
Abstract

Pseudostratified ciliated columnar epithelium is typically found lining the greater part of the upper respiratory tract. It is also found in the lacrimal sac, part of the tympanic cavity, and the eustachian tube. The presence of this typical respiratory epithelium is uncommon in cysts that derive from odontogenic epithelium, and therefore rare within a mandibular cyst.
CASE REPORT
A 59-year-old white man was referred by his dentist for treatment of a cyst of the anterior mandible. There had been acute swelling of the lower lip and lower labial vestibule several days earlier, when he first presented. Pus drained into the vestibule when the dentist examined him, and the acute swelling resolved. The patient denied prior episodes of pain or swelling in that area. The incisor teeth had been removed years earlier.
On examination, there was a smooth, fluctuant swelling occupying most of the lower labial vestibule and fixed to the underlying bone. There was no neurosensory deficit. A panoramic radiograph showed a large unilocular radiolucency in the region of the symphysis menti, between the roots of the canine teeth. The diagnosis of an acutely infected odontogenic cyst seemed most likely.
The lesion was easily removed by enucleation, owing to a thick fibrous capsule. During the procedure it was conspicuous that the lesion primarily occupied the soft tissues anterior to the mandibular symphysis and had created a depression in its anterior cortex. The roots of the canine teeth were not involved. The patient had an uneventful recovery.
Microscopic examination (Fig 1) showed a fibrous connective tissue cyst wall, lined by pseudostratified ciliated columnar epithelium. The lining was thin, only 1 or 2 cells thick. Acute and chronic inflammatory cells and hemosiderin deposits were scattered throughout the cyst wall.
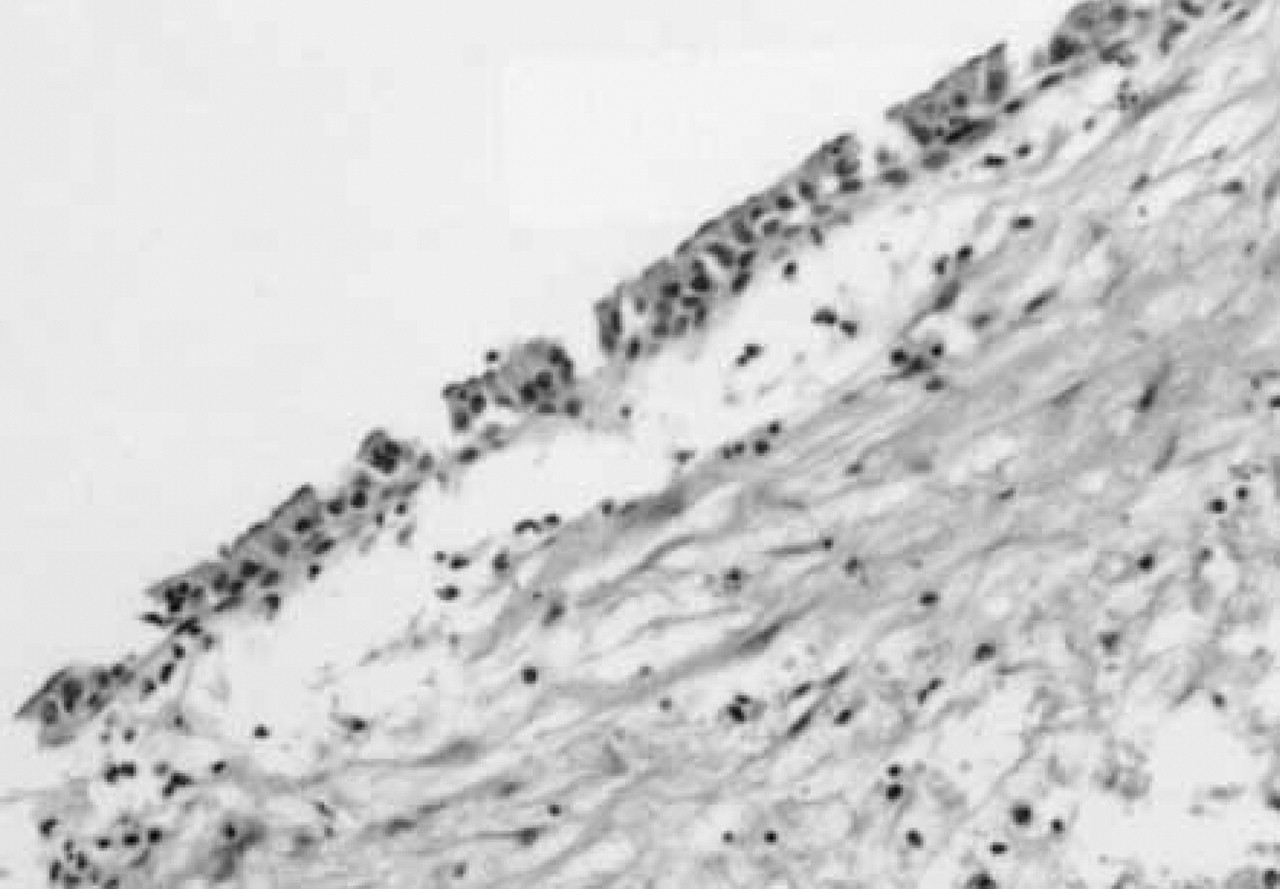
Midline mandibular cyst is lined by pseudostratified ciliated columnar epithelium, typical of the respiratory mucosa. (Hematoxylin-eosin stain; original magnification × 240.)
The patient's surgical history was of note for a septorhinoplasty after an accident 40 years earlier. It was not until after removal of the cyst, when he was informed of the unusual pathology, that the patient recalled having had a simultaneous chin augmentation using the bone and cartilage that had been removed from the nose. The patient did not recall the exact details of these procedures, and there were no records available.
DISCUSSION
Several explanations have been offered in literature for the rare occurrence of respiratory epithelium within a mandibular cyst. Some authors favor transformation through metaplasia of squamous epithelium. 1 Others believe that respiratory epithelium can develop from rests of pluripotential cells left in the mandible during development. 2 A final explanation is accidental implantation from surgical intervention or trauma. 3 The technique of chin augmentation with nasal bone or septal cartilage was frequently performed in the past. 4,5 Because of the theoretical possibility of development of a mucosal cyst, it was recommended to remove all mucosa from the graft. 4 Anastassov and Lee 3 have reported a mucocele that formed 39 years after augmentation genioplasty with a nasal osteocartilaginous graft. Because of the history and the medioanterior mandibular location in our case, it appears most likely that respiratory epithelium was transferred from the nasal region when the augmentation genioplasty was performed 40 years ago. This would make it only the second reported instance of respiratory epithelial implantation during cosmetic genioplasty.
SUMMARY
The case of a mandibular cyst lined with an unusual respiratory epithelium is described. The pathogenesis of this cyst may be related to implantation of respiratory epithelium during chin augmentation with an osteocartilaginous graft 40 years earlier.