
Abstract
OBJECTIVE: The phenomenon of postobstructive pulmonary edema (POPE) has been associated with the relief of upper airway obstruction, which itself is fundamental to the pathophysiology of obstructive sleep apnea (OSA). A review of patients with OSA undergoing tracheotomy was performed to characterize this process.
STUDY DESIGN: Retrospective chart review of study patients with OSA undergoing tracheotomy and of control patients without OSA undergoing tracheotomy for unrelated problems. Chest radiographs were reviewed in a double-blind fashion to score posttracheotomy changes in pulmonary status.
SETTING: Academic tertiary referral center.
RESULTS: Thirty (67%) of 45 OSA patients treated by tracheotomy had evidence of POPE, whereas only 5 (20%) of 25 control group patients had increased pulmonary edema. The remaining 15 (33%) of 45 OSA patients and 20 (80%) of 25 control patients had either no change or an improved pulmonary status. Those with OSA that developed POPE were mostly graded as having mild pulmonary edema (22/30, 73%). Far fewer were graded as having moderate pulmonary edema (6/30, 20%), and fewer still with severe pulmonary edema (2/30, 7%). Two (7%) of 45 patients with severe POPE died of complications related to cor pulmonale in the postoperative period.
CONCLUSION: Results support maintaining a high index of suspicion for the development of postobstructive pulmonary edema in patients treated for OSA. Treatment options, such as positive pressure ventilation and diuresis, and an increased awareness of this condition may help reduce the morbidity and mortality associated with treatment of this disease.
Obstructive sleep apnea (OSA) is a serious medical problem resulting in hypersomnolence, 1 behavioral changes, occupational disability, and cardiopulmonary disease. 2 Serious cardiac dysrhythmias and conduction abnormalities are well recognized. 3 Chronic hypoxemia and respiratory acidosis contribute to the changes that lead to severe pulmonary hypertension and cor pulmonale. Our observation that relief of the chronic upper airway obstruction manifest by OSA patients can sometimes result in a temporary worsening of pulmonary status is the focus of this investigation. It has been previously reported that after the relief of acute airway obstruction, patients are at risk of developing postobstructive pulmonary edema. 4–9 The upper airway obstruction in patients with OSA represents a more chronic physiological condition, but a similar postobstructive pulmonary edema (POPE) has been recognized in our patient population after the relief of upper airway obstruction by tracheotomy. Deterioration after tracheotomy in this group of patients has resulted in increased morbidity and prolonged hospital stays. A review of those patients with severe OSA warranting tracheotomy was undertaken to determine the incidence and severity of radiographic pulmonary edema. The physiologic mechanisms of POPE are postulated and its management reviewed so that recognition of the risk factors associated with POPE may help anticipate its occurrence and guide its management.
MATERIALS AND METHODS
A retrospective chart review was performed on patients with OSA at our institution who underwent tracheotomy as an isolated procedure during a 13-year time period between 1985 and 1998. Patients with comorbidities that would predispose them to pulmonary edema were excluded from the study population. These included renal failure, myocardial infarction, and other hypervolemic states such as sepsis that required fluid resuscitation. Patients were also excluded if chest x-rays (CXRs) in the preoperative and immediate postoperative period were not available. Polysomnography and continuous positive airway pressure (CPAP) data were not collected in the record review. Of 100 medical records reviewed, 45 patients met our criteria. The control group was selected from patients undergoing tracheotomy without a diagnosis of OSA and were matched for age, weight, intravenous fluids and operative duration. Twenty-five patient control charts with complete preoperative and postoperative CXRs were reviewed. As with the study group, patients with comorbidities predisposing them to pulmonary edema were eliminated. The incidence of POPE was not correlated with individual patient demographic data, but rather, demographic data were used to ensure comparability between the study and control groups. Treatment regimens for OSA and preoperative evaluation of OSA by polysomnography were not reviewed.
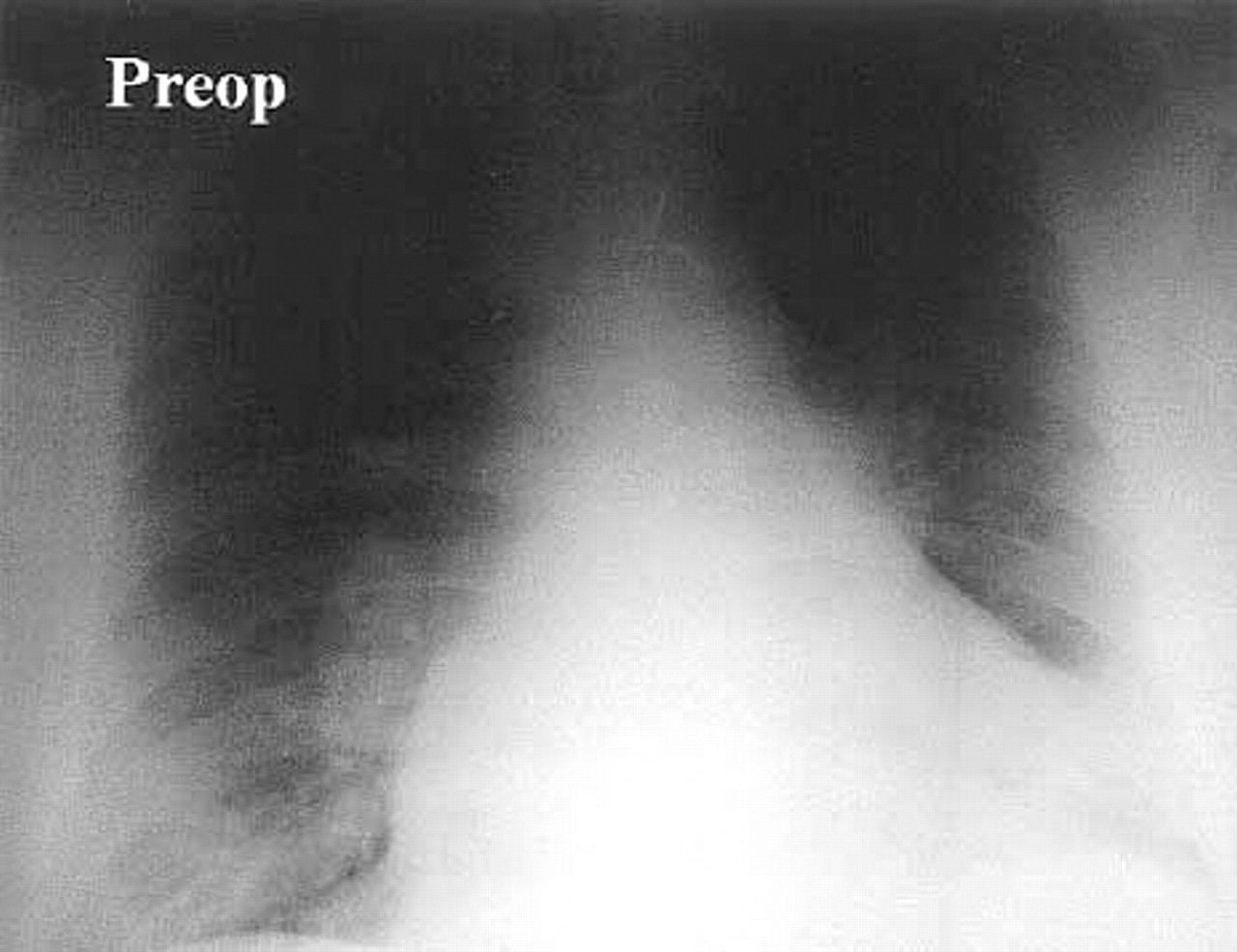
Preoperative PA chest radiograph of a 43-year-old male patient with severe OSA and mild pulmonary edema (score = 3/10) in addition to dilated cardiomyopathy as a result of cor pulmonale.
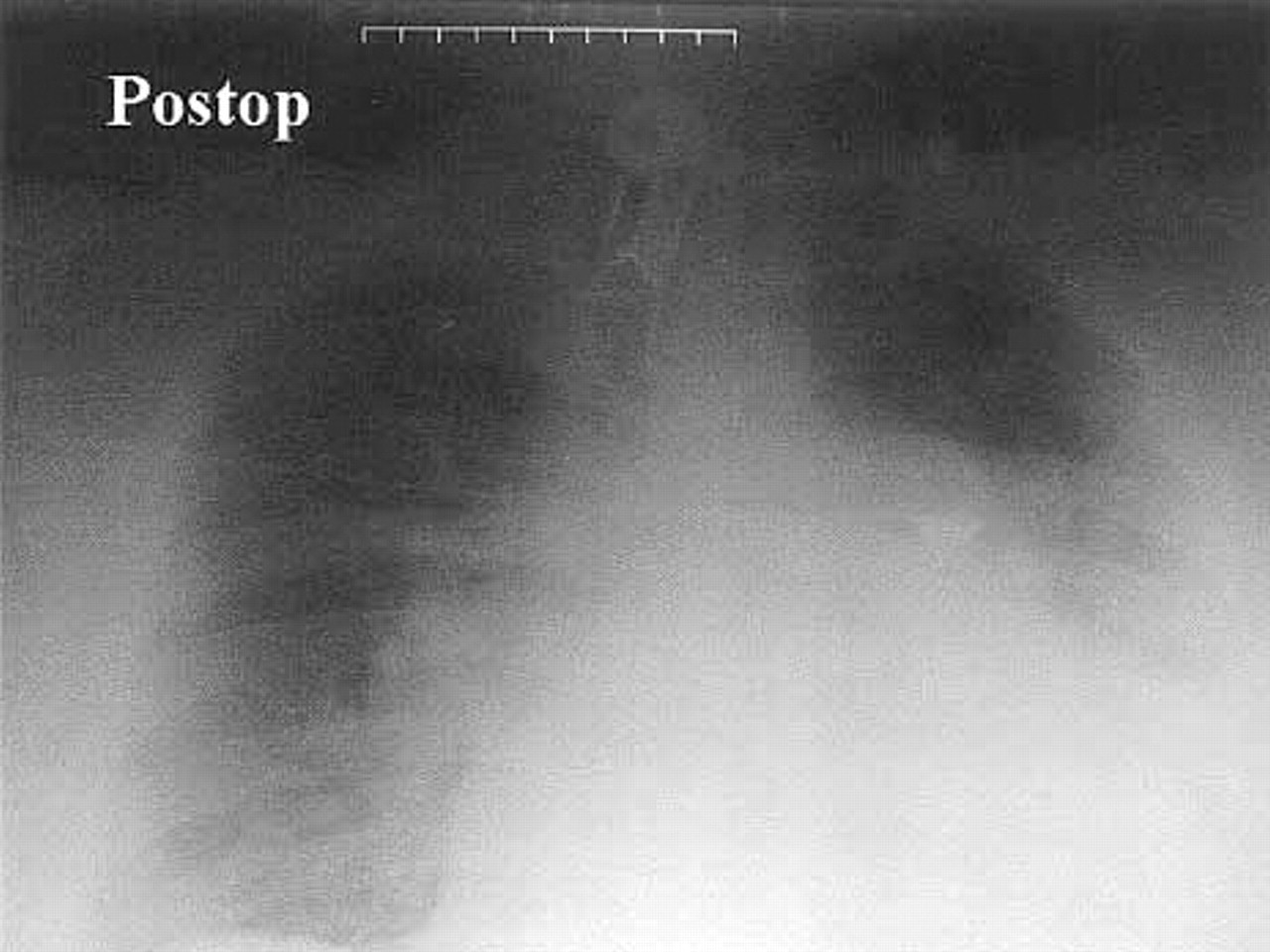
Postoperative AP supine chest radiograph taken of the same patient in Fig 1 24 hours after tracheotomy for severe OSA. Note the increase in pulmonary edema from mild to moderate levels (score = 5/10).
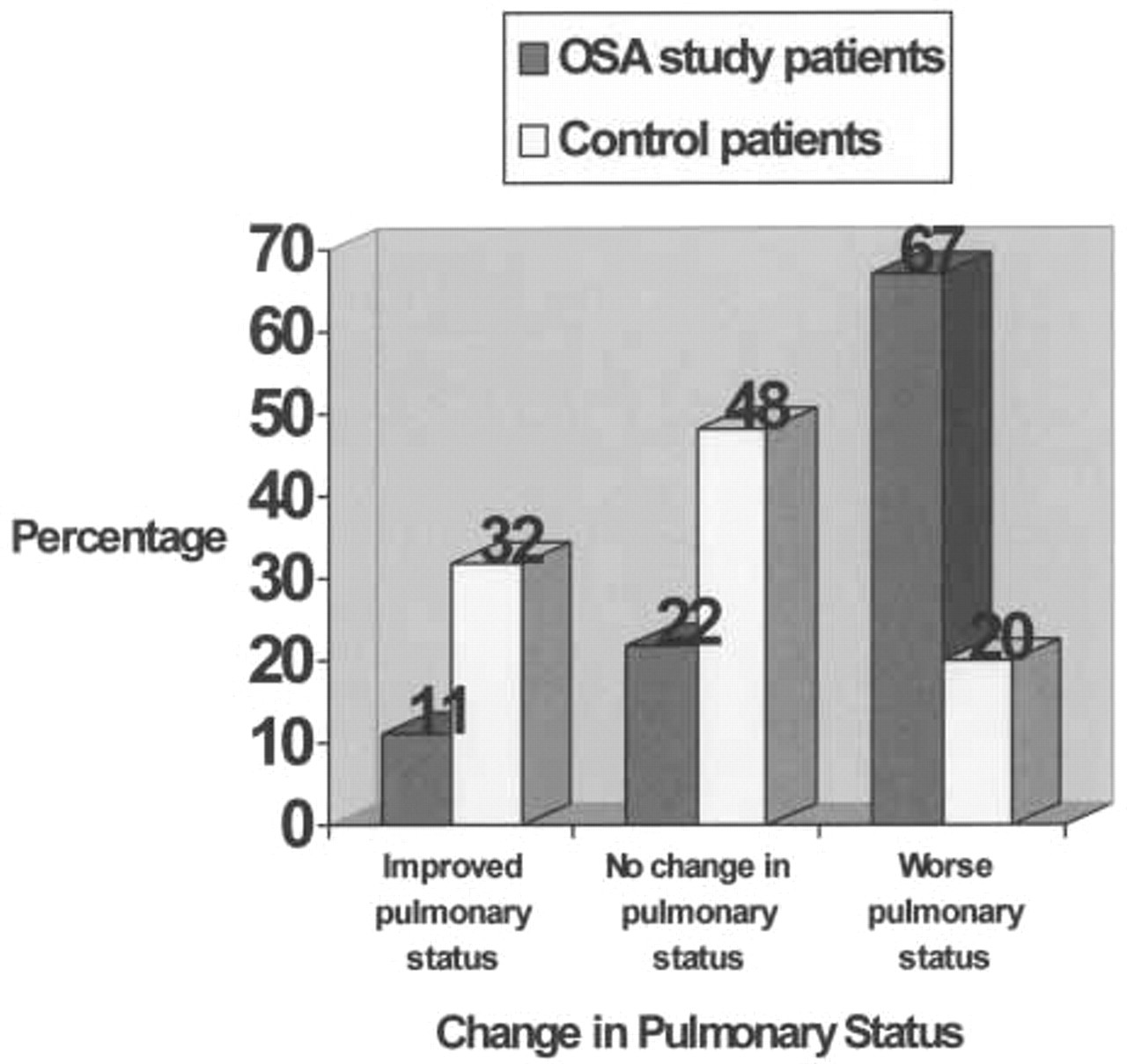
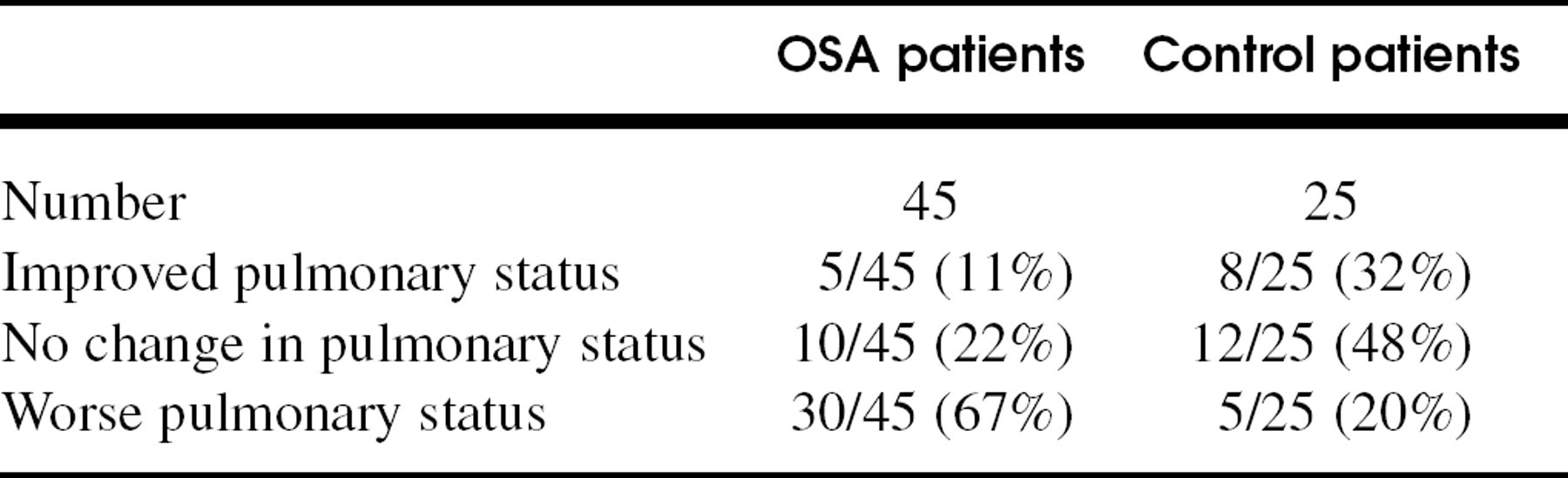
Pulmonary status in both OSA patients and control group is represented after tracheotomy. A majority of OSA patients demonstrated a worse pulmonary status, or increased pulmonary edema, after tracheotomy (30/45, 67%), whereas a minority had no change (10/45, 22%) or had improved (5/45, 11%) pulmonary status. Most patients from the control group demonstrated no change in the pulmonary status (12/25, 48%), whereas only the minority (5/25, 20%) had a worse postoperative pulmonary status.
Preoperative and postoperative chest radiographs from within 24 hours of the procedure were reviewed by a radiologist in a blinded fashion. These included both posteroanterior (PA) and lateral CXRs as well as portable anteroposterior (AP) CXRs. The postoperative CXRs were typically portable, supine AP CXRs. Markings on the CXRs were obscured by card shields across the dates and demographics; the mediastinum was shielded to obscure the presence or absence of tracheotomy tubes and thus prevent the radiologist from any bias related to knowledge of preoperative or postoperative status. Each chest radiograph was graded in an analog fashion on a scale of 0–10, 0 representing a clear CXR, and 10 representing diffuse, bilateral airspace disease consistent with severe pulmonary edema. A grade of 1–3 was assigned as mild pulmonary edema (Fig 1), 4–7 was assigned as moderate pulmonary edema (Fig 2), and 8–10 assigned as severe pulmonary edema. Any increase in radiographic score was considered significant for a change in pulmonary status, though there was no cut-off that defined “pulmonary edema.” The paired CXR results within the study and control groups were compared using the Student t test. Results were analyzed and grouped into subsets: (1) acquired/worsened pulmonary edema, (2) unchanged pulmonary status, and (3) improved pulmonary status after tracheotomy.
Pulmonary status after trachostomy
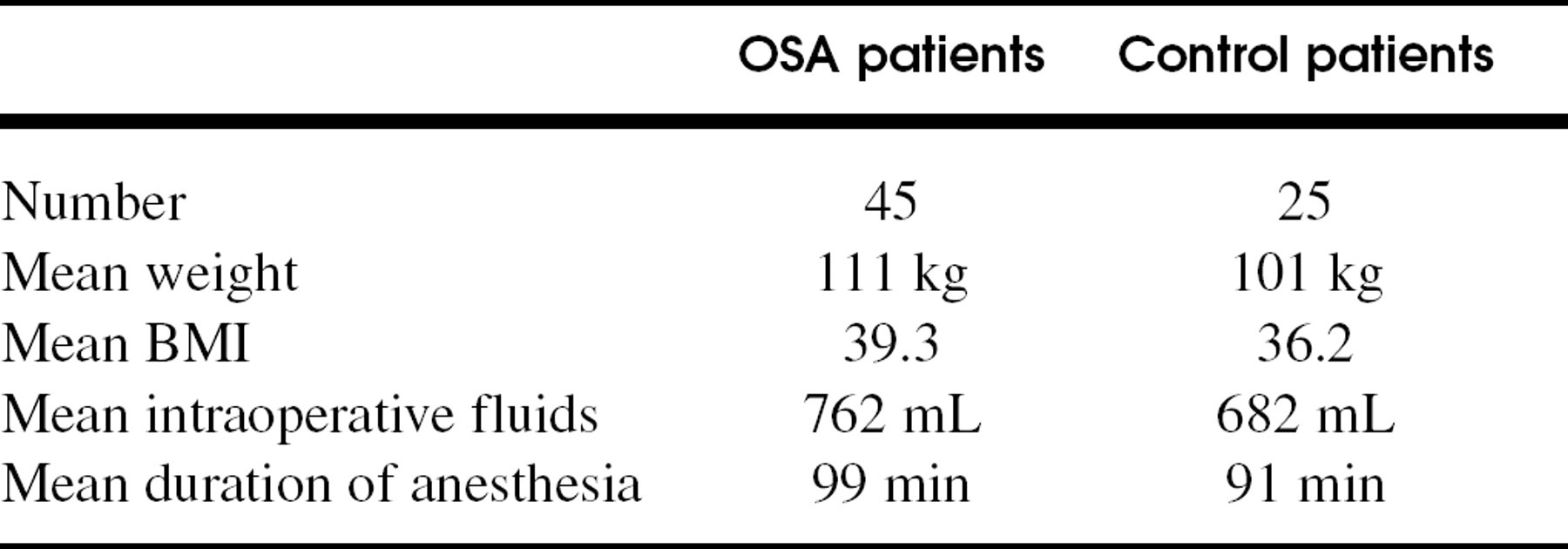
Patient demographics
RESULTS
Analysis of preoperative and postoperative CXRs revealed that 30 (67%) of 45 patients with the diagnosis of OSA developed or had worsening of pulmonary edema after tracheotomy. This compares to 5 (20%) of 25 control patients who developed pulmonary edema postoperatively. The difference between these 2 groups is statistically significant based on the Student t test with a P value of < 0.01 (Fig 3).
Thirty (67%) of 45 OSA patients who were treated by tracheotomy had an increase in radiographic score postoperatively, consistent with postobstructive pulmonary edema. Ten (22%) of the 45 had no radiographic change postoperatively, and 5 (11%) showed an improvement. In the control group, 12 (48%) of 25 demonstrated no radiographic change; 8 (32%) of 25 improved and 5 (20%) of 25 had a degree of pulmonary edema radiographically (table 1).
Fifteen (33%) of 45 patients in the study group and 20 (80%) of 25 patients in the control group had no change or had improvement in their CXR after tracheotomy.
Among those patients in the study population who developed worsening pulmonary edema, slightly less that half, 13 (43%) of 30 had radiographic evidence of pulmonary edema preoperatively with progression after tracheotomy (Fig 4). Six (20%) of 30 study patients that developed worsening pulmonary edema had clinical evidence of cor pulmonale preoperatively. The remainder of the study group, 26 (57%) of 45 patients, had no evidence of pulmonary edema preoperatively. Two (7%) of 45 patients with severe OSA died as a result of cardiac dysrhythmias in the postoperative period, having developed fulminant posttracheotomy pulmonary edema.
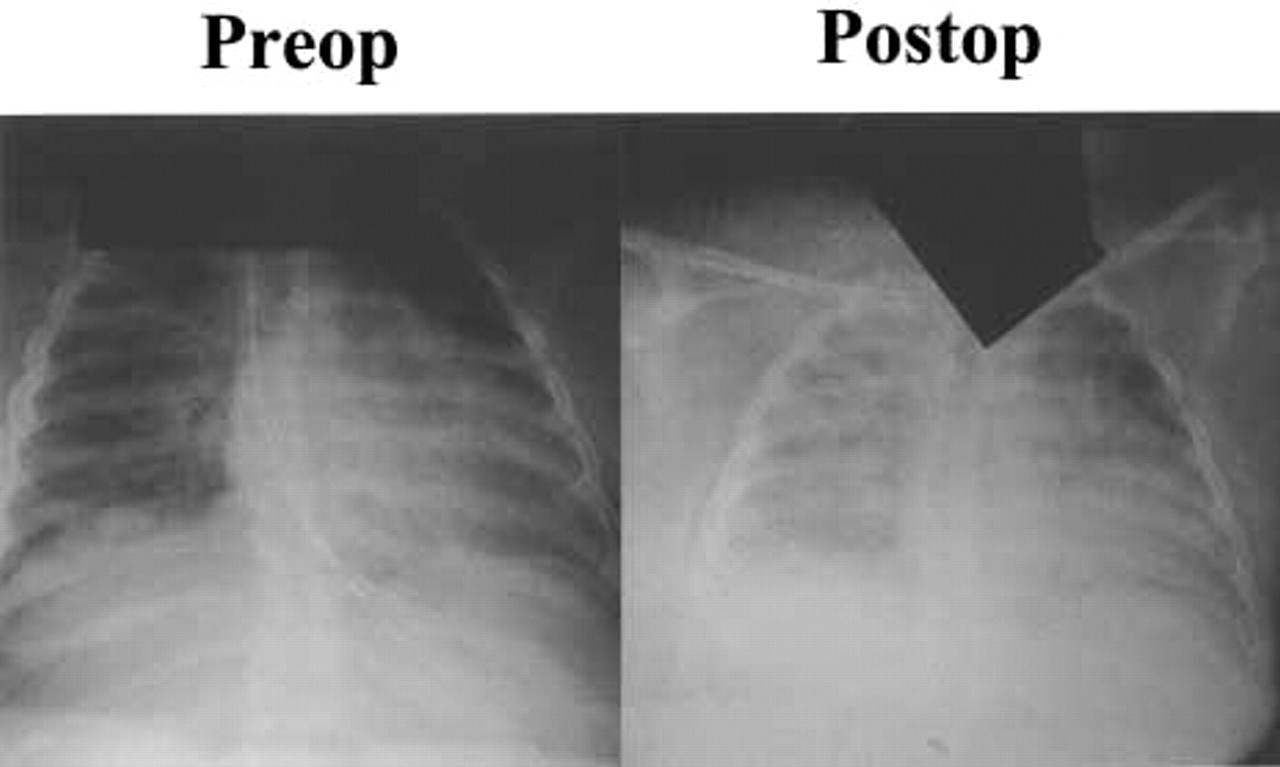
These are paired preoperative and postoperative CXRs of a 52-year-old male patient with severe OSA who developed postobstructive pulmonary edema 24 hours after tracheotomy. This patient had pre-existing moderate pulmonary edema before the tracheotomy that was graded as 4/10; the postoperative score was 8/10 reflecting a transition to severe pulmonary edema. Screens were placed over the upper trachea to blind the reviewing radiologists of the patients pretracheotomy or post-tracheotomy status.
The study and the control group patients were matched to reduce observer error and bias in the analyses. Differences between weight, intraoperative fluid administration, and total anesthesia time were not statistically significant based on the paired Student t test, P < 0.01 (table 2).
In the study population, those with OSA that developed POPE were mostly graded as having mild pulmonary edema (22 of 30, 73%). Far fewer were graded as having moderate pulmonary edema (6 of 30, 20%), and fewer still with severe pulmonary edema (2 of 30, 7%). The numbers for those patients in the control group who developed pulmonary edema were much smaller: 1 in 5 or 20% developed mild pulmonary edema, 3 in 5 or 60% developed moderate pulmonary edema and 1 in 5 or 20% developed severe pulmonary edema (Fig 5).
DISCUSSION
The occurrence of pulmonary edema after acute upper airway obstruction is well recognized. 4–10 OSA represents a chronic form of upper airway obstruction and we believe the same physiologic principles are applicable when the airway obstruction is relieved by tracheotomy, resulting in pulmonary edema. Our results are significant for an increased radiographic presence of pulmonary edema compared with a matched patient population who also underwent tracheotomy, despite the likely presence of undiagnosed OSA in this group of obese control patients. We have not made an attempt to correlate the radiological severity with the patients' clinical status owing to the difficulties of a retrospective review. It was clear, however, that many of these patients were managed in the ICU-setting requiring treatment for new onset pulmonary edema, exacerbation of pulmonary edema. or frank cor pulmonale, and that another subset of patients had postoperative problems that manifested as difficulty with pulmonary toilet or secretions. We believe that this last set of patients may have had unrecognized transient POPE and may have benefited from appropriate care directed against its development.
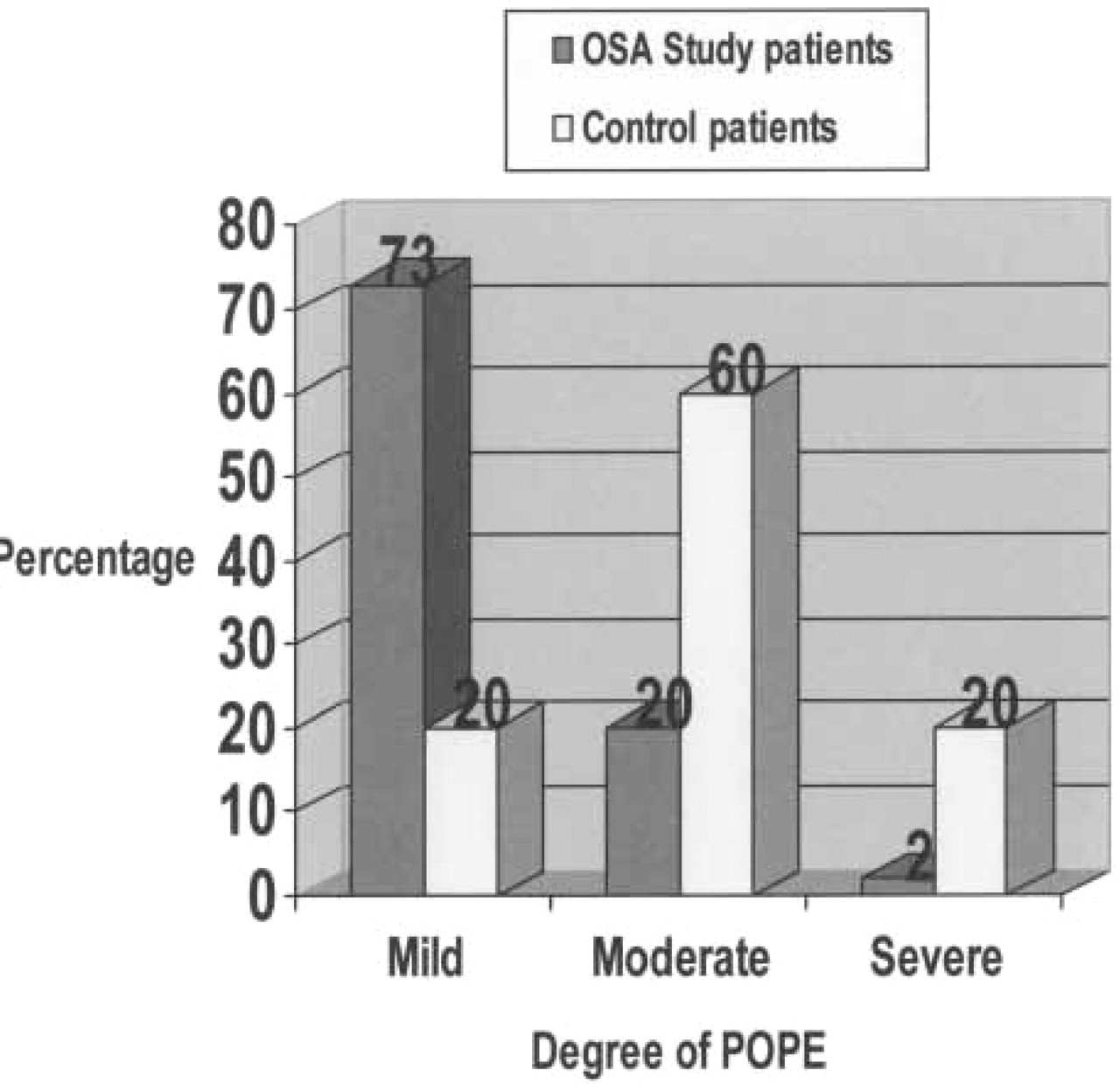
Those study patients with OSA that developed POPE were mostly graded as having mild pulmonary edema (22/30, 73%). Far fewer were graded as having moderate pulmonary edema (6/30, 20%), and fewer still with severe pulmonary edema (2/30, 7%). The figures for the control population appear more random though the total numbers involved are small. One fifth or 20% developed mild pulmonary edema, 3/5 or 60% developed moderate pulmonary edema, and 1/5 or 20% developed severe pulmonary edema.
The first reports of pulmonary edema after relief of acute airway obstruction were published in 1977 by Travis et al 4 in children and Oswalt et al 5 in adults. Numerous case studies have been published since that usually involve infants with acute epiglottitis/croup, 4,7 postlaryngospasm, 8 or removal of foreign bodies, and in adults with airway obstruction from such diverse causes as trauma, 5 neoplastic obstruction, 6,9,10 and strangling. 5 Relief of chronic obstruction has been limited mainly to pediatric patients after adenotonsillectomy for either chronic tonsillitis or OSA. This same POPE can be relieved through the institution of positive end expiratory pressure (PEEP) ventilatory support and the judicious use of diuretics, more apt in those with preexisting congestive heart failure. 7
Various pathophysiologic mechanisms have been proposed to explain the occurrence of postobstructive pulmonary edema. Initially, the pulmonary edema was thought to result from the transudation of fluid through an injured alveolar membrane caused by the large negative intrathoracic pressures that result from breathing against an obstruction. 5 As the complex mechanics of this process have been studied, it is clear that these large negative pressures increase intrathoracic venous return that in turn increases the transpulmonary hydrostatic pressure. 3,11 Physiological PEEP from the obstructed airway counterbalances this positive intravascular pressure, but when relieved of the obstruction, the lack of PEEP permits the transudation of fluid into the alveolar spaces resulting in pulmonary edema.
Hypoxia from airway obstruction exacerbates the physiology of POPE. Hypoxia will cause a systemic adrenergic release thereby causing systemic vasoconstriction, further increasing venous return. In the lungs, vasoconstriction elevates the intravascular pressure thereby encouraging the transudative process. 7
These mechanisms fit an acute obstructive process, but incompletely explain the chronic situation found in OSA patients. The physiology of a patient with chronic airway obstruction differs in that the repetitive, chronic negative pulmonary intravascular pressures are counterbalanced by a reactive pulmonary vasoconstriction and increase in pulmonary artery pressure. With time, pulmonary hypertension and often systemic hypertension develop with ensuing hypertrophy of the tunica media of the pulmonary arterial vasculature and eventually right-sided heart failure or cor pulmonale develop. 12 Total relief of airway resistance is achieved by placement of a tracheotomy that also removes any auto-PEEP that also may have counterbalanced the transudative forces. The tracheotomy would tip the intrapulmonary balance by thus favoring the development of pulmonary edema.
The resolution of POPE occurs over approximately 48 hours during which the cardiopulmonary physiology equilibrates. The institution of supportive care using PEEP, oxygen, and judicious diuresis aids this recovery and may help prevent further cardiovascular morbidity in those patients with OSA with or without underlying cor pulmonale. A curiosity of the study was the evidence preoperative pulmonary edema in OSA patients without the diagnosis of cor pulmonale. We believe that this subgroup of patients had not yet been labeled with cor pulmonale, clinically though had radiographic evidence fitting with the diagnosis. Continuous positive airways pressure (CPAP) or the application of PEEP has been studied extensively in OSA patients. 13 In this population, CPAP acts by pneumatically splinting the upper airway and thus preventing the obstructive episodes characteristic of OSA. In the treatment of POPE, the application of PEEP is effective in a different manner. The PEEP counterbalances the higher intravascular hydrostatic pressure and impedes the transudation of edema fluid, both treating and preventing the occurrence of POPE.
“Near miss” death has been described in the OSA patient within the critical care setting. 14 The combination of OSA and COPD or hypercarbic, hypoxemic states predisposes patients to respiratory failure, triggered by events such as bronchospasm, facial trauma, or lower respiratory tract infections. 15 The morbidity of this respiratory failure can be reversed with the effective treatment of OSA. Many of the patients in our own study required prolonged intensive care, and significantly there were 2 deaths that occurred after the development of POPE.
It is important to note that the comparison of chest radiographs represents a very blunt tool for investigating pulmonary edema (Figs 1 2, and 4). This difficulty is compounded by the often corpulent body habitus of the patients and the increased pulmonary atelectasis and decreased pulmonary volumes that result from postoperative recumbency. Our review was done retrospectively and other measures of declining pulmonary status such as arterial blood gases or invasive vascular monitoring could not be collated. In addition, the presence of increased pulmonary edema does not necessarily imply a worsening of the patient's clinical status. What is shown is the increased occurrence of radiographic POPE in patients with OSA after a tracheotomy. These findings support the need for a prospective investigation that would include objective monitoring data, stratification of the severity of OSA with polysomnography, clinical assessment, and outcome measures.
CONCLUSIONS
Patients with severe obstructive sleep apnea who undergo tracheotomy for relief of the upper airway obstructive process are at an increased risk for postobstructive pulmonary edema. A high index of suspicion should be present for the development of this phenomenon and to allow the appropriate institution of PEEP, oxygen supplementation, and diuresis. Awareness of this condition may help provide more timely and appropriate postoperative care and reduce the morbidity, mortality, and hospital stay required for treatment of this disease.