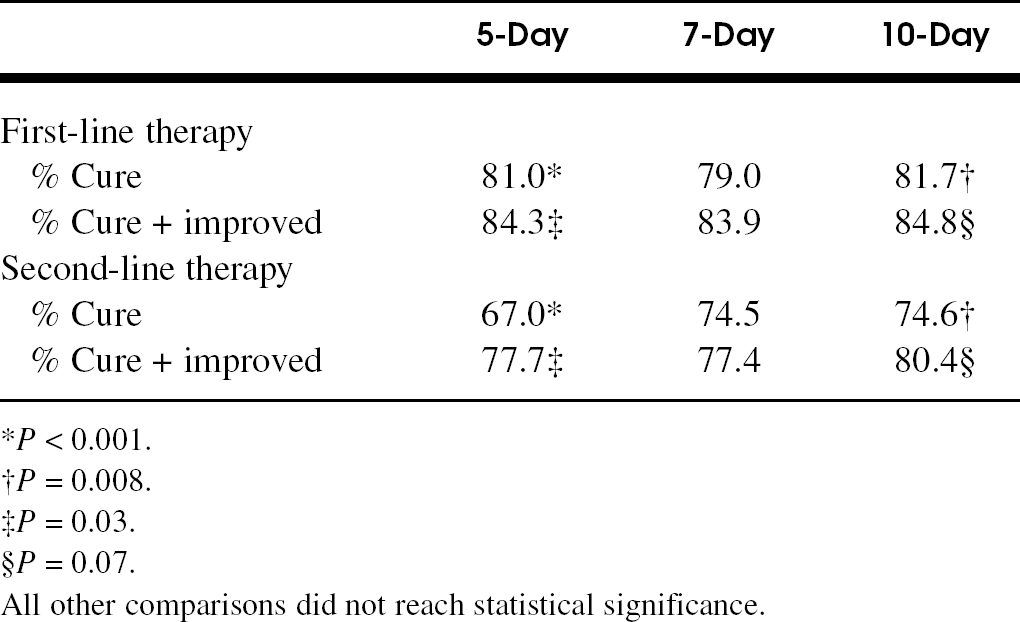
∗P < 0.001.
†P = 0.008.
‡P = 0.03.
§P = 0.07.
All other comparisons did not reach statistical significance.
Outcome According to Antibiotic Selection
The antibiotics used in treatment for the study and the overall clinical outcome for the 5-, 7-, and 10-day regimens combined are shown in table 2. A comparison of clinical efficacy of the 3 antibiotic durations according to first-line versus second-line antibiotic selection is shown in table 3. There were no differences in outcome among the 3 treatment durations when comparing across first line therapy and no differences when comparing across second line therapies. However, clinical cure and clinical success occurred significantly more often with first-line therapy compared with second-line therapy for the 5-day treatment and the 10-day treatment regimen (table 3). This result likely reflected selection second-line therapy for recently treated or persistent AOM. 7
Clinical efficacy of 5-, 7-, and 10-day antibiotic regimens in the treatment of AOM, according to patient age
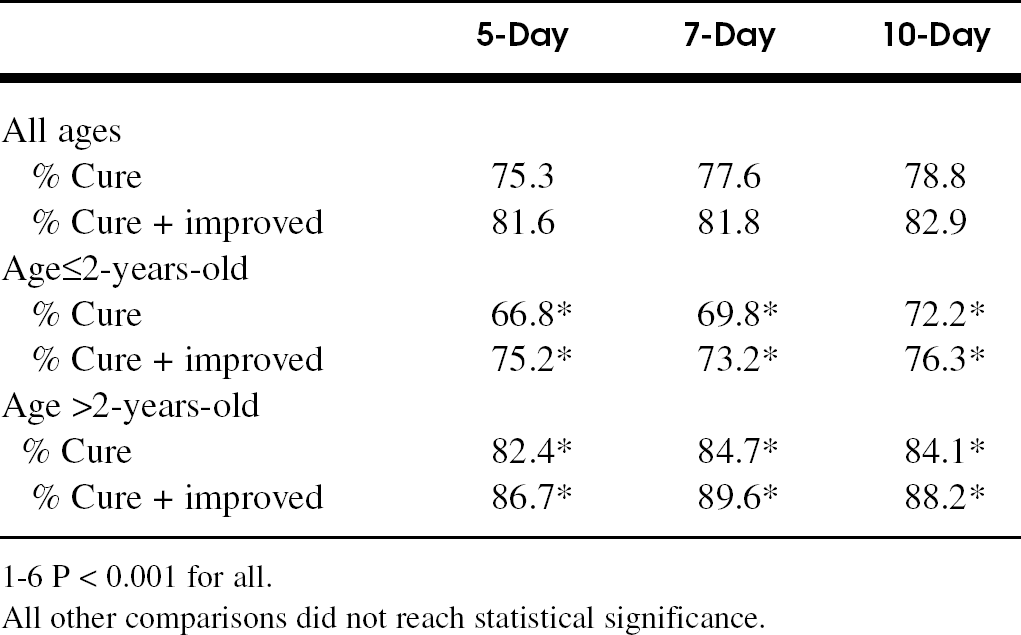
1-6 P < 0.001 for all.
All other comparisons did not reach statistical significance.
Outcome According to Patient Age
The overall clinical efficacies of the 5-, 7-, and 10-day antibiotic regimens in the treatment of AOM are shown in table 4. There was no difference in outcome when all ages were compared for clinical cure or clinical success, nor were there any differences in clinical outcome across treatment durations when the children were divided into 2 age groups: children ≤2-years-old and children >2-years-old (table 4). However, the percentage of clinical cure and clinical success was higher for children who were >2-years-old whether treatment was for 5-, 7-, or 10-days (P < 0.001 for all comparisons; table 4).
Outcome According to Earlier Episodes of AOM
Children who had no prior episodes of AOM within the preceding 1 month had a similar percentage of cure and success regardless of treatment duration (table 5). If the child had 1 or more episodes of AOM in the preceding month, the cure and clinical success rates were significantly lower in the 5-day and 7-day treatment arms, but not the 10-day treatment arm (table 5). For those children with ≥1 episodes of AOM in the prior month, the likelihood of cure or success was higher in the 10-day compared with the 5- or 7-day regimen (table 5). Children who had no AOM episodes within 12 months of enrollment had similar high cure rates regardless of treatment duration. Moreover, cure and/or success were less likely regardless of treatment duration if the child had ≥1 episode in the prior 12 months (table 5).
Confounding Factors, Multilogistic Analyses, Kaplan-Meier Estimates
The lower rate of cure and clinical success with second-line antibiotic therapy compared with first-line therapy occurred as a result of confounding in our antibiotic selection procedure. Second-line therapy was given because the child had persistent AOM, already experienced AOM in the prior month, or had already recently received first-line therapy. The correlation of second-line antibiotic choice and≥1 episode of AOM within 1 month was significant (P < 0.001).
Clinical efficacy of 5-, 7-, and 10-day antibiotic regimens in the treatment of AOM, according to number of prior episodes of AOM
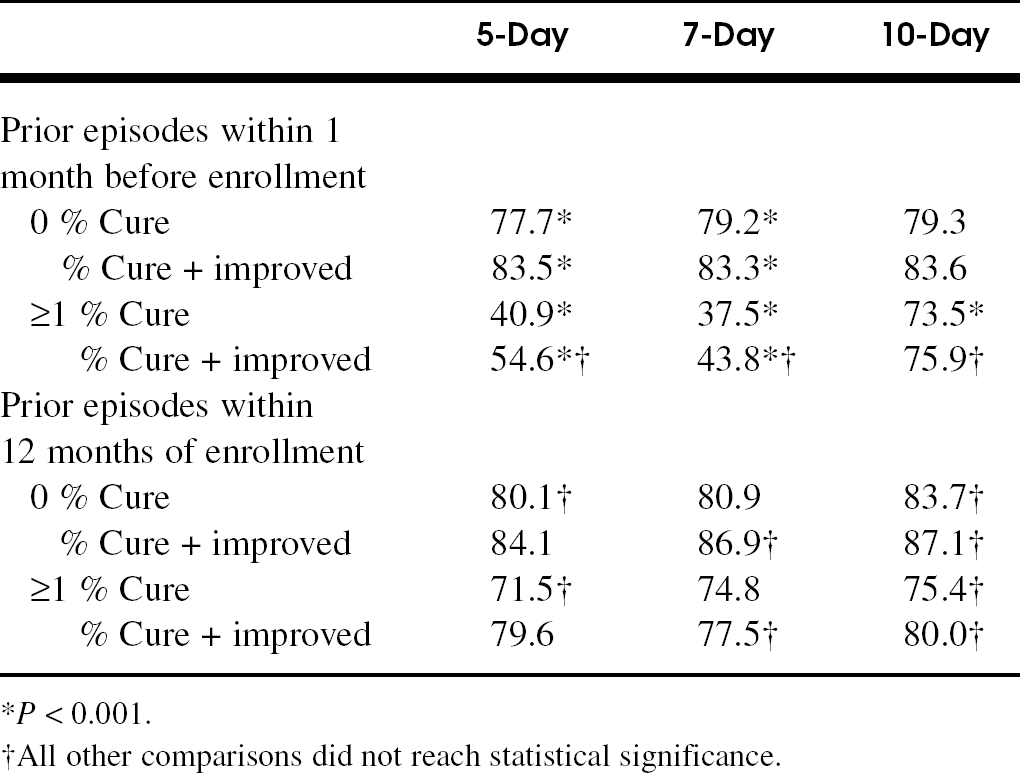
∗P < 0.001.
†All other comparisons did not reach statistical significance.
In multilogistic analysis, the variables identified as contributing to the cure of AOM as an outcome (with treatment duration as a fixed effect) were age ≥2-years-old (P < 0.0001), history of no episode of AOM in the preceding month (P = 0.07), history of no episode of AOM in the preceding 12 months (P = 0.03); treatment duration and first-line versus second-line antibiotic choice were not significant. The odds ratio (95% confidence interval) for cure of AOM was 1.88 (1.36 to 2.59) if children were >2-years-old versus ≤2-years-old, 0.64 (0.46 to 0.88) if children had ≥1 versus zero episodes of AOM in the preceding 1 month, 0.93 (0.88 to 0.99) if children had ≥1 episode versus zero episodes of AOM in the preceding 12 months, and 0.63 (0.41 to 0.99) if children were treated with 5-days of antibiotics versus 10-days. The marginal significance of the 5- versus 10-day regimen of antibiotics disappeared when age as a confounding factor was considered (OR = 0.78; 95% CI = 0.57 to 1.08, P = 0.13).
Kaplan-Meier estimates were constructed to compare the time until another AOM episode occurred in those who had another episode. There was no significant difference in time until an AOM failure occurred among the 5-, 7- and 10-day treatment groups (Fig 1P = 0.46 for 7- and P = 0.29 for 5- versus 10-day comparison).
Bacteriology Profile During Study Time Frame.
None of the studied children underwent tympanocentesis before enrollment. However, tympanocentesis wasperformed for other children in the practice on other study protocols. This information offers a pathogen profile in our patient population and the antibiotic resistance pattern of those isolates. Results of tympanocentesis for 24 children without recent (within 1 month) antibiotic treatment failure (tympanocentesis performed with acute pain as an indication) were as follows: 38% S. pneumoniae (22% relatively and 11% resistant), 12.5% H. influenzae (33% β-lactamase-producing), 12.5% M. catarrhalis (100% β-lactamase-producing), 4% S. pyogenes, 0% S. aureus, and 33% no bacterial growth. Results of tympanocentesis for 56 children with persistent or recurrent AOM were as follows: 14% S. pneumoniae (63% relatively resistant and 13% resistant), 7% H. influenzae (43% β-lactamase-positive), 5% M. catarrhalis (100% β-lactamase-positive), 5% S. pyogenes, 2% of S. aureus, and 55% no growth.
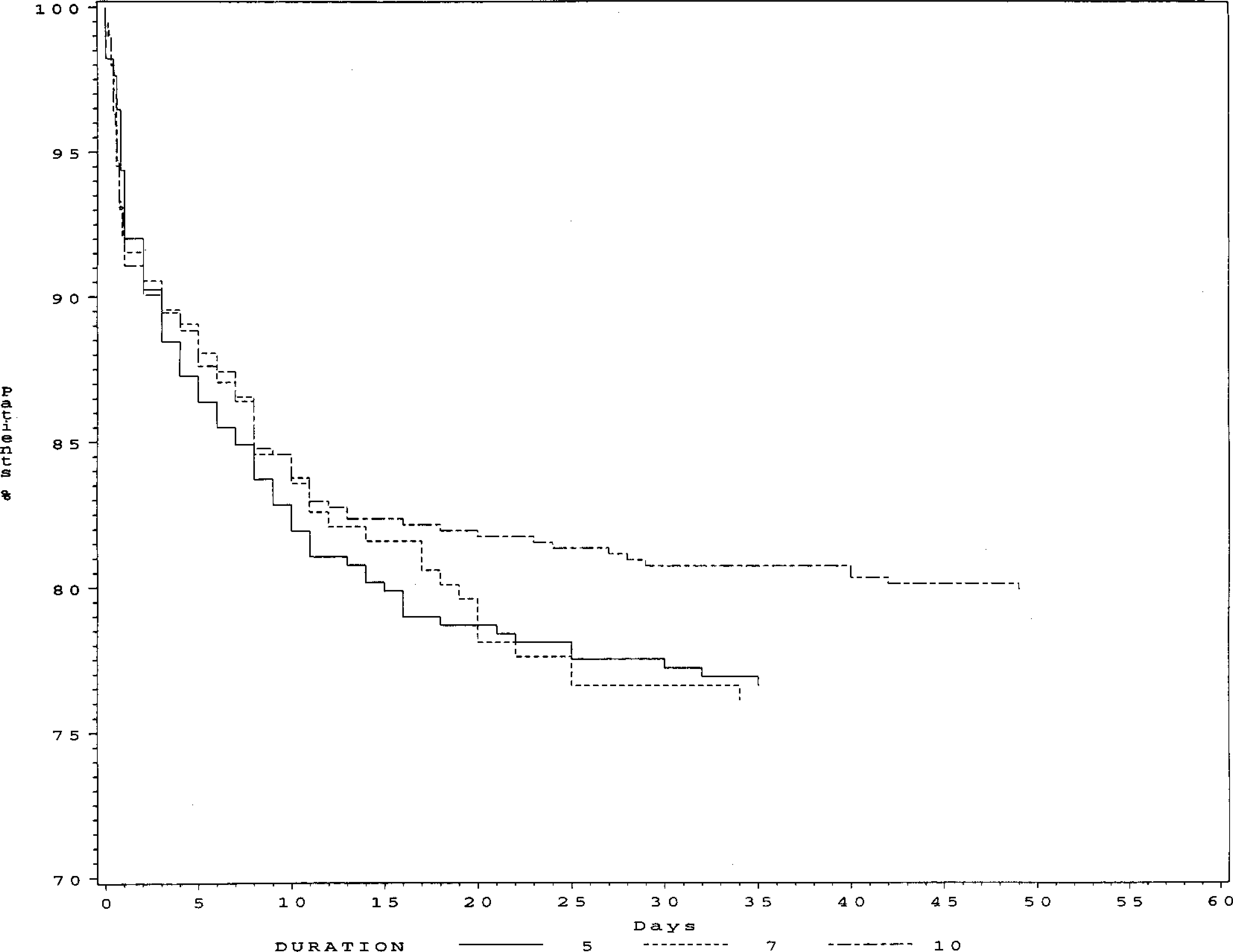
Kaplan-Meier estimate for the time until a new AOM episode occurred after enrollment into the study among those who had a new episode within 60 days after 5-, 7- and 10-days antibiotic treatment regimens.
DISCUSSION
In this practice-based prospective analysis of 2172 children, we found no significant differences in outcome when the 5- and 7-day treatment regimens were compared with the 10-day regimens of the various antibiotics used. Consistent with prior studies, antibiotic treatment failure was observed more frequently in children under 2 years of age, 8–11 regardless of treatment duration. The difference in percentage of cure after a 5-day regimen vs a 10-day regimen in children <2-years-old was not significant, a finding consistent with the meta-analysis of Kozyrskyj et al, 2 but differing from the results of Hoberman et al 9 and Cohen et al. 12,13
Antibiotic selection was not random but reflected parameters often used in primary care practice in the routine care of patients with AOM. 7 Amoxicillin and trimethoprim/sulfamethoxazole (TMP/SMX) were first-line agents. Second-line antibiotics were selected in 25% of episodes of AOM because the child recently had a treatment failure after use of amoxicillin or TMP/SMX, a track record of 2 failures with one or the other of these agents in the preceding 6 months, or had a persistent or recurrent AOM after treatment with an antibiotic during the preceding month. As a consequence of the antibiotic selection process, clinical cure and clinical success occurred more frequently with first-line therapy compared with second-line therapy. First-line antibiotic treatment failures and second AOM episodes within 1 month more often are associated with resistant bacteria, and such bacteria are more difficult to eradicate, 14–16 including with second-line antibiotic agents 7,9–11 regardless of treatment duration.
Children who had no prior episodes of AOM within the preceding 1 month had a similar percentage of cure and success regardless of treatment duration. However, 1 or more episodes of AOM within the preceding month had a substantial impact on the likelihood of clinical success in the 5-day and 7-day treatment regimens compared to the 10-day regimen. This group of children therefore might be categorized as otitis-prone; they are more likely to be infected with resistant bacteria and more likely to return to an environment where reacquisition of resistant strains might occur. The prophylactic benefit of a 10-day antibiotic regimen surfaces as a significant benefit in this type of patient. Across all treatment durations the absence of any AOM episodes in the prior 12 months was typically followed by a cure. The advantage of longer treatment (10 days) compared with the 5- and 7-day regimens in the otitis prone child was not apparent when the entire 12-month history of AOM was factored into the analysis. When the AOM episodes clustered in the 3 months before enrollment, a trend favoring 10-day regimens emerged but significance was not achieved (P = 0.07).
With multivariable analysis, clinical outcome in AOM treatment was most influenced by patient age (<2 years) and a history of AOM. The Kaplan-Meier curves showed that most failures took place not during, but after treatment in all 3 antibiotic treatment duration groups. These data support the hypothesis that the benefits of longer therapy, when they occur in children, might be the result of the prophylactic effects of antibiotics. 12,13
Our study has limitations that should be considered. The design was randomized and prospective, but randomization was unbalanced and not performed in a typical manner; randomness occurred as a consequence of patient appointments for otalgia visits with different physician co-investigators. There was no standardized protocol for antibiotic selection; selection reflected the treatment successes of prior AOM infections in a particular patient and differing clinical experience with a variety of second-line agents. Although all investigators were validated otoscopists and interobserver variability was reasonably good, sensitivity and specificity of AOM diagnosis on a case-to-case basis could have been variable. As each investigator knew which treatment regimen they were prescribing, there is a chance for bias. The patient population was drawn from a suburban private pediatric practice in a limited geographic area. The pattern and percentages of resistant bacterial pathogens causative of AOM as seen in this study are similar to general trends in the United States, but geographic variations have been described in such resistance rates. We excluded children if they had a ruptured tympanic membrane or tympanostomy tubes based on a very small prior study 17 suggesting that shorter courses of therapy may not be effective in such patients and because we routinely use antibiotic ear drops as a preferred first-line therapy in those with tympanostomy tubes before proceeding to oral agents. The possibility of bias among parents regarding if and when they would return for follow-up care may have occurred. A trend for a slightly earlier return for follow-up among 5-day treatment duration patients than 7- and 10-day treatment groups occurred. We did not perform tympanocentesis on our study population; this procedure was done on a companion group of our patients to provide information regarding the resistance patterns and pathogens circulating in our study population. This does not assure that the tympanocentesis and nontympanocentesis populations are otherwise indistinguishable. We only assessed outcome at approximately 2 weeks after enrollment in the study. Longer-term follow-up would have been of interest. In the meta-analysis by Kozyrskyj et al 2 and the study by Cohen et al, 12 the small statistical differences that were observed between shorter and longer term treatment durations dissipated with a longer follow-up of 30 to 45 days.
Patient and parents prefer short-term antibiotic therapy. 18 Improved compliance has been documented. 19 Whether a beneficial impact would occur on overall antimicrobial pressure that encourages the selection of resistance strains requires further study. No difference was observed in the study by Cohen et al. 12 Nevertheless, patients who do not complete their antibiotic prescriptions may save the remaining amounts for subsequent use. During storage, suspension antibiotic formulations rapidly lose potency. Low concentrations of antibiotic clearly provide a selective advantage for resistant strains in vitro and probably in vivo. 20 Thus, the surreptitious use of left over antibiotic prescriptions for AOM may be a major contributor to the antibiotic resistance problem. This notion should be validated.
We thank Vladamir Dragalin, PhD, Department of Biostatistics, University of Rochester Medical Center, for his biostatistical analysis.