
Abstract

Neurofibromatosis type 2 (NF2) is caused by a mutation on chromosome 22 1 and is characterized by the bilateral occurrence of vestibular schwannoma on the eighth cranial nerve. 2 Although this disease has been demonstrated to be associated with several complications, such as intracranial neurogenic tumors, spinal tumors, and presenile lens opacities, 3–5 it has not to our knowledge been reported to be accompanied by cervical schwannoma derived from cranial nerves. In this report we suggest the occurrence of cervical schwannoma in patients with NF2 by demonstrating 2 such cases involving cervical schwannoma derived from the vagal or hypoglossal cranial nerve.
CASE REPORTS
Five cases of NF2 were seen at Kansai Medical University Hospital between 1992 and 1996. All patients showed bilateral vestibular schwannoma of the eighth nerve and were followed up for more than 2 years. The patients' average age was 29.4 years (range, 17–47 years), and 4 of the 5 patients were women. Complications of cranial nerve schwannoma have been observed in the 2 cases described here.
Case 1
A 47-year-old man with a 5-year history of a right-sided sub-mandibular 4 × 4-cm mass came to our hospital in April 1996 for evaluation. His family history was unclear because he had lost contact with his family. A cervical CT revealed a well-delineated mass on the dorsal side of the right submandibular gland (Fig 1). Surgery was performed in July 1996. The mass was adhered to the submandibular gland craniomedially and was compressing it. It was unexpectedly derived from the hypoglossal nerve under the caudal side of the posterior belly of the digastric muscle. The encapsulated solid tumor was resected and was histopathologically demonstrated to be a schwannoma.
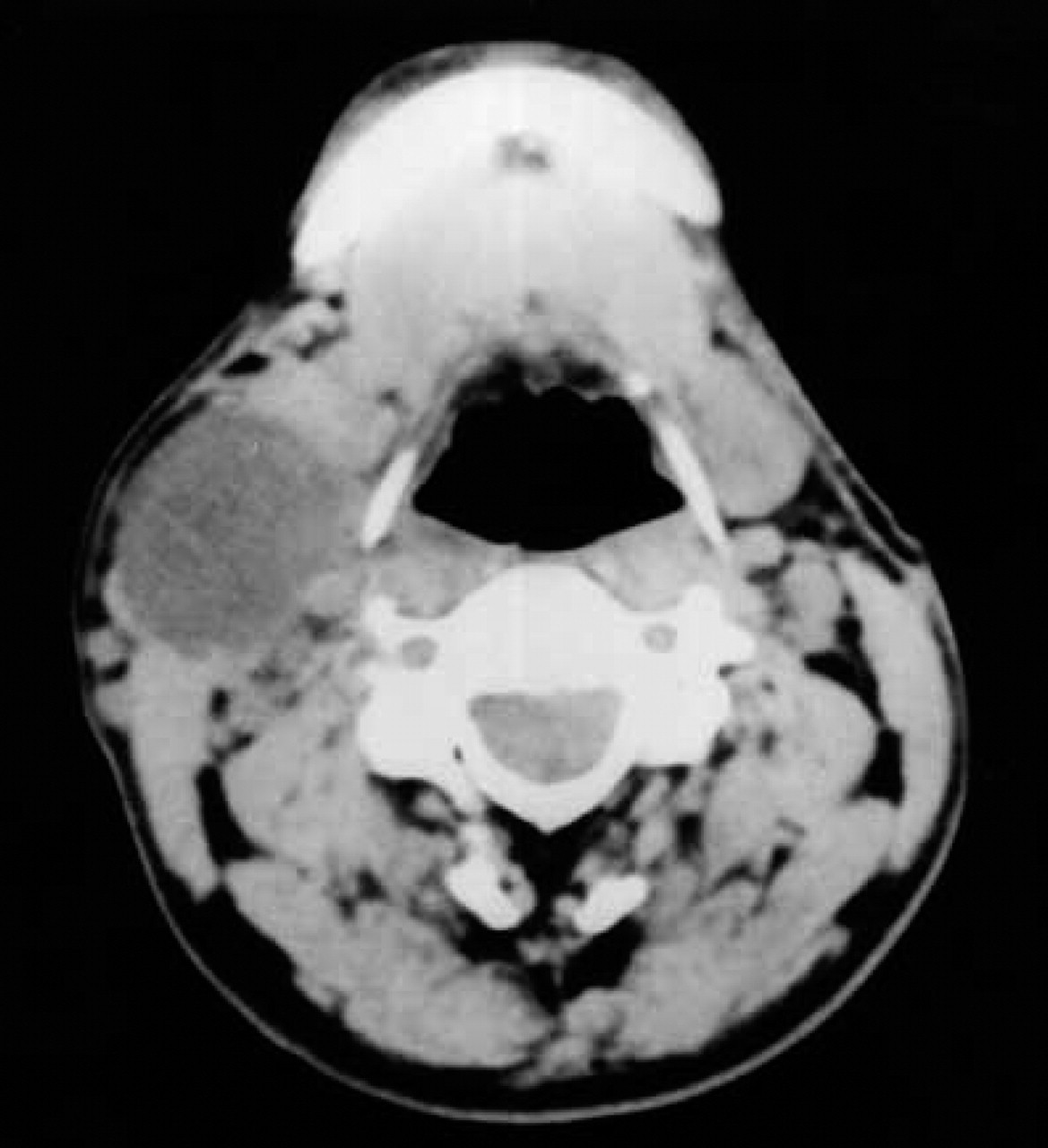
CT in neck (case 1) reveals well-delineated enhanced mass on dorsal side of right submandibular gland.
The patient returned to our hospital in July 1997 with a 4-day history of floating dizziness and nausea. An audiogram revealed bilateral sensorineural hearing impairment of the high-tone diminishing type. Acoustic brainstem response showed prolongation of bilateral I-V waves. MRI of the head revealed enhanced masses in the bilateral internal acoustic canals (IACs) (Fig 2). MRI of the spinal cord showed a tumor at the C3 level (Fig 3) compressing the spinal cord and multiple nodules positive for enhancement effects in the thoracic and lumbar spinal cord (data not shown). In September 1997, the tumor in the cervical spinal cord was resected at the orthopedic department of our hospital. Pathologic examination of the specimen demonstrated neurofibroma. Because the patient had the tumors in the bilateral IACs and the neurofibroma in the spinal cord, he was diagnosed as having NF2. The small nodules in the thoracic and lumbar spinal cord were suspected to be multiple neurogenic tumors.
Case 2
A 33-year-old woman with a 3-week history of right-sided tinnitus came to our hospital in October 1993 for evaluation. Otoneurologic examination indicated severe sensorineural hearing loss on the audiogram and no response in acoustic brainstem response in the right side of the ear. MRI of the head showed a mass (1.5 cm in diameter) on the right side of the cerebral falx suggesting meningioma and bilateral but right-side dominant cerebello-pontine (CP) angle masses for enhancement effects (Fig 4). Although family history revealed nothing clinically relevant, the patient had a history of cervical spinal neurofibroma resection at 14 years of age. From these clinical data taken together, we diagnosed the patient as having NF2. In January 1994 the patient underwent resection of the right-sided CP angle mass in the neurosurgical department. The mass originated from the vestibular nerve and was histopathologically demonstrated to be a schwannoma.
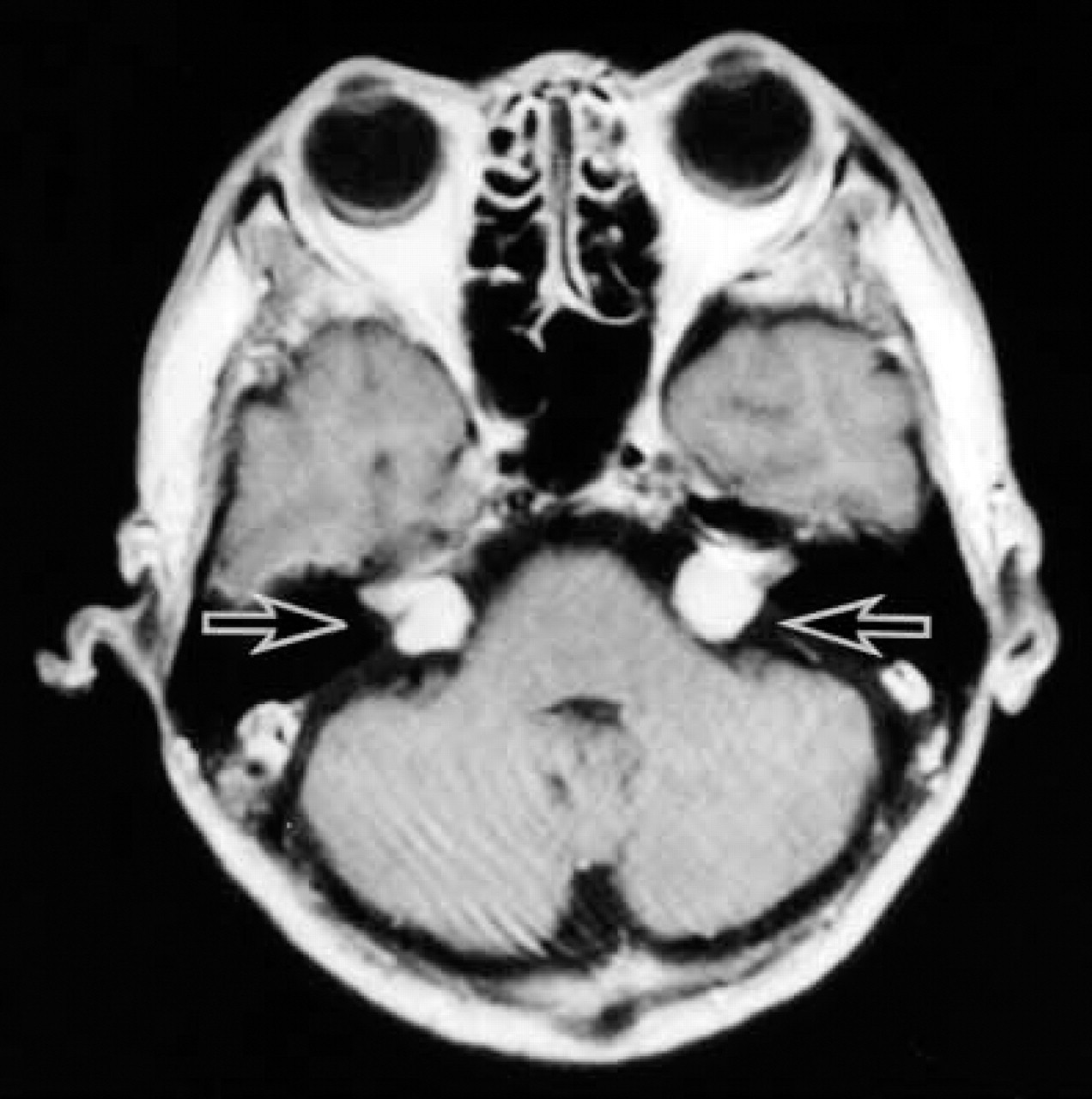
Enhanced MRI T1-weighted image of head (case 1) reveals enhanced masses (arrows) in bilateral IACs.
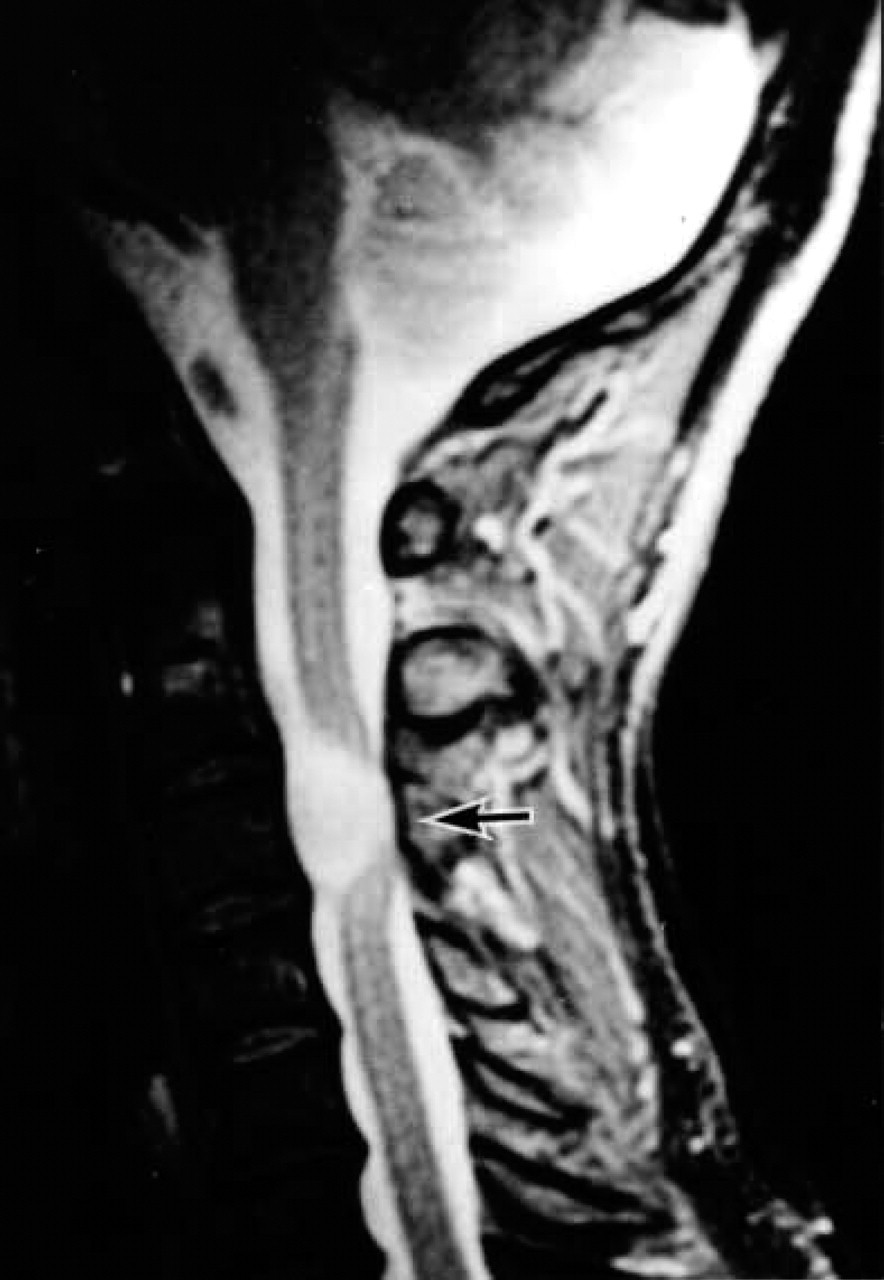
Enhanced MRI T1-weighted image of spinal cord (case 1) shows enhanced tumor at the C3 level (arrow).
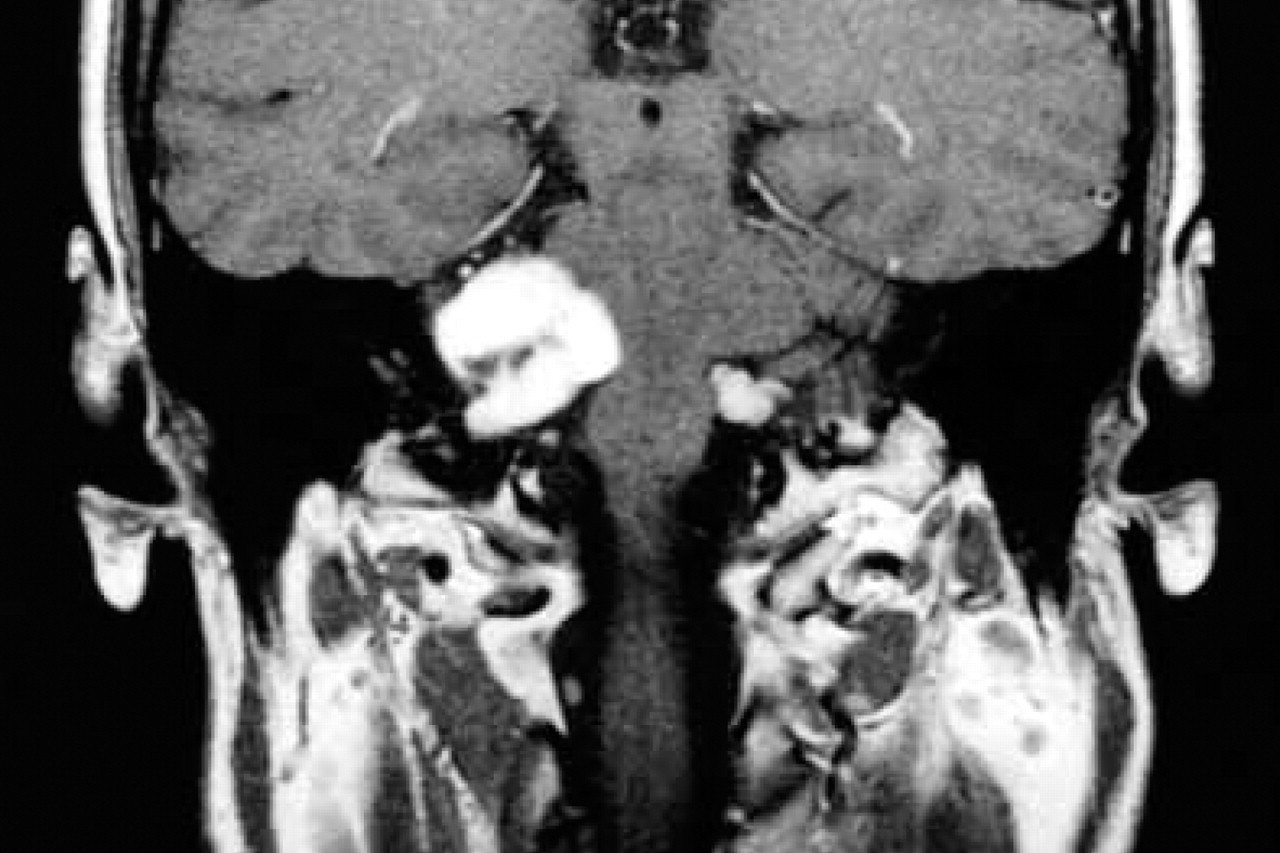
Enhanced T1-weighted image of head (case 2) shows bilateral but right-side dominant CP angle masses as enhancement effects.

MRI T1-weighted image of neck (case 2) reveals well-defined mass on dorsal side of internal (I) and external (E) carotid arteries and jugular vein (J), which were close together.
The patient had a 3-year history of an asymptomatic cervical mass and returned to our hospital in July 1998. Physical examination indicated a left-sided 4 × 4-cm mass under the sternocleidomastoid muscle, which was elastic and hard, demonstrated poor movement cephalocaudally, and was not pulsatile. A cervical MRI revealed a well-defined enhanced mass on the dorsal side of the internal and external carotid arteries and jugular vein, which were close together (Fig 5). The mass was resected with the vagal cranial nerve at the central and peripheral ends and was histopathologically demonstrated to be a schwannoma derived from the vagal cranial nerve.
DISCUSSION
According to the NIH diagnostic criteria, 2 a patient with bilateral vestibular schwannomas is immediately considered to have NF2. These criteria also indicate that patients with NF2 often have intracranial neurogenic tumors, including meningioma, schwannoma, and neurofibroma. Moreover, an association with spinal tumors has been reported in NF2 in addition to these criteria, and the necessity of spinal MRI is emphasized to find spinal tumors when bilateral vestibular schwannomas are detect-ed. 2,4 Although the transmission of NF2 was not confirmed in the family histories of our 2 patients, they fulfilled the criteria and were judged to have NF2 because of bilateral vestibular schwannomas, as well as spinal neurofibromas (cases 1 and 2) and meningioma (case 2).
In addition, these cases were complicated by lower cranial nerve schwannomas in the neck. Although we encountered only 5 cases of NF2, the presence of schwannomas in 2 of these patients suggests a high incidence of this combination. Although Kuchna et al 5 reported a patient with NF2 showing bilateral vestibular schwannoma complicated by multiple neurogenic tumors, there have been few reports of patients with NF2 with schwannomas originating from the lower cranial nerves. It is likely that these lower cranial nerve tumors in the neck have been treated separately from the treatment of NF2. Head, spinal, and cervical tumors in NF2 seem to appear asynchronously, and cervical tumors are generally resected at head and neck surgery departments independently of neurosurgical and orthopedic departments, without mutual communication. Therefore we emphasize the importance of examination not only of cranial and spinal tumors but also of cervical tumors, which are not, however, included in the NF2 criteria at present. Reports on the complications of these neck tumors in NF2 may increase in number in the future in proportion to the development and spread of MRI and CT use.