
Abstract
OBJECTIVE: We set out to study the effects of radiation therapy on laryngeal tissue barriers in a canine model as described by Welsh.
STUDY DESIGN: India ink was injected into 1 vocal fold on irradiated and nonirradiated canine larynges.
RESULTS: The india ink dye spread more prominently into the supraglottis of the irradiated specimens by submucosal lymphatics. Larger dye volumes simulating larger tumor bulk spread to the contralateral larynx in irradiated specimens.
CONCLUSION: Conservation laryngeal surgery for laryngeal carcinoma is a popular method of treatment. Some surgeons advocate partial laryngectomy for radiation failures; in other instances, it is the primary modality of treatment. These findings suggest a cautious approach when planning conservative laryngeal surgery after radiation therapy failures of glottic carcinoma.
In deciding between radiation therapy or surgery for small laryngeal cancer, the oncologic surgeon considers many factors, such as, patient status, age, status of the cervical nodes, demographic, logistic variables, cost, and especially patient preference.
If radiation therapy is chosen, the patient may be spared resection of the larynx. After irradiation, there are a small number of failures with either recurrence or persistence of disease that then require surgery. The rationale underlying conservation surgery of the larynx is based on anatomic studies that demonstrated compartmentalization of the larynx. This anatomic compartmentalization allows for very narrow margins in certain areas of the larynx. The larynx is unique in this regard, as other areas in the upper aerodigestive tract require margins of a centimeter or more when resecting invasive squamous cell carcinoma. The integrity of these laryngeal tissue barriers after radiation therapy has not been assessed. The question now frequently encountered is whether conservation surgery can still be undertaken after radiation therapy. Head and neck surgeons are very much divided on this issue. Some advocate limited resections (ie, conservation surgery) for small glottic recurrences whereas others feel total laryngectomy is indicated.
Early observations by Hajek (1891) revealed that laryngeal edema tended to be compartmentalized in reproducible patterns. Subsequently these compartments were demonstrated in anatomic studies using dye and radioisotope injection techniques. 1 In 1962, Tucker and Smith 2 published a histologic study of fetal larynges and demonstrated the anatomic basis of the earlier observations. Histologic studies relating this anatomy to the spread of laryngeal carcinoma have been per-formed. 3–7
Olofsson and van Nostrand 3 noted that vertical extension of glottic carcinoma was more common than horizontal spread. The conus elasticus was seen to resist tumor invasion initially. Once a tumor reaches the anterior commissure, it tends to invade the subglottic region. Kirchner and Carter 4 noted that the anterior commissure tendon initially is a strong barrier to the spread of tumor, and it is only when there is extension superiorly (just a few millimeters) or inferiorly (at least 1 cm) that cartilage invasion occurs. Extension to the contralateral cord can occur without deep invasion. He found no instances where the tumor was confined to the glottis when there was invasion of the cartilage. Kirchner and Carter pointed out that this correlated with Welsh's findings. Welsh et al 8 injected dye into Reinke's space and found that it did not penetrate the anterior commissure but rather went around it.
Conservation surgery of the larynx is predicated on both the above anatomic compartmentalization and on subsequent patterns of tumor spread, especially in smaller lesions. The practical clinical application is that oncologically sound surgical procedures have evolved for laryngeal carcinoma in which tumor margins are measured in millimeters. This concept of millimeter surgery is demonstrated in supraglottic laryngectomy where the inferior margin at the ventricle is only a few millimeters while the base of tongue margin is a centimeter or more. Recurrences occur at the base of tongue, however, not in the inferior margins. 9 Likewise glottic conservation surgery in appropriately selected cases has cure rates equal to that of total laryngectomy. 5
The results of therapy for small (T1 or T2) carcinomas of the glottis are apparently equal for surgery or radiation therapy (XRT). Many patients have opted for primary radiation for cure. For patients receiving XRT, about 5% and 17% will recur with T1 and T2 lesions, respectively, and will require surgical salvage. 10 If this recurrence is small, the question then arises whether the individual is a candidate for conservation therapy.
Radiation therapy failures for supraglottic cancer have been shown to do poorly after supraglottic laryngectomy and most people agree that total laryngectomy is indicated for recurrences. 11 However, in glottic radiation therapy failures, there is disagreement among head and neck surgeons as to whether conservation surgery is appropriate.
Several clinical series 12–15 have indicated good results with salvage conservation laryngeal surgery for glottic carcinoma. Brandenburg et al 16 examined coronal sections from 89 wide field laryngectomy specimens; 20 specimens were radiation failures of T1 or T2 glottic carcinoma and were compared with 69 primary surgery specimens from larger tumors. He found that cartilage invasion was more prevalent in the radiation failures. He also felt that staging was less accurate and that the conus elasticus and perichondrium may not provide a barrier to microscopic spread of tumor. He concluded that conservation laryngeal surgery may fail to cure disease in glottic carcinoma after radiation therapy failure.
Certain factors must be considered in this regard. Most importantly, one must realize that when squamous cell carcinoma is treated with radiation therapy, the tumor does not “shrink” to a central point. If radiation fails to eradicate disease and persistent tumor is found, it is present as scattered nests of tumor cells in the entire tissue volume that was previously involved with the tumor. 3 Furthermore, frozen section evaluation of margins is more difficult in previously irradiated fields.
For conservation laryngeal surgery of XRT failures to be successful, certain conditions must be met. First, the initial primary tumor (ie, before XRT was given) must have met criteria for conservation surgery. The entire tissue volume previously involved with tumor must be excised with appropriate margins. This is important because, on clinical examination, one may only see edema or a small area of obvious tumor and this may lead one to underestimate the extent of the disease. Finally, the spread of tumor should still be along contiguous pathways that are predictable based on anatomic boundaries and thus allow correlation of clinical findings with extent of disease and resection of the tumor with acceptable narrow margins.
In this study, the effects of irradiation on the endolaryngeal region were examined to determine whether there is: (1) modification of lymphatic flow subsequent to radiation therapy for cancer of the cords, and (2) whether an alteration of the translymphatic channels after failure of radiation therapy would impact on subsequent curability by local resection. The study is based on the recognized analogy between the spread of cancer cells via the local lymphatics and the identification of these channels by the infusion of a particulate agent such as india ink.
Injection of the india ink need not be done in the living state as it has been previously shown that the result in the nonvital state does not bias the direction and extent of lymphatic flow. From a technical standpoint, it is much easier to perform the injections in the isolated larynx that allows a more accurate analysis. The same technique performed in human cadaver larynges correlates with the canine model. 8
MATERIALS AND METHODS
As an overview, the basic approach involved treating canine larynges with therapeutic doses of radiation therapy. After a period of 1 year, the animals were sacrificed and the larynx removed, then immediately injected in the glottic region with india ink and the spread of the dye observed grossly and histologically. Specific details and rationale follow.
The canine model was used as it had been previously in similar studies and had been shown to correlate with human anatomy and pathophysiology. We chose a waiting period of 1 year after radiation therapy for 2 reasons. First of all, this period of time corresponds to the time when recurrences tend to be discovered (about 85% of recurrences occur within the first 2 years). This period of time also allows for radiation-induced changes to occur. Six adult dogs (Beagles) in the range of 20 to 30 pounds were used as the size of the larynx was adequate to work with but not too large for embedding and sectioning on the microtome in the pathology lab.
The technique of radiation therapy was an external beam at a dose of 6600 cGy. The radiation therapy was delivered over 35 treatments, given 5 days per week in single daily exposures. A cobalt 60 source was used to deliver fractions of 200 cGy/day. It was necessary to shave the animals' necks in the area of the larynx so that the area to be exposed could be tattooed. Radiation was isolated to the glottic region with 2-cm margins in the superior and inferior (ie, supraglottic and sub-glottic) limits. The animals required sedation during the treatments that were achieved with 10 to 15 mg/kg ketamine/acepramazine 1.5 mg/kg IM. After the course of radiation therapy, the animals were boarded for a period of 1 year.
The animals were sacrificed with sodium pentobarbital (5 mg/kg) and the larynges immediately harvested with the following procedures undertaken. Six irradiated and 6 nonirradiated larynges were used.
India ink injections were performed using a 27-gauge needle on a tuberculin syringe. Each specimen received only 1 injection. India ink was injected into Rienke's space in the midportion of the cord. Two specimens each were injected with 0.1 mL, 0.5 mL, and 1 mL of the solution. The same was performed with the nonirradiated larynges. The specimens were then fixed and embedded in paraffin for sectioning and staining. The stains used were the Verhoeff elastin stain and routine hematoxylin and eosin (H-E) stain. The sections were coronal in orientation and spanned from the anterior commissure region to the arytenoids. Both sides of the larynx were evaluated and any microscopic spread around the anterior commissure or through the conus elasticus could be observed. Representative slides from anterior to posterior at approximately 6 to 8 even intervals were obtained (ie, 2 sections from each interval, 1 for H-E and 1 for Verhoeff stains).
Experimental Subjects
All animals were used and cared for in compliance with DOD Directive 3216.1 and AFR 169–2, The use of Animals in DOD Programs, and NIH publication 85–23, Guide for the Care and Use of Laboratory Animals for the period 1995–1997. Appropriate consideration was given to the policies, standards, and guidelines for the proper use, care, handling, and treatment of animals. Live animals were required for use in this protocol as evaluation of radiation-induced changes on otherwise normal laryngeal tissue is being evaluated. A total of 12 dogs (6 subjects and 6 controls) of the weight outlined here were used as this model has previously been shown to correlate with human laryngeal anatomy and the previously demonstrated compartmentalization in the canine model also correlates with patterns of spread of laryngeal cancer in human cadaver studies. It is an accepted and previously established animal model. Every effort was made to select procedures that avoid or minimize discomfort or pain to the animals, or to find alternatives to these procedures. In addition, these activities did not unnecessarily duplicate previous experiments.
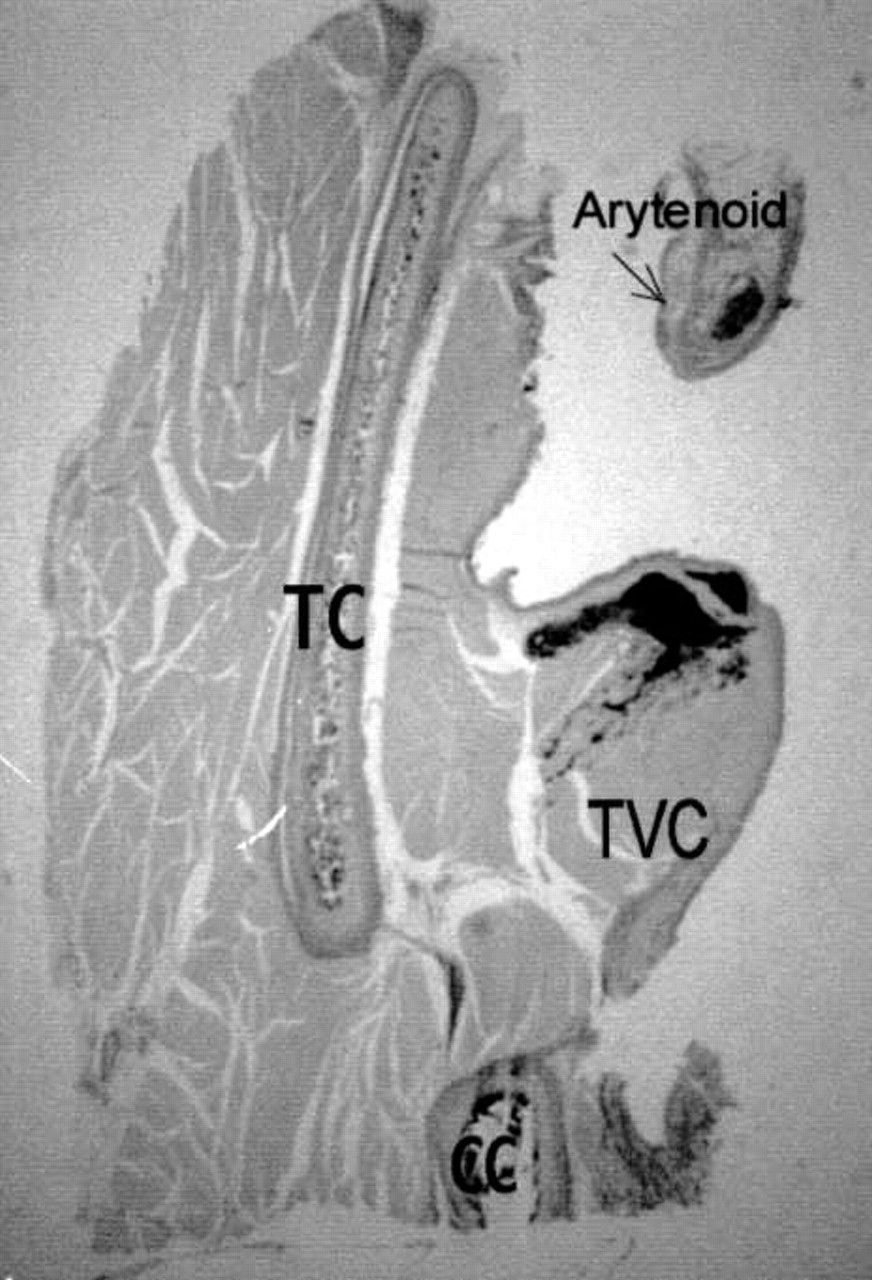
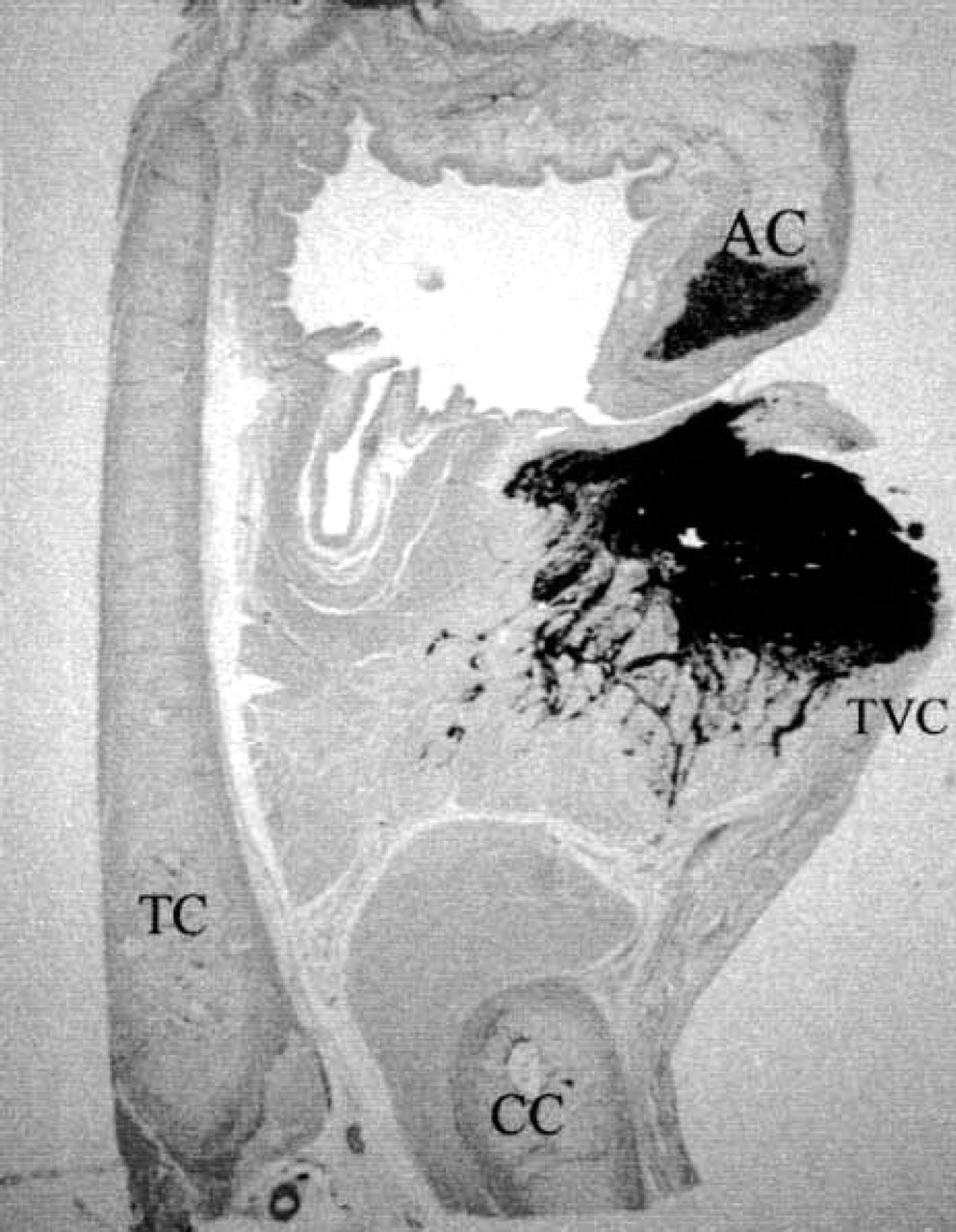
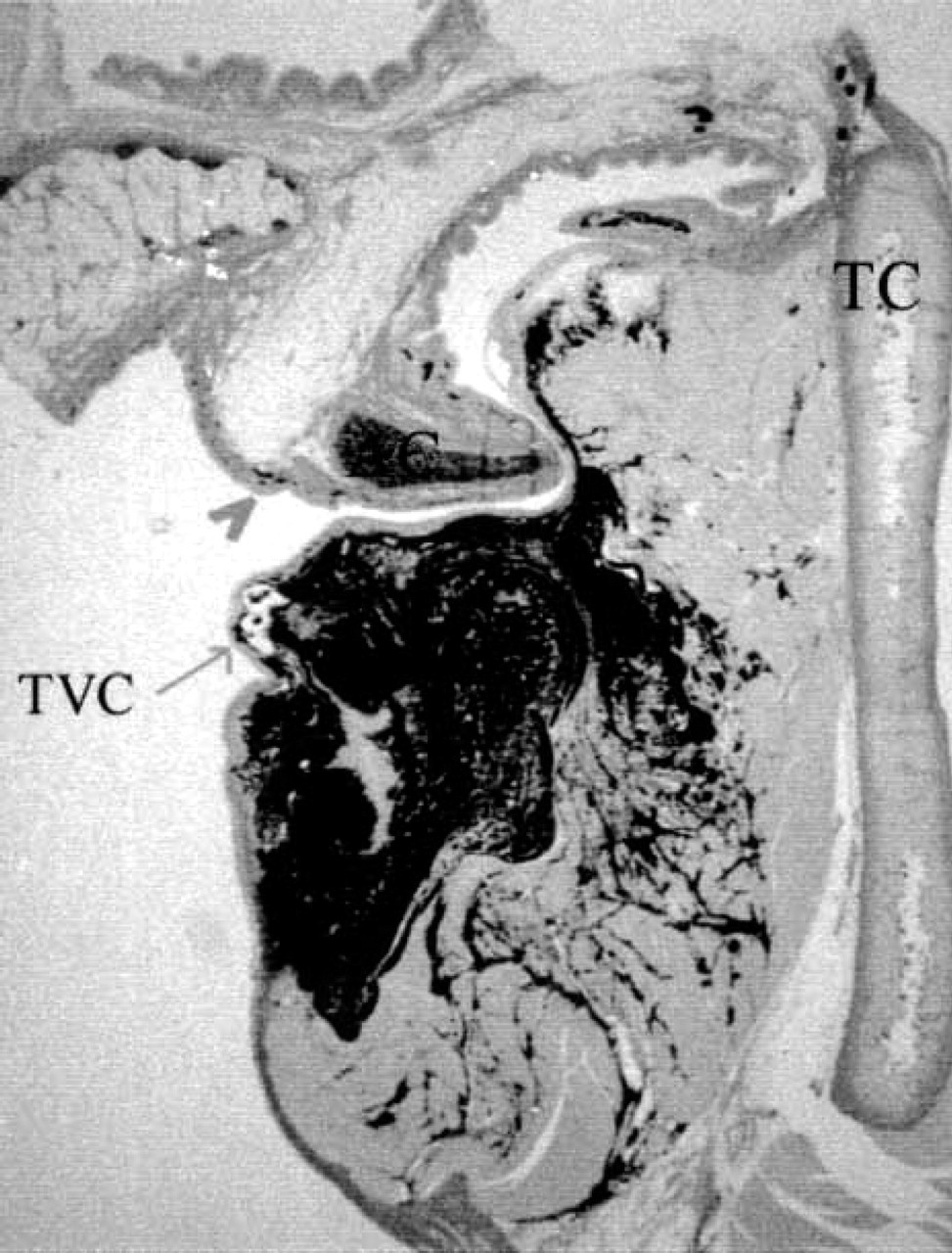
Control specimen with 0.1 mL india ink Verhoeff stain. Note lack of significant spread. Conus elasticus is not well visualized. Arytenoid is cuneiform process. Note dark staining of arytenoid cartilage with elastin stain (not india ink). (TC, thyroid cartilage; TVC, true vocal cord; CC, cricoid cartilage.)
RESULTS
After an injection of 0.1 mL india ink, there were no observed gross differences in dispersal pattern between radiated and nonradiated (control) specimens. The majority of the dye stayed within the area of Reinke's space and the superficial muscle, though some dye could be seen in submucosal lymphatic spaces in both radiated and nonradiated subjects (Figs 1 and 2). The laryngeal compartments, as delineated by the elastin stain, appeared unchanged after radiation therapy. The dye appeared to progress into the muscle layer with equal spread in nonirradiated or irradiated specimens. Microscopic dye spread, however, was noted submucosally further from the point of origin in radiated specimens (Fig 3). Dye was seen in the submucosal lymphatics over the arytenoid area under magnification with the radiated specimens (Fig 4), but not the controls. Note that most of the sections contain the arytenoid cartilage, as canine arytenoids have a prominent cuneiform process that extends anteriorly to the ventricular fold. However, this spread over the arytenoid process was not appreciated grossly.
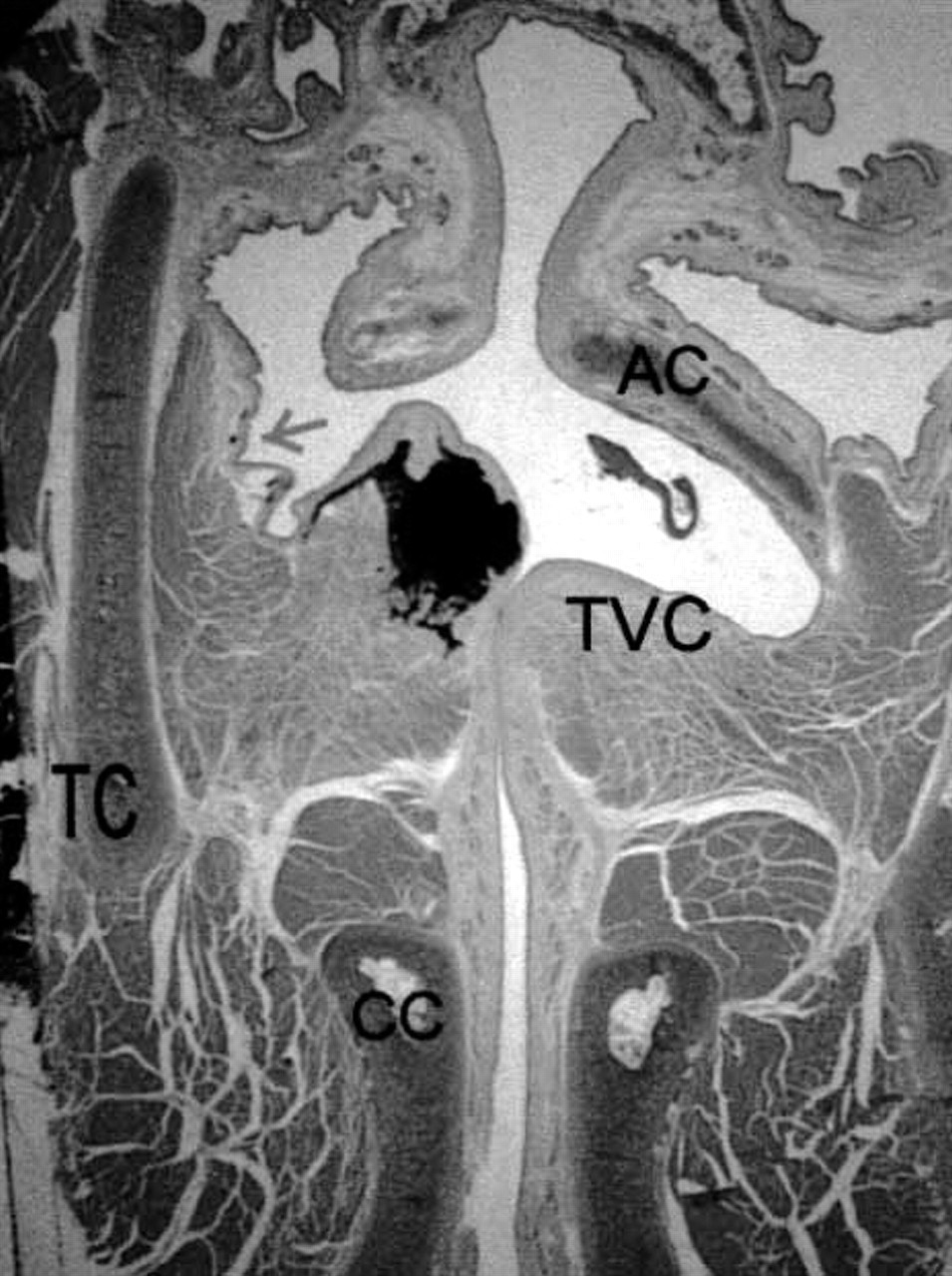
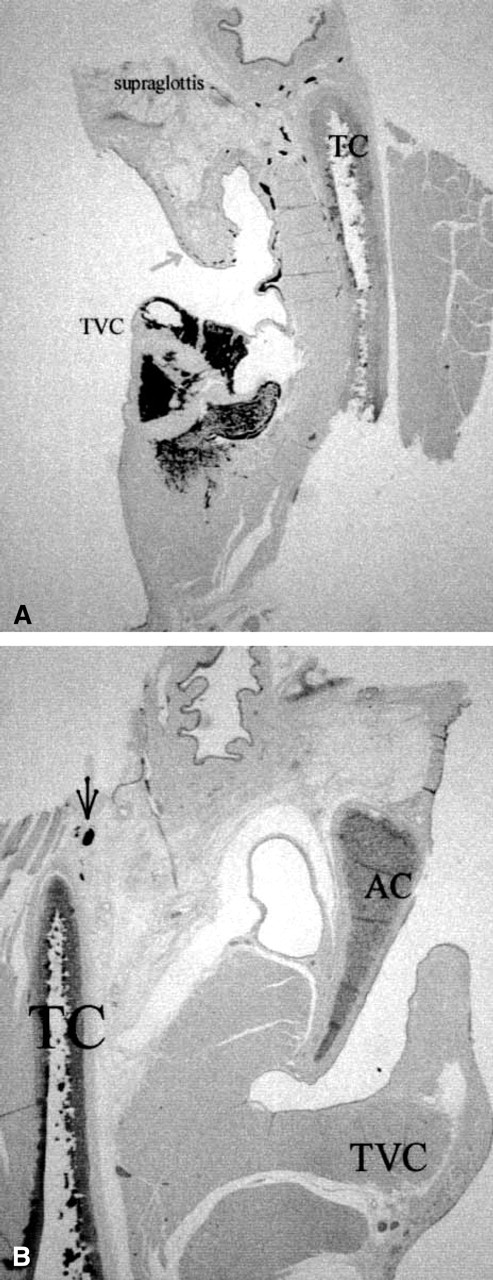
Control specimen with 0.1 mL hematoxylin-eosin stain. Minimal submucosal spread (arrow). (TC, thyroid cartilage; TVC, true vocal cord; CC, cricoid cartilage; AC, arytenoid cartilage.)
After injection of 0.5 mL of india ink, the dispersal pattern was different by gross examination for radiated versus nonradiated larynges. The radiated larynges displayed a more widespread dispersal, predominately over the supraglottis. Fine strands of india ink could be seen creeping superiorly on the laryngeal epiglottis as well as the arytenoid area, ipsilaterally, without magnification. This observation was confirmed microscopically as dye was visualized submucosally in a wider distribution pattern when compared with the nonradiated specimens (Figs 5 and 6). Only microscopically could contralateral spread be seen in the irradiated specimens, from a supraglottic pathway. No arytenoid, supraglottic, or contralateral penetration was seen in the controls. In the region of the subglottis, there was no observable difference between the 2 subject sets. In addition, the anatomic barriers appeared to be unchanged. The dye was seen traversing the tissue away from the vocal cord epithelium in direct spread, as well as submucosal lymphatic spread in both radiated and control specimens, but the radiated specimens showed greater spread. The most striking observation was the extent of supraglottic spread in the submucosal lymphatics of radiated samples.
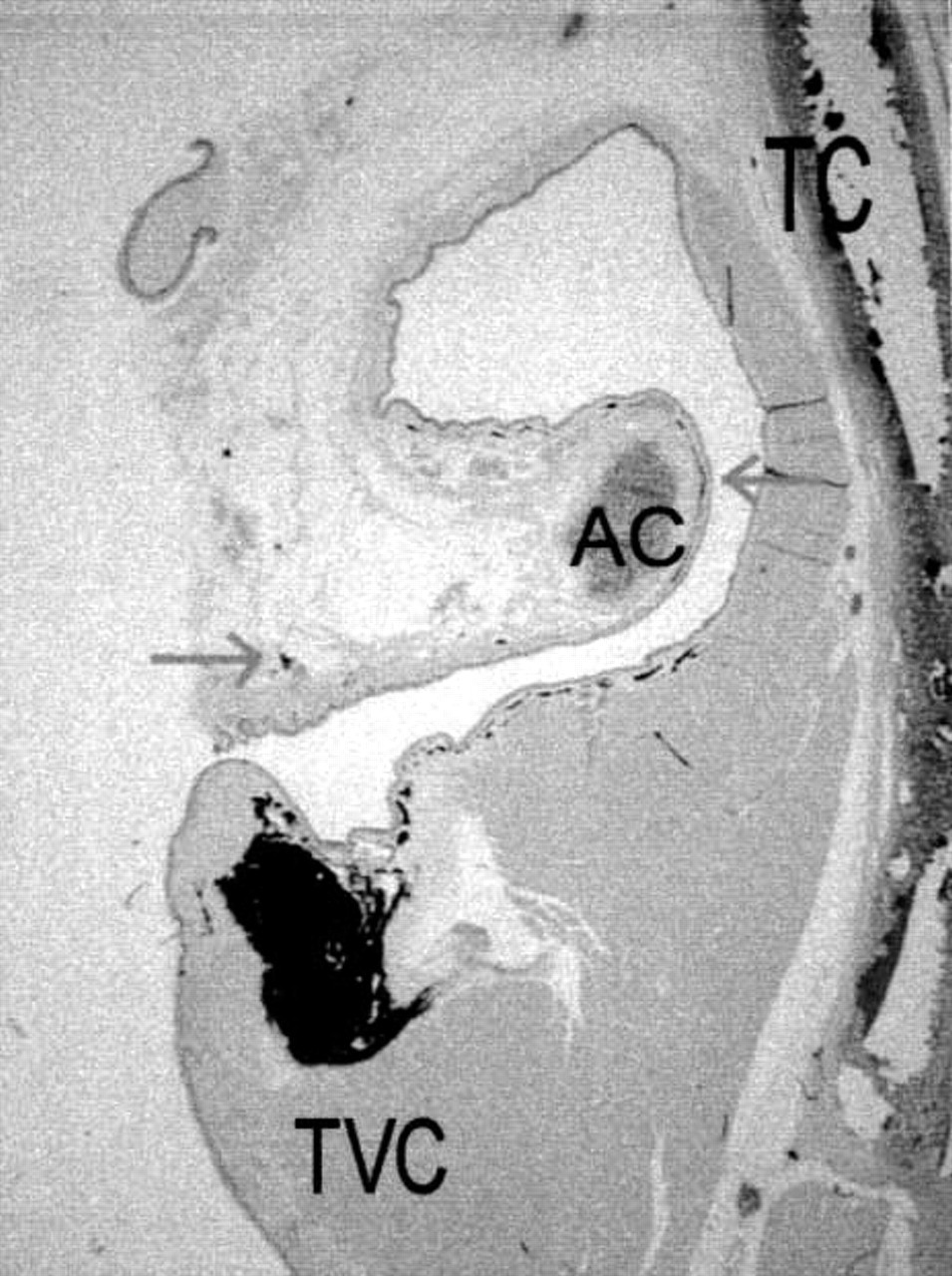
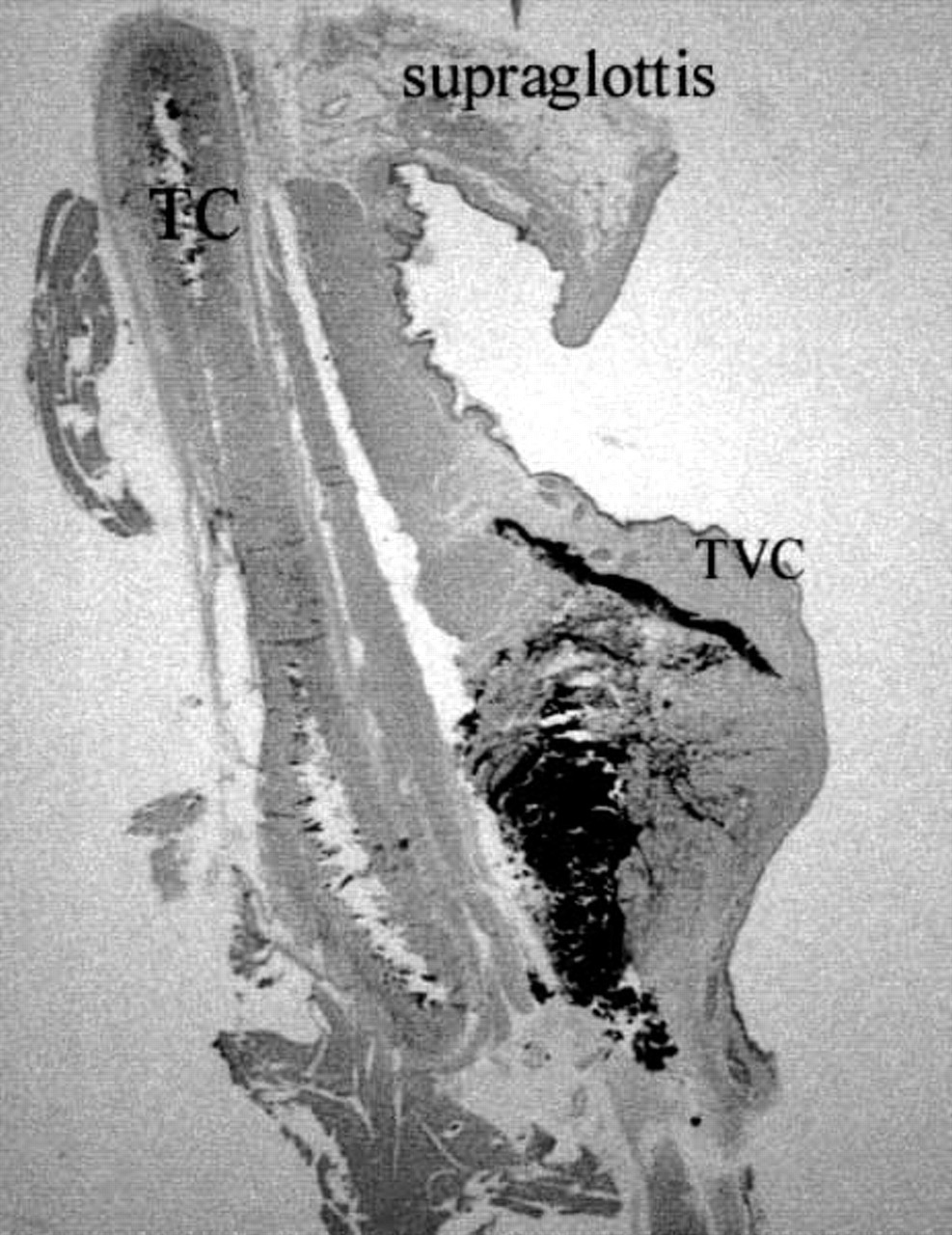
Radiated specimen with 0.1 mL hematoxylin-eosin stain. Note dye over arytenoid area (arrows). (TC, thyroid cartilage; TVC, true vocal cord; AC, arytenoid cartilage.)
Injection of 1.0 mL of india ink yielded similar results to the 0.5 mL specimens, but with a more dramatic appearance. The gross differences were more apparent as well as the microscopic findings. Again, there was little subglottic spread (Fig 7). Dye spread directly into the muscle and through submucosal lymphatics toward the supraglottis. The area of dye dispersion was much larger in the radiated specimens, though a similar pattern could be seen being initialized in the nonradiated subjects. At this volume of injection, dye could again be seen contralaterally in the radiated specimens (Fig 8 and 9), and appeared to spread via the supraglottis and not through the anterior commissure. This contralateral spread appeared to occur primarily through submucosal lymphatic spaces. No dye was seen over the arytenoid or in supraglottic tissues in the nonirradiated specimens. These observations appeared consistent for both sets of specimens in corresponding control or radiated categories.
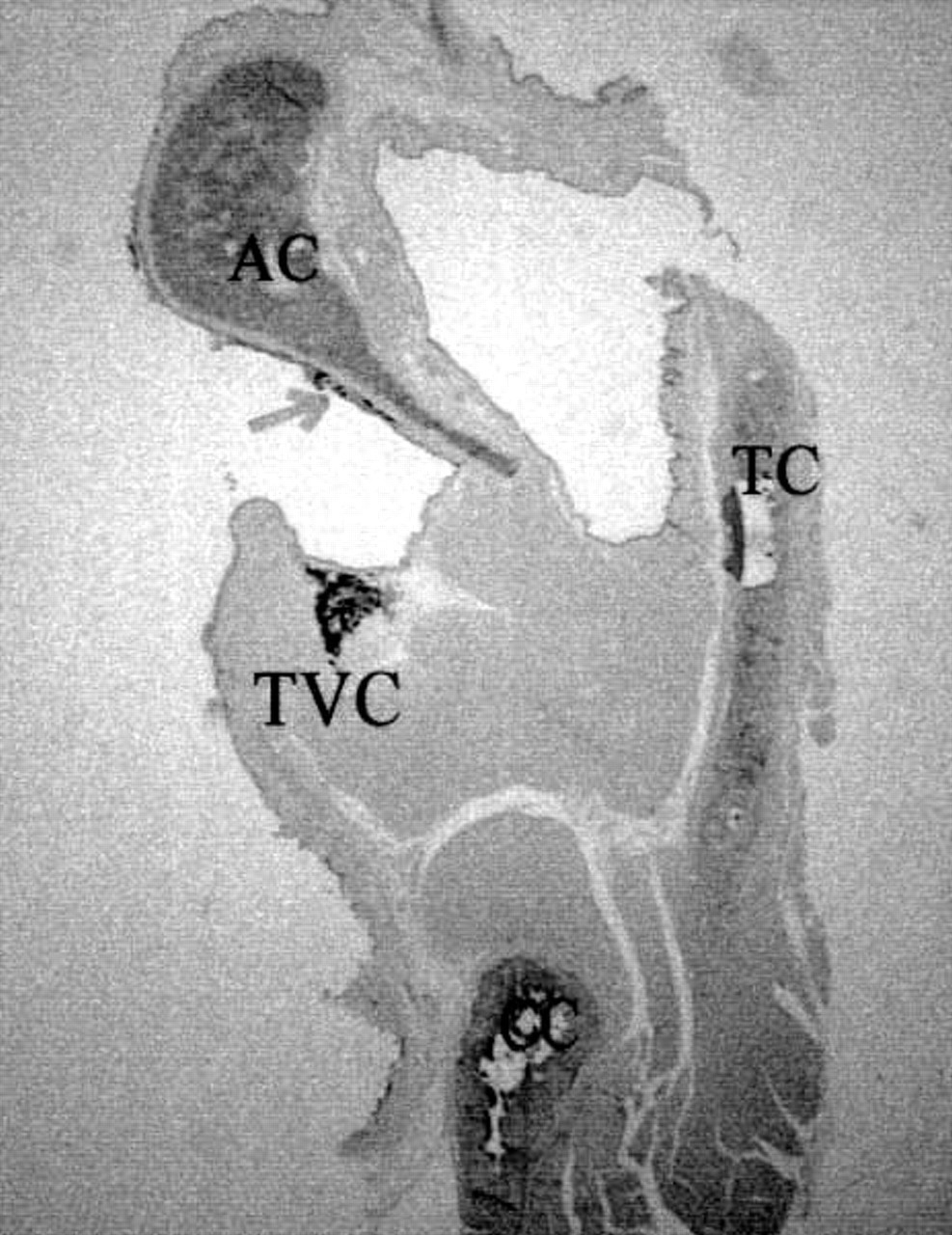
Radiated specimen with 0.1 mL hematoxylin-eosin stain. Posterior cut with dye over arytenoid (arrow). (TC, thyroid cartilage; TVC, true vocal cord; CC, cricoid cartilage; AC, arytenoid cartilage.)
DISCUSSION
Through all the specimens, the general pattern of spread was similar, but the radiated specimens consistently showed a greater area of penetration submucosal-ly compared with nonradiated ones. This spread appeared to be directed supraglottically. Even with the smallest volume of dye injection, the dye spread further into the supraglottis (cuneiform process of arytenoid) in radiated larynges. There was no contralateral spread nor was there the fine lace-like spread of ink over the arytenoids or supraglottic structures in the controls.
One of the objectives of this study was to examine, qualitatively, the change in tissue barriers after radiation therapy. We did not observe, by elastin stain or by ink boundaries, the conus elasticus and other barriers demonstrated by human studies regardless of radiation status. The most striking finding as noted above was the extent of spread through the submucosal lymphatics. It is possible that radiation therapy may have altered the submucosal lymphatic channels allowing easier flow of dye. Recanalization of lymphatics, however, has been discounted by most researchers in the past (verbal communication, Kirchner). Another consistent finding was the spread of ink primarily toward the supraglottis. It is difficult to conclude whether the dye traversed deep to the ventricle or spread posteriorly over the arytenoid then into the supraglottis. The latter is more likely as dye was more often seen over the arytenoid process (cuneiform extension) then in the ventricle at lower volumes.
Control specimen with 0.5 mL hematoxylin-eosin stain. (TC, thyroid cartilage; TVC, true vocal cord.)
We did not observe subglottic spread that previous authors 17 had described with their dye injection studies. This difference may be partly due to our injection at the superio-medial aspect of the true vocal fold, with perhaps a tendency to inject more on the superior aspect, as it was technically easier to accomplish. We attempted to keep the larynx whole until after the injection. To inject the vocal fold at its most medial aspect consistently would have necessitated opening the larynx posteriorly, possibly disrupting laryngeal lymphatic channels. Only 1 investigator injected the specimens under loupe magnification for consistency.
Another possible explanation for our finding of supraglottic spread (and contralateral spread via the supraglottis) is the interruption of regional cervical lymphatics with the subsequent isolation of the larynx. In 1983, Welsh et al 18 showed that irradiation of the regional nodes did not significantly alter the ipsilateral flow of lymphatics unless infection or surgery, which produces scarring, distorted the flow. The flow would then be rerouted to the contralateral side. In our study the larynx was isolated from its hosts as had been accomplished in prior cadaver studies. This allowed for easier and consistent injections but may have resulted in altered flow.
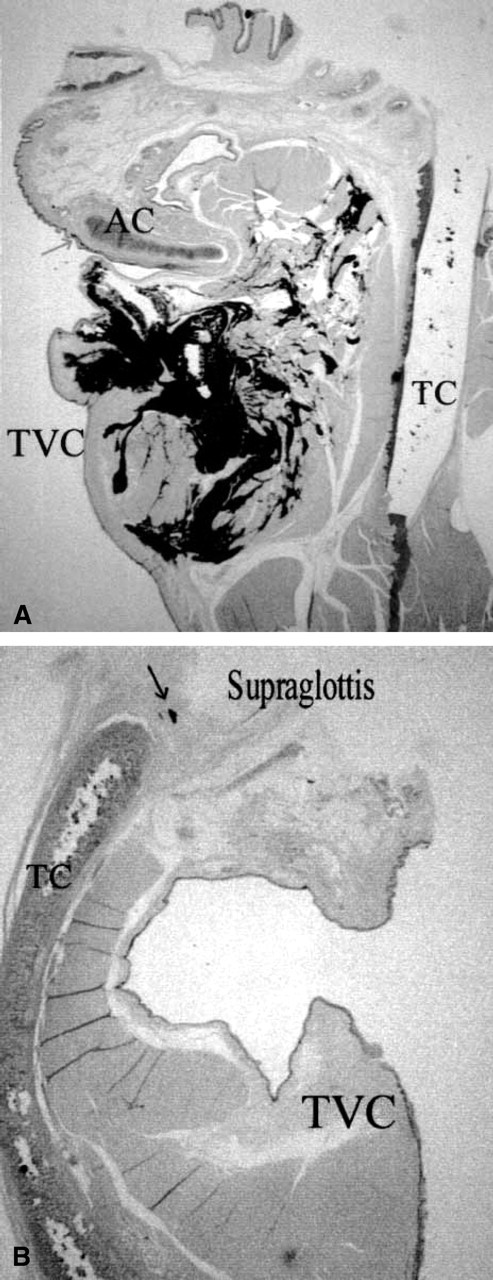
Radiated specimen with 0.5 mL hematoxylin-eosin stain. (A) Dye into ipsilateral supraglottic area (arrow); (B) contralateral dye in supraglottis (arrow). (TC, thyroid cartilage; TVC, true vocal cord; AC, arytenoid cartilage.)
Control specimen with 1.0 mL Verhoeff stain. Lack of significant submucosal spread. Note dark staining of arytenoid cartilage (not ink). (TC, thyroid cartilage; TVC, true vocal cord; CC, cricoid cartilage; AC, arytenoid cartilage.)
One might conclude that lymphatic alteration after radiation leads to wider spread of disease in cases of treatment failure. Certainly that may be implied by the consistent findings seen here, but there are only 2 specimens per category. No statistically significant conclusions can be drawn from this study. An additional consideration is that of the use of normal canine larynges. Although their use has been compared with that of the human cadaver larynx in other studies, it is not an actual human patient. The presence of tumor burden before radiation may have already changed the lymphatic architecture. Our india ink injections were done after radiation was completed. It is possible that resulting spread patterns may be different (ie, subglottic spread) for a pre-existing, but actively growing, tumor.
Radiated specimen with 1.0 mL hematoxylin-eosin stain. (A) Note dye through muscle and over arytenoid process (arrow); (B) contralateral dye in supraglottis (arrow). (TC, thyroid cartilage; TVC, true vocal cord; AC, arytenoid cartilage.)
Radiated specimen with 1.0 mL Verhoeff stain. True vocal cord (arrow); note dye throughout supraglottis and over arytenoid process (arrowhead). Also note dark staining of arytenoid cartilage with elastin stain (not india ink). (TC, thyroid cartilage; TVC, true vocal cord; AC, arytenoid cartilage.)
We did not find changes in the anatomic laryngeal barriers as was our initial goal. Instead, we discovered a pattern of dye spread that appears distinctly different between radiated and nonirradiated subjects. Radiated subjects were seen to have a larger dispersal of dye, especially notable with increased dye volumes simulating larger tumor burden. These observations tend to support Brandenburg et al 16 who contend that radiation therapy failures for glottic cancer may be associated with a more aggressive or at least understaged disease. T-stage classification with a basis on cord mobility has the inherent fallibility of not recognizing the cause of the impairment. Muscle invasion or irradiation-induced fibrosis can have the same effect limiting mobility. Hence, selection of candidates for conservation surgery of glottic carcinoma after radiation therapy failure should be done with great care.
Sincere appreciation is given to Drs J Welsh and L Welsh and Dr J Kirchner for their suggestions and encouragement for preparing this manuscript.