
Abstract
OBJECTIVES: To analyze oncologic results, prognostic factors, and consideration of transglottic tumors as a separate entity in 73 patients with T3 glottic carcinoma treated by surgery ± radiation therapy at La Paz University Hospital from 1984 to 1994.
METHODS: Sixty-four patients underwent a total laryngectomy; neck dissection was performed in 50 patients; 29 patients received postoperative radiotherapy.
RESULTS: The 5-year overall survival, cause-specific survival, and relapse-free survival rates were 58.1%, 66.8%, and 63.7%. Univariate analysis revealed prognostic significance for age, dyspnea, initial tracheostomy, and pathologic lymph node status. No difference was found when comparing survival and relapse rates between transglottic and glottic tumors.
CONCLUSION: Surgery provides acceptable rates of cancer control and survival for patients with T3 glottic carcinoma. Older patients, patients with positive neck nodes, and those presenting with dyspnea have worse prognosis. The term transglottic is merely descriptive and has little impact on prognosis.
A T3 glottic cancer is defined as a cancer of the vocal cord with fixation of the hemilarynx but clinically confined to the larynx, ie, not extending to the thyroid cartilage or the soft tissues beyond the larynx. 1 Vocal cord fixation by a glottic cancer is usually caused by replacement of the thyroarythenoid muscle by tumor. It indicates an advanced stage (stage III), with eventual invasion of the subglottis, the supraglottis, and the paraglottic space.
With regard to T3 glottic tumors, some controversial issues need to be clarified.
Best therapeutic option. The appropriate therapy for T3 glottic tumors is still a matter of debate. Treatment options include surgery alone or associated with radiation therapy; induction chemotherapy followed by radiation or surgery based on tumor response; and radical radiation therapy with salvage laryngectomy for recurrences. 2–6
Main prognostic factors. Despite refinements in therapy, prognosis for patients with T3 glottic cancer varies widely. This variation may be explained not only by treatment-related factors but also by other clinical and pathologic factors. 7–9 The identification of prognostic factors could provide a more rational patient selection for therapy in order to accomplish the ultimate goal of therapy, ie, improvement of survival.
Consideration of transglottic tumors as a separate entity. The term transglottic is imprecise and does not imply a site of origin. Although the current AJCC and UICC classification system does not provide a separate category for transglottic cancer, these lesions have been stated to be more aggressive than “pure” glottic tumors, having higher incidence of cervical metastases and requiring more aggressive therapy. 10
To address these issues we reviewed the clinical notes from 73 consecutive patients with T3 glottic (or transglottic) squamous cell carcinoma of the larynx treated by surgery ± radiation therapy at La Paz University Hospital from June 1984 to June 1994.
PATIENTS AND METHODS
Data were collected retrospectively from a departmental database, and the notes were reviewed. The original tumor description was considered for this study. Clinical stage was assigned in accordance with the American Joint Committee for Cancer Staging. Patients included 72 men and 1 woman ranging in ages from 38 to 81 years (mean, 60 years). Distribution according to AJCC clinical stage was as follows: T3N0, 58 (79%) patients; T3N1, 8 (11%) patients; and T3N2, 7 (10%) patients. No patients were clinically T3N3. Most patients (64 of 73) underwent total laryngectomy; near-total laryngectomy and partial laryngectomy were performed in 6 and 3 patients, respectively. Six (8%) patients required a tracheostomy before the definitive surgical treatment for symptoms of airway obstruction. The decision of performing a neck dissection and its extent varied according to the surgeon's choice at the time of surgery. All patients with positive neck nodes underwent comprehensive neck dissections, which consisted of functional or radical neck dissections depending on the N stage. In patients with clinically negative neck nodes (n = 58), an elective functional neck dissection was performed in 35 patients (25 unilateral and 10 bilateral); a policy of observation or radiotherapy was followed in 13 and 10 patients, respectively. Overall, 29 patients received radiation therapy after surgery. All patients were followed until death or a minimum of 5 years. The median follow-up for survival was 54 months. Site of recurrence was considered to be at the most proximal site.
The major end points were overall survival, cancer-specific survival, and relapse-free survival. Factors analyzed included: age, sex, smoking habits, alcohol intake, the presence of dyspnea, initial tracheostomy, tumor location (glottic vs transglottic) including specific laryngeal-involved structures, clinical and pathologic lymph node status, and histologic grading. Transglottic tumors were defined as those lesions clinically extending to the supraglottis site from the glottis, ie, the central mass involving the vocal cord. Therefore, supraglottic tumors extending to involve the glottis were excluded from this review. Tumors were considered “pure” glottic tumors when limited to the vocal folds, including the anterior and posterior commissures.
The SPSS program (Statistical Package for the Social Sciences Plus) was used for statistical analysis. Survival estimates were obtained using the method of Kaplan-Meier, and the log-rank test was used for univariate testing of potential prognostic factors. Multivariate survival analysis was performed by Cox proportional hazards regression. Fisher exact test and χ2 test were used to assess the statistical significance of association of glottic vs transglottic tumors with different parameters. A P value of less than 0.05 was considered statistically significant.
RESULTS
After a minimum follow-up of 5 years, 39 (53%) patients were alive with no evidence of disease, 23 (32%) died of cancer, and 11 (15%) died of unrelated causes. The 5-year overall survival, cause-specific survival, and relapse-free survival were 58.1%, 66.8%, and 63.7%, respectively. In patients who died of cancer, tumor recurred locally in 12 (52%) patients, in the neck in 5 (22%) patients, and in 6 (26%) patients developed distant metastases. Surgical complications included fistula (n = 16), seroma (n = 20), wound dehiscence (n = 20), infection (n = 14), and hemorrhage (n = 2). One patient died in the early postoperative period because of myocardial infarction. Stomal recurrences occurred in 5 patients.
Univariate analysis on overall survival, cancer-specific survival, and relapse-free survival revealed prognostic significance for age, dyspnea, initial tracheostomy, and pathologic lymph node status (Table 1). Patients older than 67 years had a smaller chance of survival when compared with younger patients. In addition, patients presenting with dyspnea at the time of diagnosis, those requiring initial tracheostomy, and patients with pathologically positive nodes had worse prognosis. Differences in survival rates according to sex, consumption of alcohol and tobacco, tumor location, clinical lymph node status, and histologic grading were not observed. When performing multivariate analysis on overall survival, pathologic lymph nodes status was found to be the most predictive factor of survival (P = 0.008). Initial tracheostomy was moderately predictive (P = 0.02), and age did not reach statistical significance (P = 0.1).
Prognostic factors
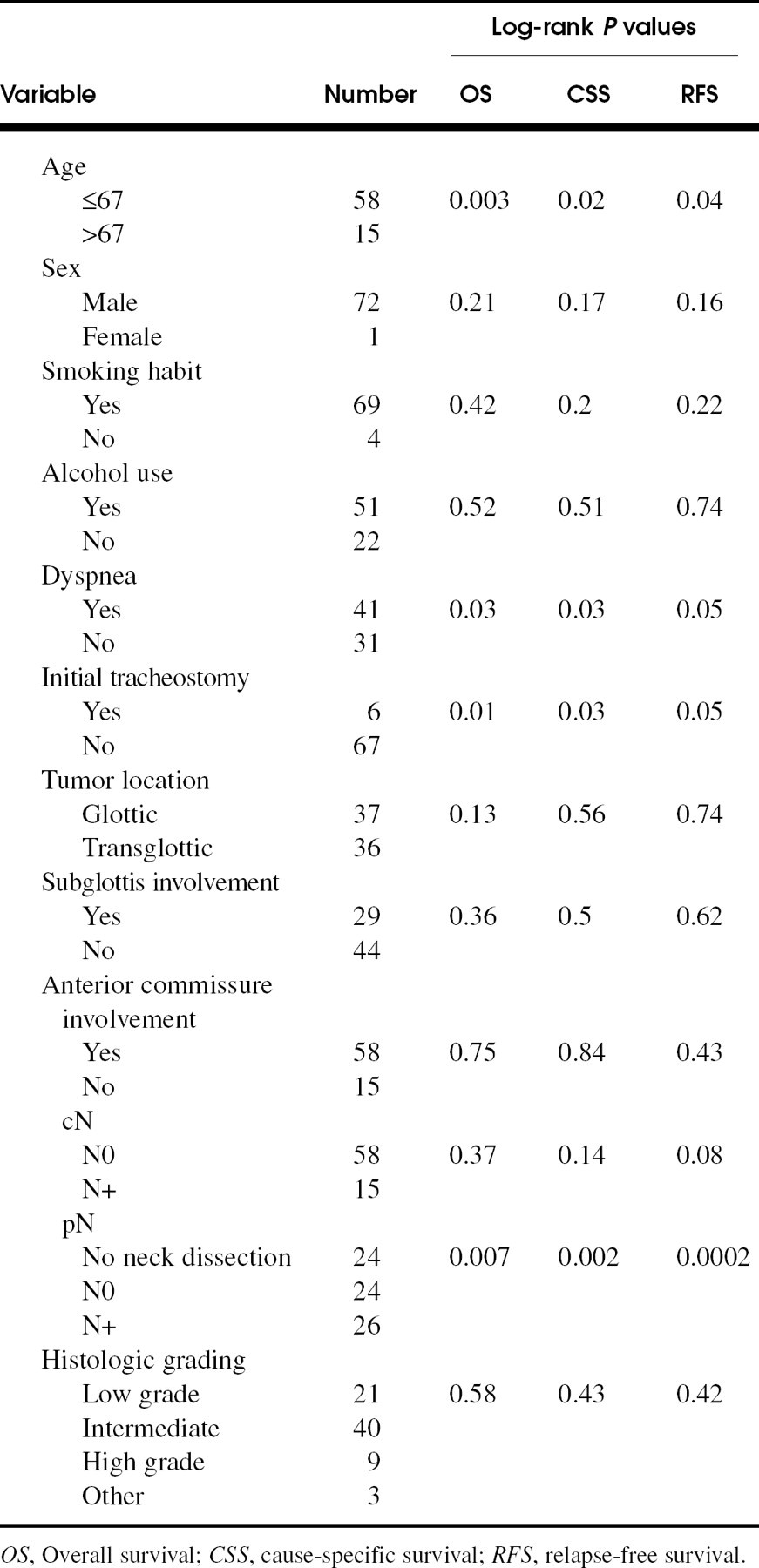
OS, Overall survival; CSS, cause-specific survival; RFS, relapse-free survival.
Survival rates in T3 glottic tumor series
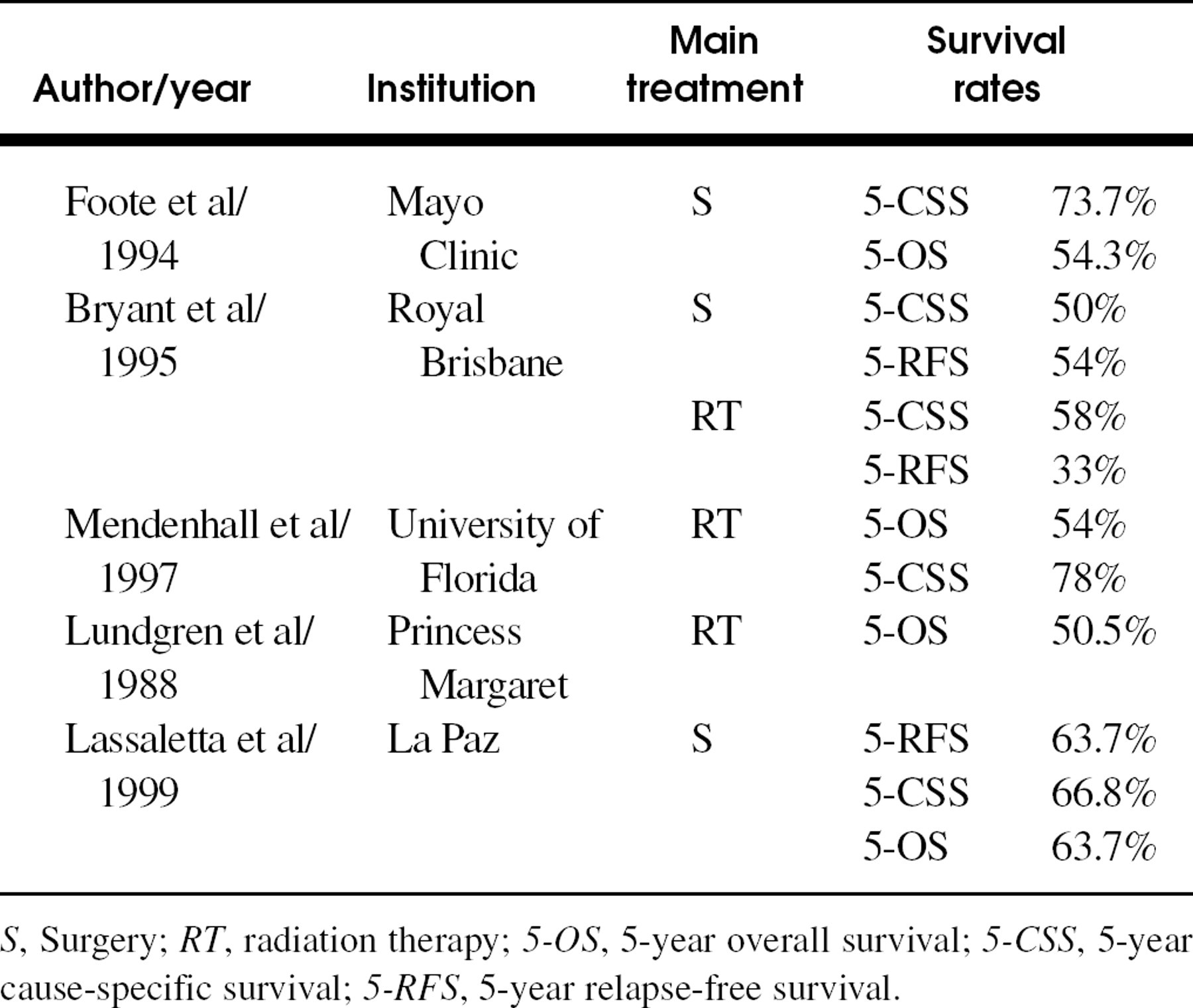
S, Surgery; RT, radiation therapy; 5-OS, 5-year overall survival; 5-CSS, 5-year cause-specific survival; 5-RFS, 5-year relapse-free survival.
According to the initial description of the tumor at the time of diagnosis, 36 tumors were classified as transglottic, and 37 as glottic. Patients with transglottic tumors had a higher incidence of palpable neck nodes (n = 12; 33%) compared with those with pure glottic tumors (n = 3; 8%). This trend had a pathologic confirmation, with higher rates of positive nodes in the transglottic group (58% vs 42%). This difference did not reach statistical significance.
Of the 35 patients who were clinically N0 and underwent neck dissection, the pathologic findings in 14 cases were positive. Of these 14 patients, 7 had transglottic and 7 had pure glottic tumors. The incidence of local recurrence (14% vs 19%), neck recurrence (8% vs 11%), and distant metastases (11% vs 8%) was similar in transglottic and glottic tumors. Stomal recurrence was less frequent in the transglottic group (2.7%) than in patients with pure glottic tumors (8%). When comparing survival and relapse rates between transglottic and glottic tumors, no significant difference was found. Patients with transglottic tumors had slightly higher cause-specific survival rates (median, 111 months) when compared with patients with pure glottic tumors (median, 76 months).
DISCUSSION
One of the most controversial aspects regarding laryngeal cancer is selection of the most appropriate treatment for T3 glottic tumors. Various approaches including different combinations of surgery and radiation therapy have been proposed. Selection of treatment modality depends on several factors, but mainly on the experience of each institution. Recently, there has been widespread investigation of the role of neoadjuvant chemotherapy in controlled randomized studies. A number of chemotherapy regimens have produced high objective response rates, but no definitive improvement in survival has been demonstrated. 6 Surgery is generally accepted as an effective treatment for T3 glottic tumors. Surgical techniques include various options including total, near-total, and partial laryngectomy, either combined or not combined with neck dissection. Unfortunately, a permanent stoma is required in many cases to achieve oncologic safety. 11 Radiation therapy either associated with surgery or not is another therapeutic option for these tumors. Some studies show similar rates of survival in patients treated with radical radiation therapy with salvage surgery when compared with those treated with surgery with or without postoperative radiotherapy. 4,12
In our experience, surgery, usually total or near-total laryngectomy, with postoperative radiation therapy in selected cases, is the best initial treatment for T3 glottic tumors. In recent years, near-total laryngectomy is being performed more frequently in our institution. Less aggressive techniques as extended hemilaryngectomy 13 or supracricoid laryngectomy 14 may play a role in the treatment of T3 tumors, but patient selection is critical in these cases. Transoral laser excision for T3 glottic tumors may prove to be another therapeutic option, 15 but larger series are needed to assess its oncologic safety.
In our study, the choice of performing a dissection in a neck that has been found clinically negative, and its extent, was decided individually by the surgeon, according to finding of neck nodes at the time of surgery, primary tumor location and extension, and the patient's clinical condition and preferences. Nevertheless, as a general rule, we believe that (1) the overall incidence of neck metastases, especially the high incidence of occult positive nodes; (2) the clinical difficulty of distinguishing between T3 glottic, supraglottic, and transglottic tumors by clinical and even surgical exploration; and (3) the frequent possibility of understaging these lesions support the convenience of performing a functional neck dissection in every T3 glottic tumor, as long as the medical condition of the patient allows for this technique. Therefore, we do not share the opinion that a neck dissection should not be indicated in T3 pure glottic carcinomas. 10
Table 2 shows survival rates in some important T3 glottic tumor series. Treatment consisted mainly of surgery, radiation therapy, or combinations of both. Although there are some differences in relapse-free survival and cause-specific survival rates among different studies, overall survival rates are similar.
This study reviews the role of several pretreatment factors in predicting overall survival, cancer-specific survival, and relapse-free survival. Age influenced overall survival, cancer-specific survival, and relapse-free survival; patients younger than 67 had better survival probabilities than older patients. Several studies describe age as a prognostic factor for survival in patients with T3 glottic tumors. 7,16 Although it seems to be clear that elderly patients have a poorer survival expectancy, different results stem partly from the variability in the cutoff levels chosen in the studies.
In our study, neck metastasis was a poor prognostic indicator in both univariate and multivariate analysis. This finding has been documented in most series. 2,7,8,17 Conversely, in our series, the presence of palpable lymph nodes did not influence survival, as there were a considerable number of false-negative results. The value of dyspnea at the time of diagnosis and the history of initial tracheostomy as a prognostic factor may be related to stomal recurrences and/or subglottic extension. Other series also show similar results. 7,17 Table 3 shows prognostic factors in some T3 glottic tumors. The presence of nodes with positive pathologic findings appears to be the most striking prognostic factor in most series.
The term transglottic cancer was used in 1961 by McGavran et al 18 to describe those tumors crossing the Morgagni ventricle and involving glottic and supraglottic sites with possible involvement of the subglottis. Since then, several definitions and theories have been postulated about these tumors. As the precise site of origin is not clear—ventricular, glottic, supraglottic—and it can follow several patterns in its development, 19 a simple definition for a transglottic tumor may be “a glottic carcinoma with supraglottic invasion.” 10 This definition excludes supraglottic tumors extending to the glottic region. However, this distinction is often difficult on clinical evaluation, since it is hard to state if the original location of the tumor is glottic or supraglottic.
As aforementioned, we have defined transglottic tumors as those lesions clinically extending to the supraglottis from the glottis, ie, the central mass involving the vocal cord. Considering that in our environment supraglottic tumors occur much more frequently than glottic tumors, we have been very careful to exclude supraglottic tumors with glottic invasion. Because we were searching for valuable clinical information before treatment, we did not include pathologic classification. Furthermore, it has been demonstrated that a significant number of clinical T3 glottic and transglottic tumors are found to be T4 tumors on pathologic evaluation. 20
It has been postulated that transglottic tumors have a higher cervical metastatic rate, thus requiring more aggressive therapy than “pure” glottic tumors. 10 In our study, although patients with transglottic tumors had a higher incidence of nodes with positive clinical and pathologic results, this fact did not entail different cervical recurrence rates or impact in survival rates. Although it appears reasonable to believe that transglottic tumors may have a higher metastatic capability compared with pure glottic tumors, the precise distinction may not be possible until pathologic examination when it would be too late for planning therapy. For all these reasons, we believe that the term transglottic may be considered essentially descriptive, with no substantial implications in prognosis.
Prognostic factors in T3 glottic tumor series
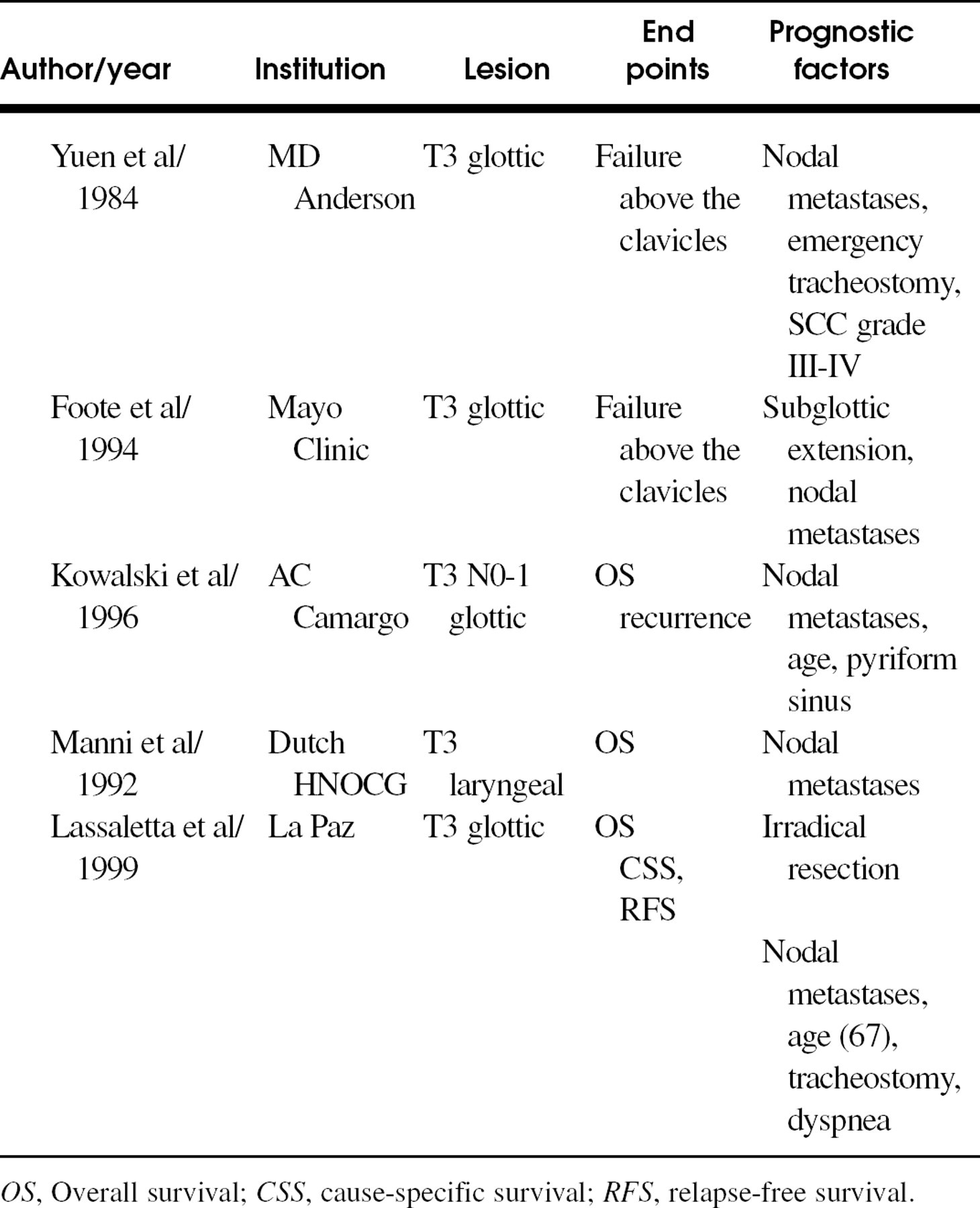
OS, Overall survival; CSS, cause-specific survival; RFS, relapse-free survival.
CONCLUSIONS
Surgery, usually total or near-total laryngectomy associated with neck dissection, and postoperative radiation therapy in selected cases is, in our experience, the best initial treatment for T3 glottic tumors.
Patients over the age of 67, patients with positive neck nodes, and patients with dyspnea, especially those requiring emergency tracheostomy, have worse prognosis.
The term transglottic is mainly descriptive and has little implications in prognosis.