
Abstract

The purpose of this article is to describe a modification of the TEP technique in patients with an esophageal stricture after laryngectomy and radiation. Strictures in these patients may be due to a tight mucosal closure, pharyngocutaneous fistula, and subsequent scarring or radiation. Higher doses of radiation are associated with increased rates of stricture formation.
METHODS
The author's office-based tumor registry was used to review 175 cases of laryngeal cancer. Two patients were subsequently identified undergoing a secondary TEP, which could not be done by conventional means but was accomplished with a modification of a polyvinyl endotracheal tube, first described by Maniglia. 2
CASE REPORTS
Case 1
A 53-year-old black man was treated for a T3N2-cM0, clinical stage IV, squamous cell carcinoma of the pyriform sinus. The patient underwent laryngectomy, bilateral modified neck dissection in July 1999, followed by postoperative radiation therapy (7060 cGy). He underwent a secondary tracheoesophageal puncture approximately 5 months later. The patient noted no dysphagia or difficulty in maintaining his weight. However, at the time of surgery he was found to have a tight esophageal stricture above the tracheal stoma, which precluded visualization with either an adult or pediatric rigid esophagoscope. The patient's esophagus was serially dilated and a No. 8 endotracheal tube was used to perform a successful TEP. Since that time, the patient has had a good voice and has been able to maintain his TEP.
Case 2
A 51-year-old black man was treated with a total laryngectomy for T4N0M0, clinical stage IV, squamous cell carcinoma of his larynx in April of 1997 followed by radiation therapy (6920 cGy). At the time of the secondary TEP in June of 1998 he related no dysphagia or difficulty in maintaining his weight. He, too, was found to have an esophageal stricture. After dilatation, a No. 6 endotracheal tube was used to help perform a TEP. He has maintained effective voicing since that time.
TECHNIQUE
In patients in whom the esophagus is too tight to allow passage of a rigid esophagoscope, an endotracheal tube is used. The endotracheal tube can be sized appropriate to the lumen of the patient's esophagus. A flexible fiberoptic bronchoscope passed through the lumen of the tube allows a concomitant esophagoscopy (Fig 1). A window, 7.5 to 10 mm, is then cut at the junction of middle distal-third of the endotracheal tube (not at its tip as described by Maniglia
2
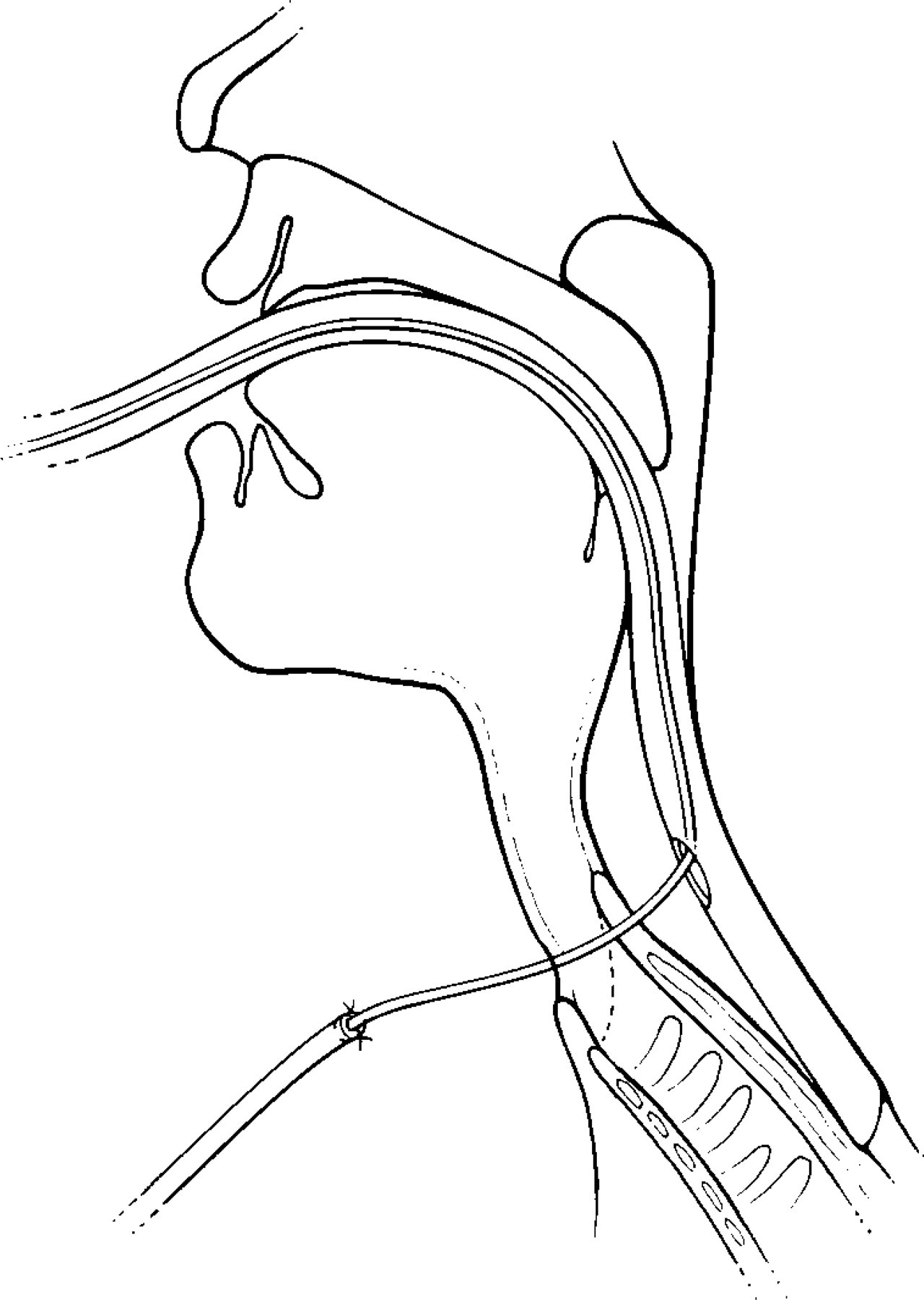
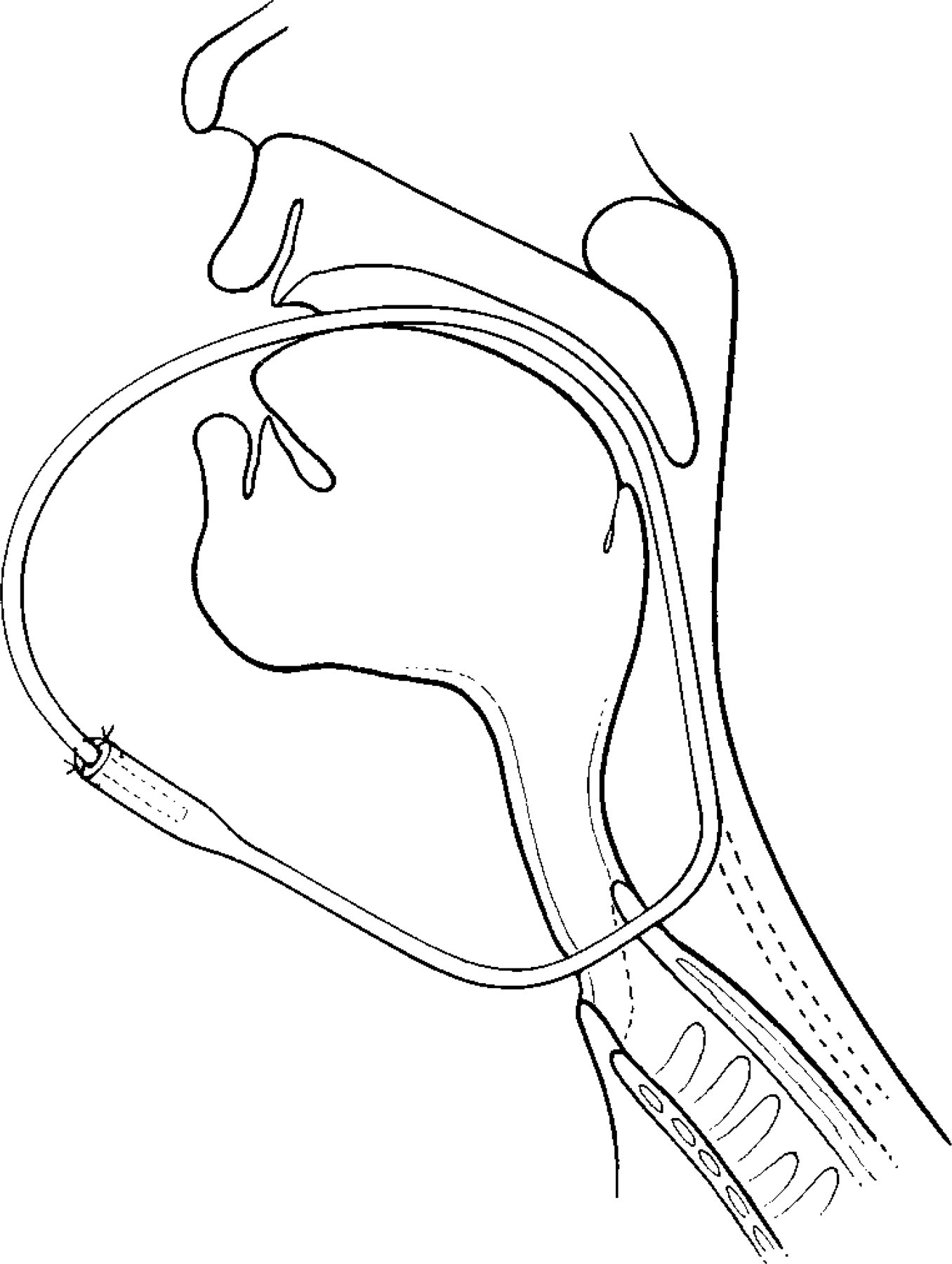
). A No. 14 Intracath (The Deseret Company, Sandy, UT) venous access needle is then inserted through the posterior tracheal stoma and passes into the polyvinyl tube (Fig 2). The needle and catheter system is an Intracath radiopaque catheter. It consists of a 14-gauge needle with an 8-inch long 16-gauge intravenous catheter containing a wire stylet. The catheter is inserted through this needle and passed up the endotracheal tube into the patient's mouth. A small red rubber catheter is sutured to the end of the plastic catheter. The plastic catheter and attached red rubber catheter are then delivered into the oral cavity and the endotracheal tube removed (Fig 3). Ideally, the red rubber catheter can be directed distally down the esophagus but in the 2 cases described, the proximal (from the patient's mouth) and distal ends (from the tracheal
Fiberoptic bronchoscope passed through endotracheal tube allows for visualization of esophageal mucosa. A “window” is cut into endotracheal tube at puncture of its middle and distal thirds. “Window” in endotracheal tube is positioned beneath tracheal stoma. Light from the bronchoscope illuminates the site for tracheoesophageal puncture. Intracath venous needle is directed through posterior tracheal stoma and enters endotracheal tube lumen. If necessary, forceps are passed through bronchoscope and grasp plastic catheter and deliver it into mouth. Plastic catheter is sutured to red rubber catheter, which is then delivered through tracheoesophageal puncture site and into oral cavity.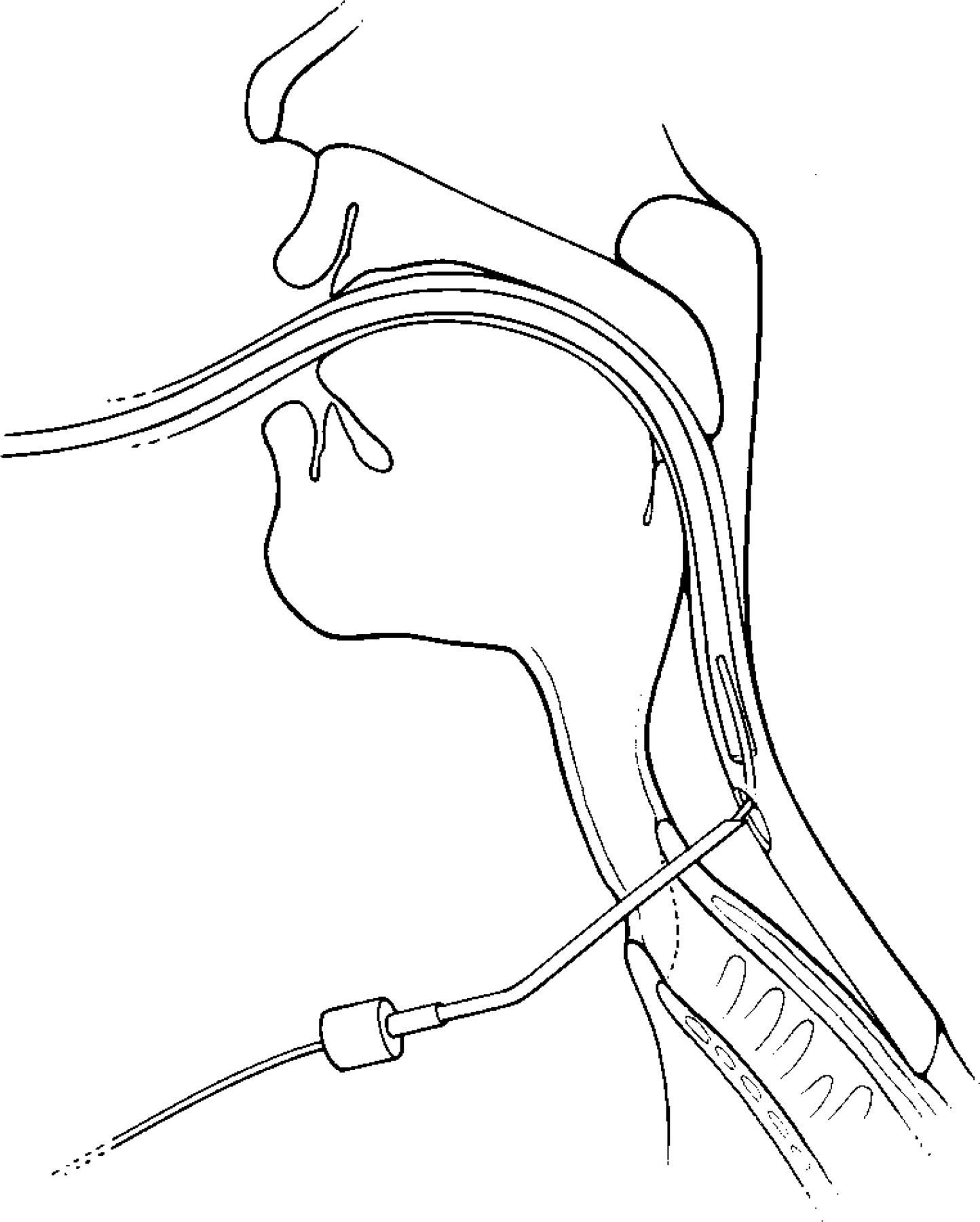
COMMENTS
TEP has become the preferred method of rehabilitating the voice after total laryngectomy. Numerous authors have reported on their success rates with TEP. Representative reports are those of Geraghty et al 3 who reported a 66% success rate. Kao et al 4 reported an 83% success rate in their series of patients undergoing tracheoesophageal puncture.
There have been numerous modifications of the technique as originally described by Singer and Blom. 1 Maniglia 2 first reported the endotracheal tube technique in 1980. The presently described technique differs from that of Maniglia in that the window placed in the endotracheal tube is not placed at the tip of the endotracheal tube. By placing the window further up (proximal) the endotracheal tube, the distal portion of the endotracheal tube actually serves to stent and stabilize the distal esophagus, thereby making insertion of the catheter through the tracheoesophageal puncture site easier. Numerous unique technologic methods have been described in inserting the TEP prosthesis. These include the following: a specially modified Yankeur suction tip, pacemaker introduction kits with a urologic stylet, use of the argon laser, and visualization with a fiberoptic gastroscope. 2 In a separate case report, Mohr et al 5 successfully used the endotracheal technique to insert a voice prosthesis in a patient after laryngectomy who had a history of ankylosing spondylitis and kyphosis, who could not adequately flex his neck for a traditional procedure.
Regardless of the technique used, the goal is to be able to successfully insert a catheter and hence a voice prosthesis. The current technique is useful in selected patients with narrow esophageal lumen after laryngectomy and radiation therapy. The advantages of this technique are multiple. The endotracheal tube can be sized to fit the patient's gullet and esophagus. Passing the endotracheal tube with a bronchoscope contained within it can allow for an endoscopic examination of the mucosa of the gullet and esophagus. By passing the endotracheal tube distal to the site of TEP, the esophagus is stabilized and makes the puncture easier. The window can be placed at any place in the endotracheal tube (I used the junction of the distal and middle-third of the endotracheal tube). The window in the endotracheal tube can be made any size desired.
SUMMARY
In selected patients with strictures or other anatomic deformity precluding the standard method of TEP, this method can be used. It is a modification of the endotracheal tube technique as originally described by Maniglia. It is modified in that the window is placed higher up (proximal) on the endotracheal tube and thus allows the distal end of the endotracheal tube to stabilize the esophagus. The procedure is short and uses equipment readily found in the operating suite. Its use is recommended in selected patients.