
Abstract
OBJECTIVES: To examine hearing results, extrusion rates, and factors likely to affect outcome in patients who underwent ossicular chain reconstruction with Plasti-Pore and hydroxylapatite total ossicular replacement prostheses (TORPs) and partial ossicular replacement prosthesis (PORPs).
STUDY DESIGN AND SETTING: Retrospective chart review was used. Subjects were 1210 consecutive tympanoplasties with or without mastoidectomy that involved ossicular reconstruction with TORPs (n = 560) or PORPs (n = 650) performed in a tertiary referral neurotologic private practice. Only 20% of the cases were primary surgeries, with the majority planned second stage or revision procedures.
RESULTS: Average last postoperative air-bone gap (ABG) was 19.2 dB with closure of the ABG to within 20 dB in 62.9%. Hearing results were better for cases who had not had previous surgery, in those with a diagnosis other than chronic otitis media, when a cartilage graft was used, and for Plasti-Pore rather than hydroxylapatite. Extrusion was known to occur in 4%.
CONCLUSION: After more than 25 years of use in our clinic, Plasti-Pore ossicular replacement pros-theses continue to provide reliable hearing results with a low rate of extrusion.
Plasti-Pore (Smith and Nephews, Inc, Memphis, TN) is a high-density polyethylene sponge that is well tolerated in the middle ear. It is rigid and can be tooled in a variety of shapes. At House Ear Clinic, we have been using the total ossicular replacement prosthesis (TORP) and partial ossicular replacement prosthesis (PORP) for hearing reconstruction since mid-1976, with substantial hearing improvement. 1 We have always favored placing cartilage between the platform of the Plasti-Pore prosthesis and the tympanic membrane or tympanic membrane graft.
Hydroxylapatite is a polycrystalline calcium phosphate ceramic whose elemental constituents closely resemble those of the mineral matrix of human bone. It has a high degree of biocompatibility and it is said that it can be used against the tympanic membrane or tympanic membrane graft without the need for cartilage interposition. More recently, several members of our group have used hydroxylapatite (primarily Medical Universal hydroxylapatite prostheses, Smith and Nephews, Inc) to reconstruct the middle ear, but some discontinued its use based on experience.
Thus we continue to use the same prostheses (Plasti-Pore) that have served us well for many years. However, because there are now a wide variety of newer prostheses that use new materials, we believed it was important to review our experience of the last decade with more than 1200 cases of ossicular reconstruction, including our more recent experience with hydroxylapatite. We determined the incidence of extrusion and the hearing results and examined factors that are likely to influence outcome. The large number of patients allows us to present outcomes for subgroups of patients having various combinations of pathologic conditions and procedures. The rates of successful hearing results and extrusion in these subgroups can, we believe, serve as a useful guideline to clinicians for counseling patients regarding expected outcome.
METHODS AND MATERIALS
Of 3173 patients who underwent tympanoplasty with or without mastoidectomy at House Ear Clinic between 1990 and 1998, inclusive, 1210 had ossicular reconstruction with a Plasti-Pore or hydroxylapatite TORP or PORP. These are the subjects of the study. Their ages ranged from 4 to 87 years, with a mean of 39.8 years (SD = 19.8). Two hundred forty-two (20%) patients were under 18 years old at the time of surgery. The cases were equally distributed between the right (52%) and left (48%) sides. PORPs were used in 650 cases (53.7%) and TORPs in 560 cases (46.3%). Other patient characteristics are shown in Table 1. Less than 20% of the cases were primary procedures, with the majority either planned second-stage operations or revisions. Chronic otitis media was the principal diagnosis in 92% of the cases. Sixty-five percent of cases underwent tympanoplasty without mastoidectomy and 27.5% underwent tympanoplasty with intact canal wall (ICW) mastoidectomy.
Characteristics of 1210 patients undergoing ossicular reconstruction surgery with a PORP or TORP
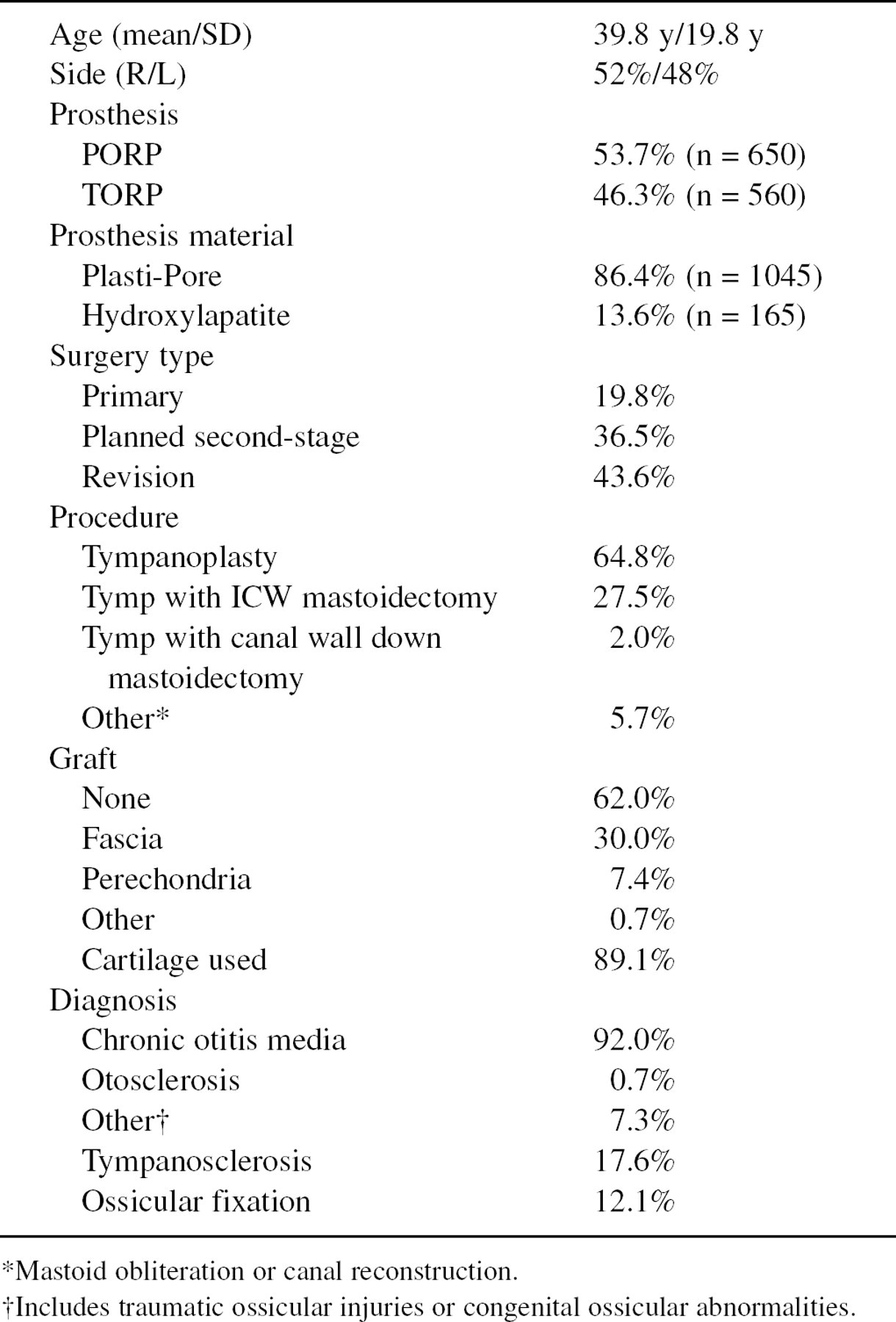
Mastoid obliteration or canal reconstruction.
Includes traumatic ossicular injuries or congenital ossicular abnormalities.
Ossiculoplasty of the middle ear ossicular chain was performed on each patient by using either a total (TORP) or partial (PORP) Plasti-Pore (n = 1045) or hydroxylapatite (n = 165) ossicular replacement prosthesis, depending on the surgeon's preference. The TORP was used when the incus and stapes or stapes superstructures were absent. The prosthesis was placed between the stapes footplate or oval window graft and the tympanic membrane. The PORP was used when the incus was absent or diseased, but the stapes was present and mobile. The prosthesis was placed between the stapes superstructure and the tympanic membrane when an intact stapes was encountered. Tragal cartilage was interposed between the drum and the prosthesis in 89.1% of cases, including nearly all of the Plasti-Pore cases. No cartilage was used in 10.9% of cases, primarily in those receiving a hydroxylapatite prosthesis.
Selected data from each patient who underwent surgery were entered on a data-collection sheet designed for the study. Information was obtained from the patient's preoperative record, operative note, audiograms, and postoperative office visits. All patients underwent audiometric testing before surgery and were typically seen approximately 3 months after surgery for a full audiometric follow-up, with many returning again later. The mean time to last audiologic follow-up was 19.9 months (median = 10.9 months), ranging from 2 weeks to 9.5 years. Of the 1210 cases, 665 (55.0%) had audiologic data available from a follow-up of at least 1 year and 30.9% were tested at 2 years or more after surgery. An additional 56 patients returned for an office visit at 1 year or later although complete audiologic testing was not performed.
Data analysis
Pure-tone air and bone-conduction thresholds were obtained before and after surgery. Air- and bone-conduction thresholds at 500, 1000, 2000, and 3000 Hz were used to calculate the pure-tone averages (PTAs). If 3000 Hz was not tested, 4000 Hz was substituted in calculation of the PTA. Air and bone from the same test were used to calculate the air-bone gap (ABG). For the 3-month postoperative visit only, when bone-conduction thresholds were not available, preoperative bone thresholds were used instead to calculate the ABG. This was done after a paired-comparison analysis of data from those patients having both preoperative and 3-month postoperative bone-conduction data showed no statistically significant changes from before to after surgery. For later follow-ups, when bone thresholds were not available, earlier postoperative bone thresholds were used. Results are reported in compliance with the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) Committee on Hearing and Equilibrium guidelines for evaluation of the results of treatment of conductive hearing loss. 2 A successful hearing result was defined as a postoperative ABG of 20 dB or less.
Descriptive and inferential statistical analyses were performed by using parametric and nonparametric statistics, as appropriate. For continuous variables, independent groups were compared by using the t test whereas paired-comparisons were made by using the paired t test. Relationships between categorical variables were assessed with chi-squared analyses. Criterion for statistical significance was set at P ≤ 0.05, two-tailed.
The AAO-HNS guidelines for reporting results suggest using audiometric testing done 1 year or more after surgery. membrane. The PORP was used when the incus was absent or diseased, but the stapes was present and mobile. The prosthesis was placed between the stapes superstructure and the tympanic membrane when an intact stapes was encountered.
Mean (SD) air PTA (500, 1k, 2k, 3k) and ABG

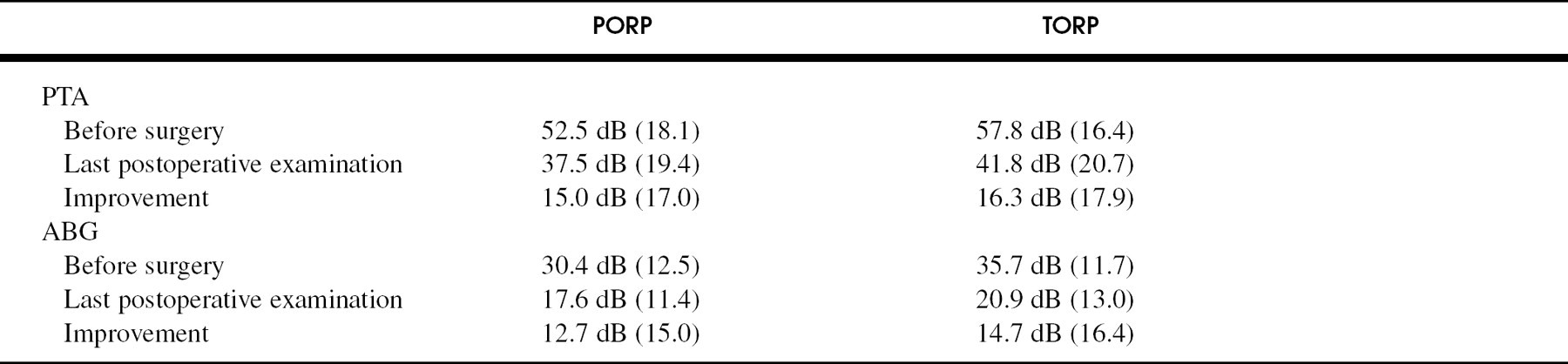
Mean (SD) hearing results by type of prosthesis
RESULTS
The overall hearing results are shown in Table 2. PTA and ABG are shown for the preoperative, 3-month postoperative, ≥1 year postoperative, and last available follow-up periods. PTA improved from a preoperative average of 54.9 dB to 38.3 dB at 3 months after surgery, remaining relatively stable at last follow-up. There were no dead ears (air PTA ≥120 dB and bone conduction equal to 80 dB) after surgery. The mean postoperative ABG was 19.2 dB at 3 months and 19.2 dB at most recent visit. The mean improvement in the ABG from preoperative to last postoperative period was 13.6 dB improvement (SD = 15.7 dB). Success rate (ABG ≤20 dB) was 60.4% at 3 months after surgery and 57.6% in cases with a last hearing test at 1 year or more after surgery. Overall success rate based on last test available was 62.9%. Of the 741 cases who had an intact tympanic membrane and did not require grafting, 460 (62.1%) had a postoperative ABG of 20 dB or less.
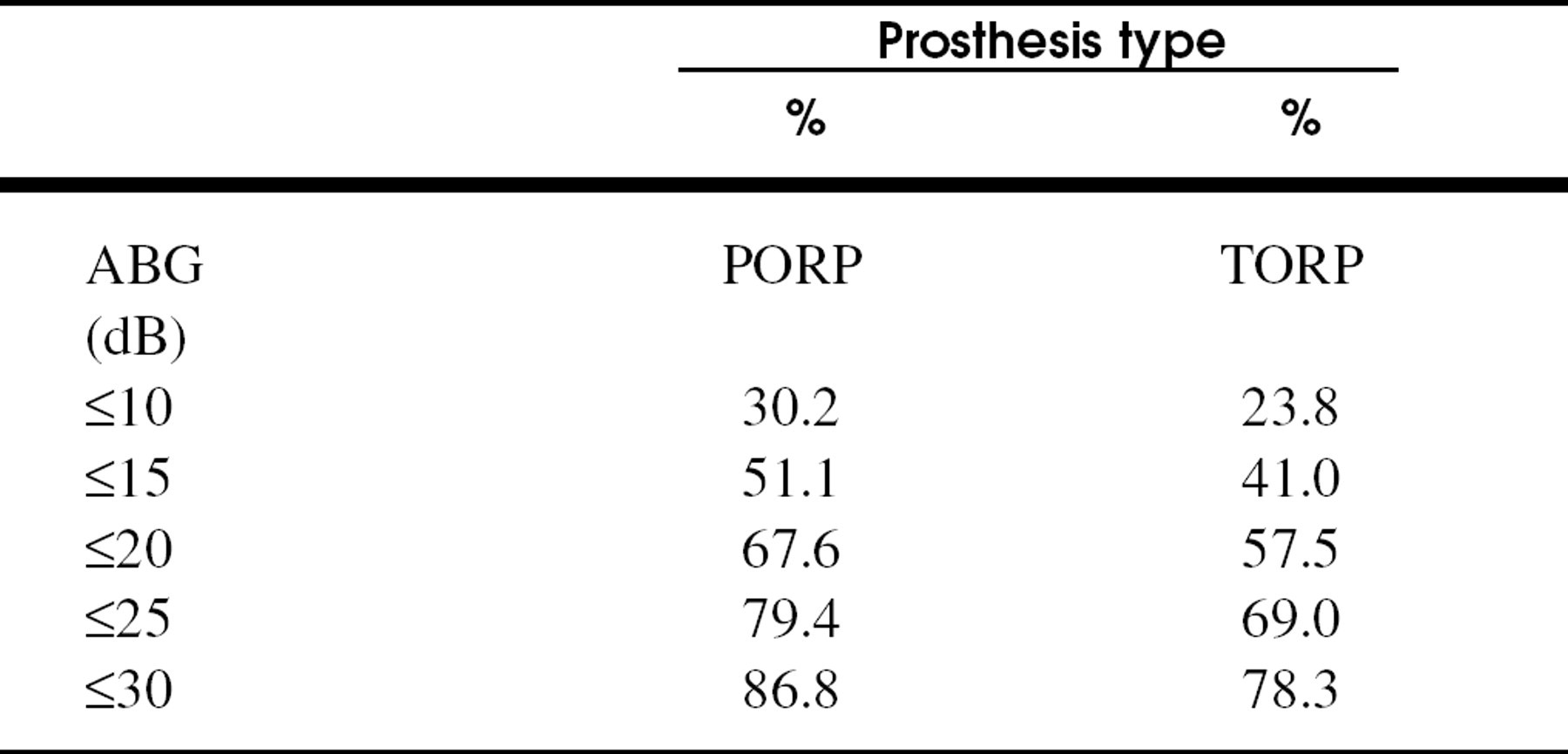
Last postoperative ABG in 5 dB cumulative steps, by prosthesis type
Hearing was stable over the length of follow-up. As already noted, there was no significant change in ABG for those with both 3-month and a later follow-up, and 85.2% of the cases had a change of 15 dB or less from 3 months to last follow-up; 5.0% got better by more than 15 dB and only 9.8% got worse by more than 15 dB. The 3-month ABGs of those who also had later follow-up (n = 667) were compared with the gaps of those who did not have longer-term follow-up (n = 416). Successful closure of the ABG to ≤20 dB 3 months after surgery occurred in 68.5% of those with no long-term follow-up and 55.3% of those who did return later, with mean ABGs of 17.5 dB and 20.2 dB, respectively (P ≤ 0.001). Although this is not a large difference in mean gap, it is consistent with the hypothesis that those who did return later tended to be patients with poorer initial results.
Extrusion rates by use of cartilage graft and prosthesis material

Factors affecting a successful hearing outcome (ABG ≤20 dB)
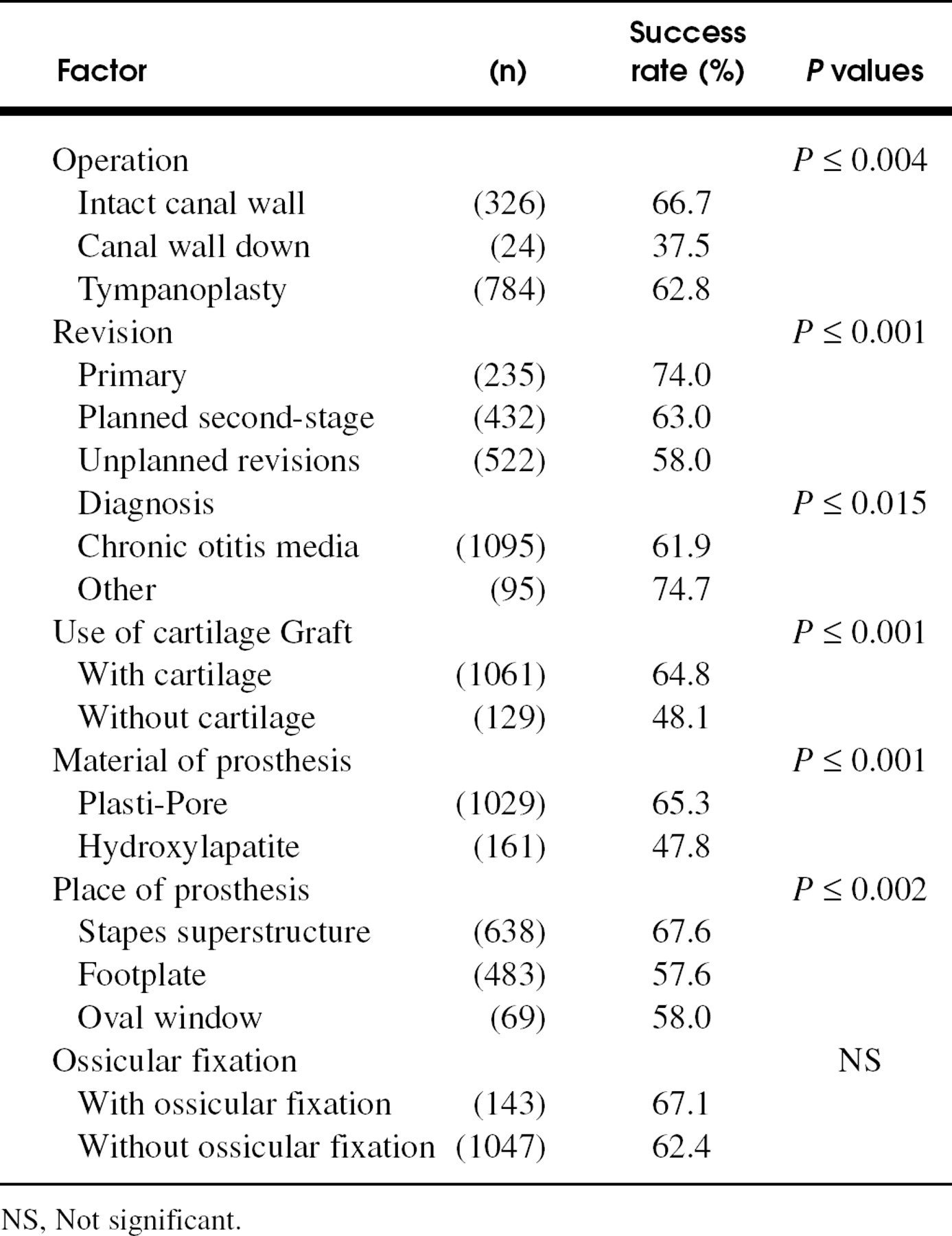
NS, Not significant.
Hearing results by type of prosthesis
Hearing results by type of prosthesis are summarized in Tables 3 and 4. PTA improved by a mean amount of 15.0 dB for PORPs and 16.3 dB for TORPs. The mean amount of change in the ABG from preoperative to last follow-up visit was 12.7 dB (SD = 15.0 dB) for PORPs and 14.7 dB (SD = 16.4 dB) for TORPs. Closure of the ABG to within 20 dB or less occurred in 67.6% of cases reconstructed with a PORP and 57.5% of those reconstructed with a TORP (P ≤ 0.001).
Extrusion and complications
Prosthesis extrusion was known to have occurred in 4% (49) of the 1210 cases. The average time for extrusion to occur in the 47 cases in which extrusion date was known was 2.3 years (range 0.26 to 7.4 years; SD = 1.5 years), with most (82.9%) of the extrusions occurring after at least 1 year and 47% occurring after at least 2 years. Because not all patients returned for follow-up, a probable „worst-case“ prevalence of extrusion was estimated based on an assumption that the prevalence of extrusion after one year would be the same in those not returning for follow-up as in those who did so. This is considered „worst-case“ because our experience suggests that if not all, certainly a large percentage, of patients having problems will return to the doctor or clinic where their treatment occurred. There were 39 extrusions at ≥1 year after surgery with 721 patients having returned for follow-up in the same time period (ie, ≥1 year after surgery). This yields a prevalence of 5.4% at 1 year or more, for an additional 26 cases of extrusion estimated as possible among the 489 who did not return. Thus, an estimated „worst-case“ prevalence of extrusion would be 75 (49 + 26) of 1210, or 6.2%.
Of the 49 cases with prosthesis extrusion, 18 had retraction of the tympanic membrane before the extrusion occurred.
Table 5 provides the extrusion rate by placement of cartilage between the drum and the prosthesis and by material. For the 1040 Plasti-Pore prostheses cases used in conjunction with cartilage, extrusion of the prosthesis occurred in 38 (3.7%) of the cases. Extrusion of the prosthesis occurred in 10 (7.9%) of the 127 cases with hydroxylapatite prostheses when cartilage was not used. However, there were no extrusions in the 38 hydroxylapatite cases in which cartilage was used. Overall, there was no statistically significant difference between the Plasti-Pore and hydroxylapatite groups in rates of extrusion, but the difference between use of cartilage and no cartilage approached significance (P < 0.056).
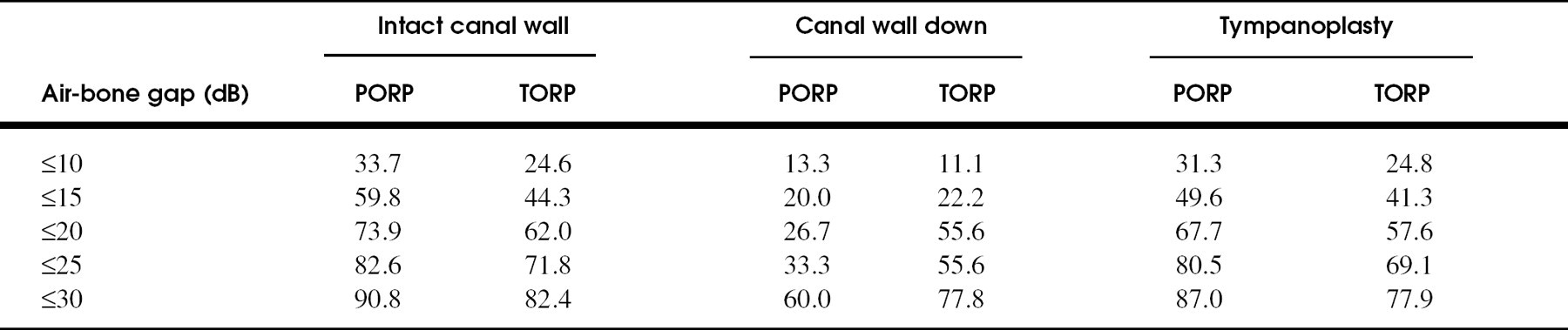
Air-bone gap in 5 dB cumulative steps by prosthesis and operation
Recurrent or residual cholesteatoma, middle ear fluid level, and perforation of the tympanic membrane were considered complications. Nine (0.7%) patients had residual cholesteatoma develop and 5 (0.4%) had recurrent cholesteatoma and required revision surgery. Eighteen (1.5%) patients had aeration failures requiring ventilation tubes and 36 (3%) had postoperative perforation of the tympanic membrane.
A high frequency (1, 2, 4 kHz) bone conduction PTA was computed to assess sensorineural hearing loss as a complication. The preoperative PTA was compared with the 3-month postoperative PTA. The postoperative PTA was within 10 dB of preoperative in 93.6% of patients, with 0.8% worse by more than 10 dB and only 1 patient (0.1%) worse by more than 20 dB. There were no dead ears. The mean change was 1.8 dB (SD = 5.7 dB).
Factors affecting outcome
A variety of factors were evaluated to determine whether they were related to a successful hearing outcome (Table 6). The associations between success rate and type of surgery, diagnosis, use of cartilage, type of material, and place of prosthesis were statistically significant. The success rate was lower in canal wall down procedures and higher in primary ears than those previously operated. Patients with otosclerosis, congenital ossicular abnormalities, ossicular fixations, and traumatic ossicular injuries were grouped as other diagnosis. These patients had a significantly higher success rate when compared with those with chronic otitis media. Cartilage and type of material are confounded by the fact that nearly all the Plasti-Pore cases had cartilage whereas most of the hydroxylapatite did not. However, further analysis showed no difference in success rate between hydroxylapatite with and without cartilage.
Table 7 shows the prosthesis and operation-specific hearing results. In intact canal wall operations, a closure of the ABG to within 20 dB was seen in 62.0% and 73.9% for TORPs and PORPs, respectively. In tympanoplasties without mastoidectomy, the difference between TORPs and PORPs was roughly the same. Results were poorest in the small number of canal wall down cases.
Hearing result by type of prosthesis and material
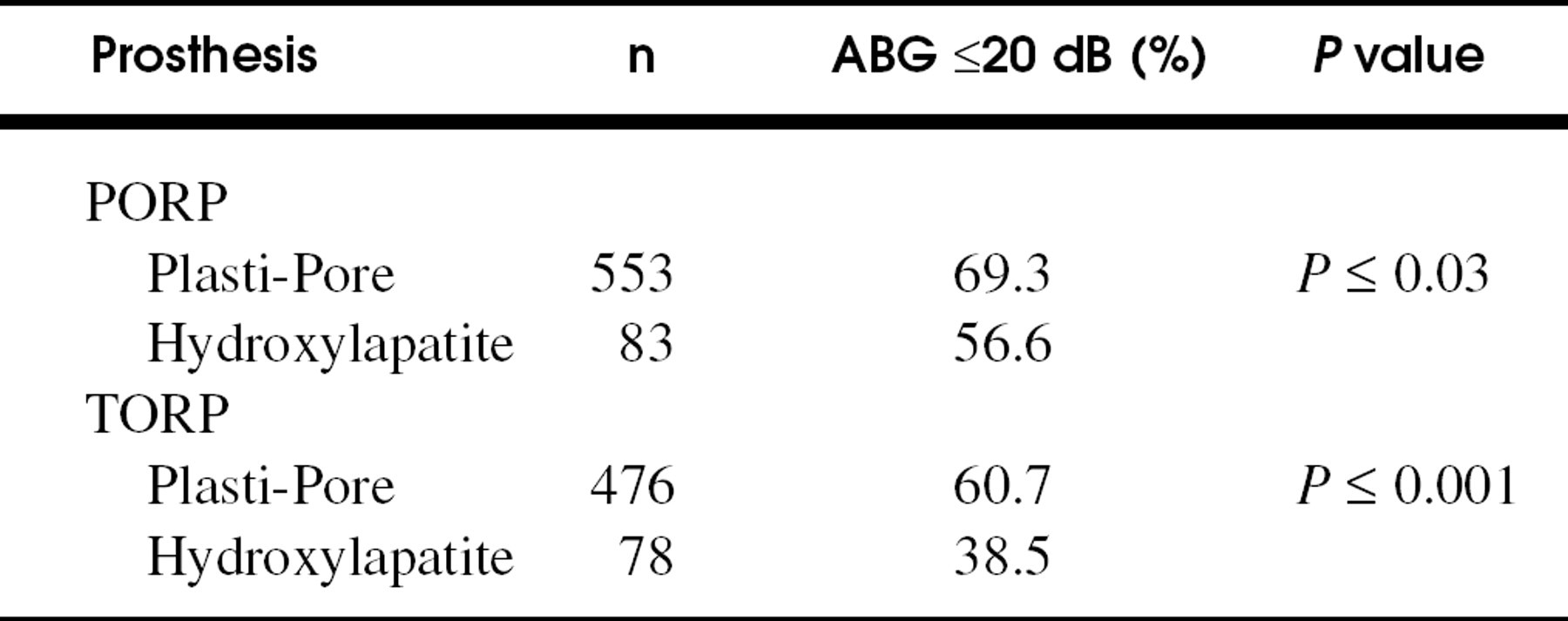
Table 8 shows the postoperative success rate for type of prosthesis and material. There was a statistically significant difference in success rate with the Plasti-Pore PORP group having the highest success rate. The difference between Plasti-Pore and hydroxylapatite results appeared both for PORPs (P = 0.024) and TORPs (P < 0.001).
Finally, we summarize hearing success and extrusion rates by disease, prosthesis type, and type of surgical procedure in Figure 1. Although some categories contain few or no patients, these results can serve as a guideline for counseling individual patients regarding probability of a „good“ hearing result and likelihood of extrusion.
DISCUSSION
We evaluated extrusion rates and hearing results with PORPs and TORPs in 1210 cases. Because we have been using Plasti-Pore prostheses for nearly 25 years, we wanted to take an updated look at the results and at factors that may be involved in a successful outcome. In addition, we recently have used hydroxylapatite prostheses and evaluated results with these newer prostheses as well.
The overall success rate was 62.9% at last postoperative visit, with an overall known extrusion rate of 4% and a „worst case“ estimate of 6.2%. The Plasti-Pore PORP and TORP groups had success rates of 69.3% and 60.7%, with extrusion rates of 2.5% and 5.2%, respectively. These outcomes remain similar to those we have previously reported. 1,2 The hydroxylapatite PORP and TORP groups had success rates of 56.6% and 38.5% and extrusion rates of 7.1% and 5%, respectively. Patients who underwent a primary procedure and cases in which a cartilage graft was used had higher success rates.
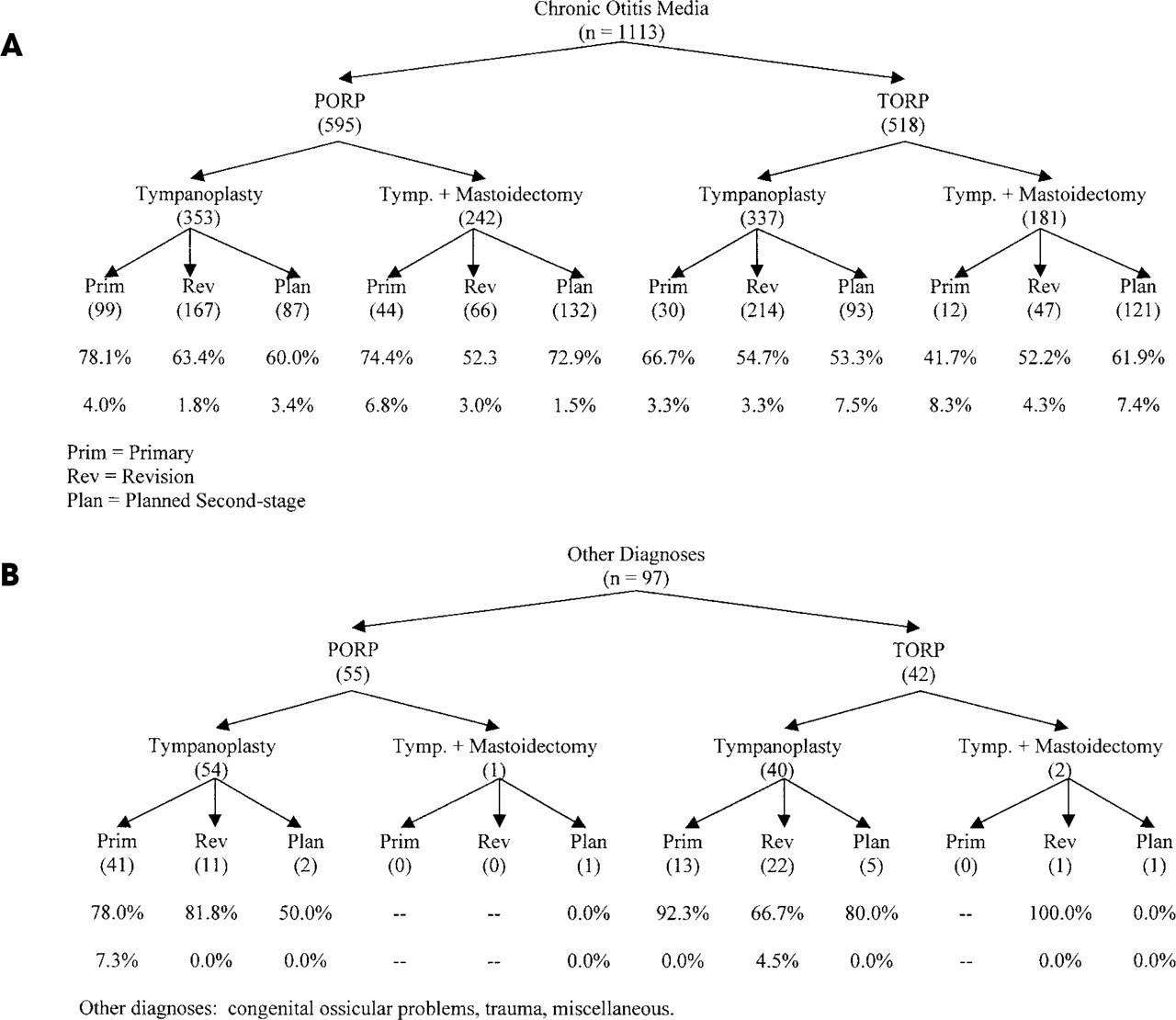
Rates of successful closure of the ABG (≤20 dB) at last follow-up and known prevalence of extrusion for various subgroups of patients. Number of subjects operated in each subgroup is shown in parentheses. Eight subjects did not have audiologic data available.
Although the AAO-HNS guidelines suggest an audiometric follow-up of 1 year or more, we found no significant difference in 3-month and later audiometric data, for those having both. Thus, we feel that the 3-month data are representative when later follow-up is not available. In addition, given the nature of our practice, longer-term follow-up is biased toward patients with poorer results. We cannot know the true extrusion rate without long-term follow-up on all 1210 patients. However, a „worst-case“ estimate of 6.2% was made based on assuming the same rate among those who did not return as among those who did. In practice, although some patients may have gone elsewhere with an extrusion, the majority who did not return probably did not have extrusion. Thus, we believe that the „true“ rate of extrusion is probably closer to the 4% rate of known extrusions.
The present study defined success as a postoperative ABG of 20 dB or less. Hearing results with hydroxylapatite and Plasti-Pore PORPs and TORPs obtained by other investigators have ranged from 43% to 76% for PORPs and from 27.3% to 69% for TORPs. 1,3-7 Our present results compare favorably with these. We do note some differences in extrusion rates. In our study, the overall extrusion rates for the Plasti-Pore group and hydroxylapatite groups were 3.6% and 6.1%, respectively. Goldenberg, however, had lower extrusion rates with hydroxylapatite prostheses than with Plasti-Pore prostheses. 8 The fact that our results with hydroxylapatite did not appear to be as good as those with Plasti-Pore led us to a closer examination of our cases, the result of which suggests that this was not due to the material but to the lack of cartilage. No extrusions occurred among the hydroxylapatite group in which cartilage was used. We have used primarily hybrid hydroxylapatite prostheses with a hydroxylapatite cap and a Plasti-Pore shaft. We believe that the problem with these prostheses may lie in the design, making the cap somehow separate from the shaft after surgery and no longer ensuring good contact and tension with the tympanic membrane. This would explain our poorer hearing success rate with hydroxylapatite. Although some members of our group have discontinued use of hydroxylapatite because of these poorer results, we believe that future modifications may help to improve the design and, therefore, the results that might be obtained.
In our hands, Plasti-Pore still provides good results when compared with other newer prostheses. It has some advantages: it is readily available, is easy to trim and shape to the desired configuration intraoperatively without special instrumentation, and has proved itself over the years for use in the middle ear. High-density polyethylene has sufficient porosity to encourage tissue in-growth that forms an interlacing network of fibrous connective tissue around the prosthesis and eventually fixes it to the footplate or stapes. 9,10 Multinucleated foreign body cells are frequently seen in and around the prosthesis, but it remains unclear what role they may play. 10,11 Plasti-Pore is a biocompatible material in the middle ear, except when it touches the tympanic membrane directly. Therefore, it must be used in conjunction with a human tissue interface (autograft cartilage). Recently, there has been increased effort by some physicians to eliminate the need for human tissue during surgery. We have been using mostly autograft cartilage along with Plasti-Pore prostheses since mid 1976 and have found no inconvenience in this procedure. We have not experienced infection or hematoma from the tragal incision or had any complaints by the patients. When removing tragal cartilage, perichondrium is always saved for later grafting, if needed, which we find to be very convenient. Our results with Plasti-Pore continue to be highly satisfactory, with low extrusion rates and good hearing outcomes. 1,3
The present study contains a large proportion of planned second-stage procedures and revisions. This accurately reflects our usual patient population and the nature of their disease, but does tend to skew the overall results of this study. We reconstruct only highly selected cases with a primary procedure. If conditions are not favorable, we stage the operation to obtain ideal conditions. Those who required more extensive surgery with mastoidectomy had more extensive disease and poorer hearing results. The middle ear space is shallow in the canal wall down situation, which probably accounts for the poorest hearing results in those cases. This and other studies have shown that a number of disease and procedure-related factors may affect results. We provide hearing success rates and extrusion rates for some common combinations of these factors that can be used to counsel patients regarding appropriate expectations.
CONCLUSIONS
We have been using Plasti-Pore prostheses with cartilage interposed between the prosthesis and the tympanic membrane for 25 years. We continue to be satisfied with the reliable hearing results and low extrusion in a variety of ossicular situations and in ears with extensive disease. Until design improvements make the newer prostheses and materials clearly better, we will continue our long-term use of Plasti-Pore.
We want to thank Mark Oppenheimer, MS, for providing the data analyses and Karen I. Berliner, PhD, for helping in the preparation and editing of the manuscript.