
Abstract
OBJECTIVE: The purpose of this study was to examine the perceptions of medical students regarding facial aesthetic surgery and those specialists most likely to perform aesthetic or reconstructive facial surgery.
METHODS: A survey was designed based on a review of the literature to assess the desirable characteristics and the perceived role of the facial plastic and reconstructive surgeon (FPRS). The surveys were distributed to 2 populations: medical students from 4 medical schools and members of the general public.
RESULTS: A total of 339 surveys were collected, 217 from medical students and 122 from the general public. Medical students and the public had similar responses. The results demonstrated that respondents preferred a male plastic surgeon from the ages of 41 to 50 years old and would look to their family doctor for a recommendation. Facial aesthetic and reconstructive surgery was considered the domain of maxillofacial and general plastic surgeons, not the FPRS.
CONCLUSION: Integration of the FPRS into the medical school curriculum may help to improve the perceived role of the specialty within the medical community. It is important for the specialty to communicate to aspiring physicians the dedicated training of an otolaryngologist specializing in FPRS.
The perceived role of otolaryngologists in FPRS among medical students has not been assessed. The specialty of FPRS is no longer in its infancy; the American Academy of Facial Plastic and Reconstructive Surgery will celebrate its 36th anniversary this year. Although facial cosmetic and reconstructive surgery has traditionally been the realm of general plastic surgeons, this is no longer the case. However, it is unclear if that is well understood by the medical community.
In many respects, the continued subspecialization of medicine has led to many otolaryngologists further sub-specializing in FPRS. FPRS is a natural extension of the intensive training an otolaryngologist receives during the 5-year residency specifically dedicated to anatomy, pathophysiology, diagnosis, and treatment of diseases involving the head and neck. However, both the public and medical profession's perception of facial plastic surgery lags behind the dramatic changes that have taken place over the course of the past decade. With the number of facial plastic and reconstructive surgery procedures rapidly increasing, 1 and the number of different specialties performing these procedures, the perceptions of medical students are important. Moreover, it is the perception of our specialty that determines the selection of a career in medicine, future referral patterns, and recommendations to friends and family. 2,3 In order to ensure a bright future for FPRS, the nature of our specialty must be communicated to the next generation of physicians early in their career.
In an era of managed health care and social reform, public perception or misconception may have a significant impact on the future of the specialty. Although certainly no medical specialty has exclusive rights over facial aesthetic and reconstructive procedures, it is important for FPRS to be ranked among the general plastic surgeons and maxillofacial surgeons, in the minds of young physicians, as most likely to perform any procedure related to facial and cosmetic surgery. The purpose of this study was to examine the perceptions of a cross-section of medical students regarding facial plastic surgery and those specialists most likely to perform aesthetic or reconstructive facial surgery.
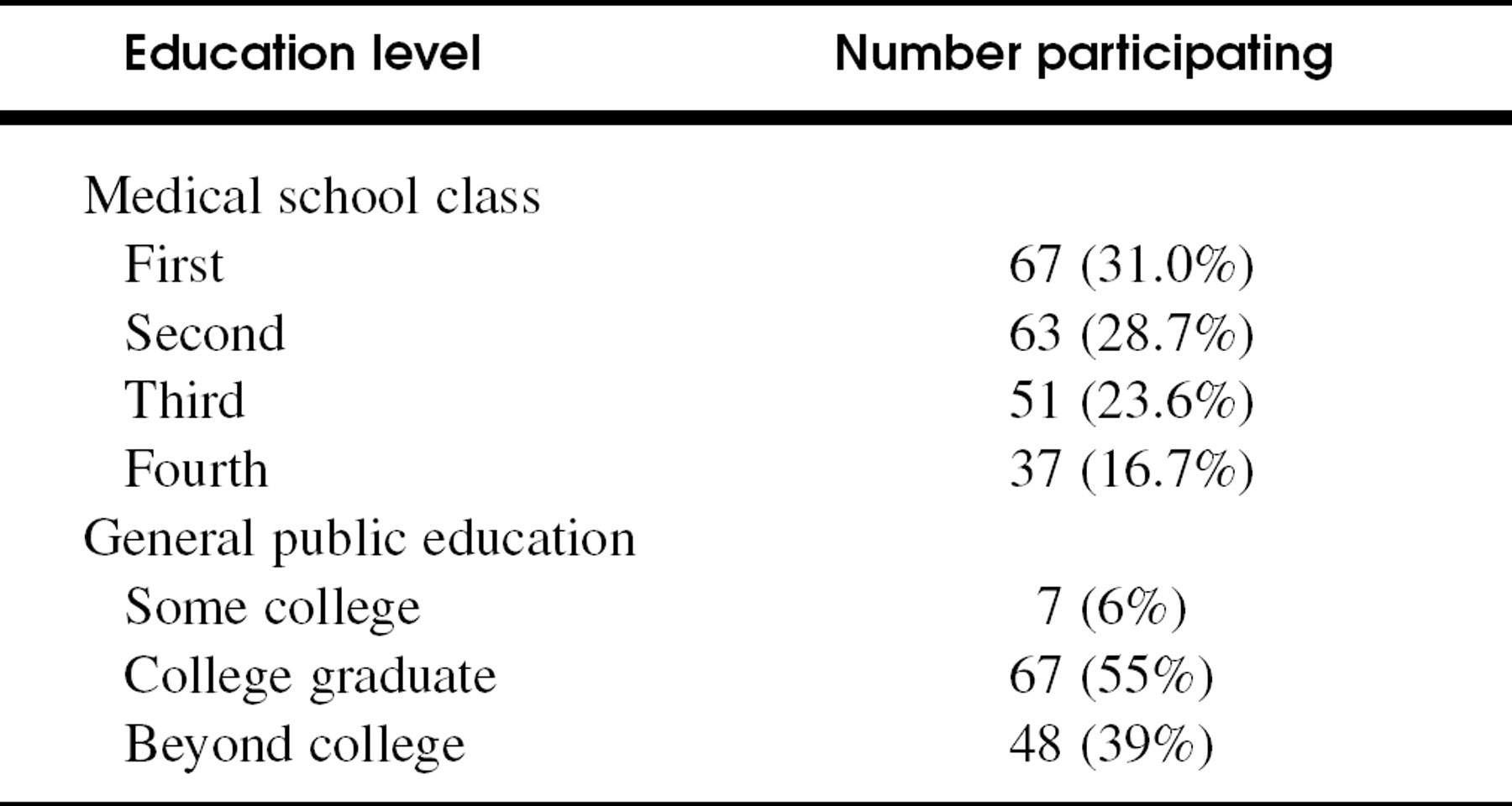
The education of medical school students (n = 218) and the educational background of the general public surveyed (n = 122)
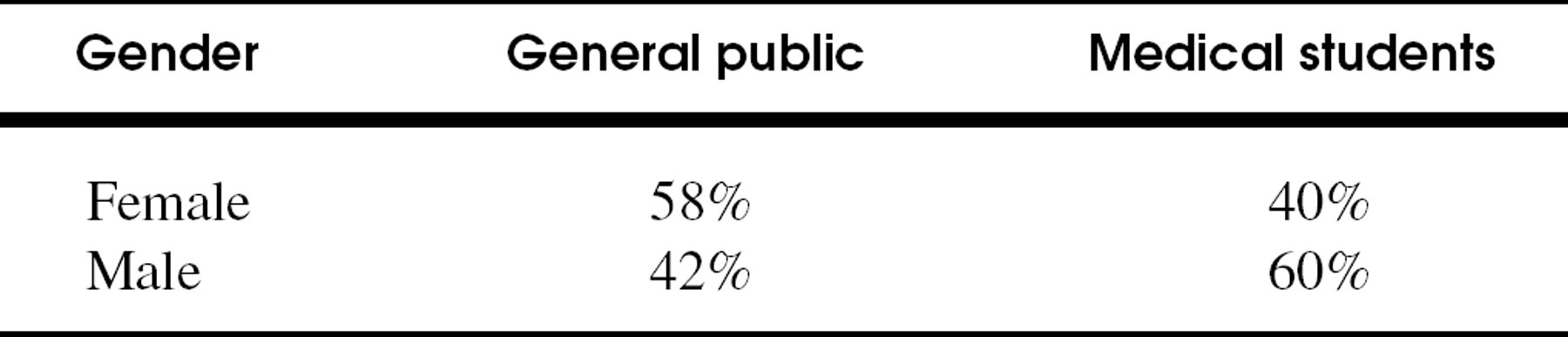
Gender of survey respondents
METHODS
To examine the perceptions of facial plastic and reconstructive surgery, we surveyed 2 populations: medical students from 4 different institutions and college-educated members of the public. The medical students were selected from medical schools around the country (University of Michigan, University of Utah, Georgetown University, and Oregon Health Sciences University). The surveys were distributed at upscale retail establishments in southeastern Michigan and northwestern Oregon.
In addition to collecting age, sex, and level of education, questions were asked regarding the responders' preferred characteristics of a plastic surgeon such as age, sex, and training. The survey questions were based on previous work examining a similar topic. 4 The following questions were asked as part of this study: Which physician is most likely to treat a cancer of the tongue? injury of the forehead? a broken jaw? facial wrinkles (collagen/botox injections)? Questions were also asked about who is most likely to perform cosmetic surgery? cosmetic surgery of the face? removal of a skin cancer of the cheek? a rhinoplasty or “nose job?” a facelift? an “eyelid tuck?” or blepharoplasty? To all of the above questions, the choices were listed as follows: oculoplastic surgeon/ophthalmologist, maxillofacial surgeon, facial plastic/ENT surgeon, general plastic surgeon, dermatologist, or not sure. (See Appendix.)
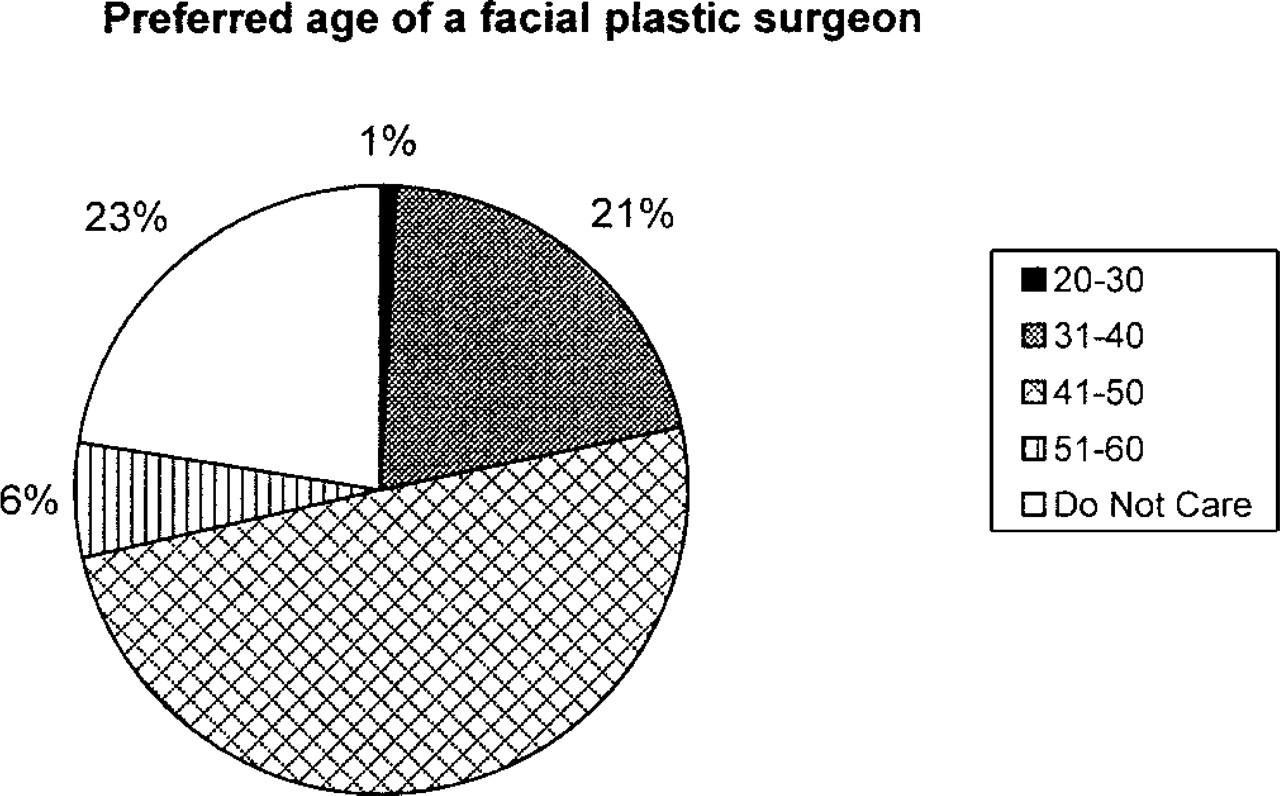
Preferred age group of facial plastic surgeons among medical students. The numbers in the legend represent years. Of the survey respondents, 49% preferred surgeons 41 to 50 years old.
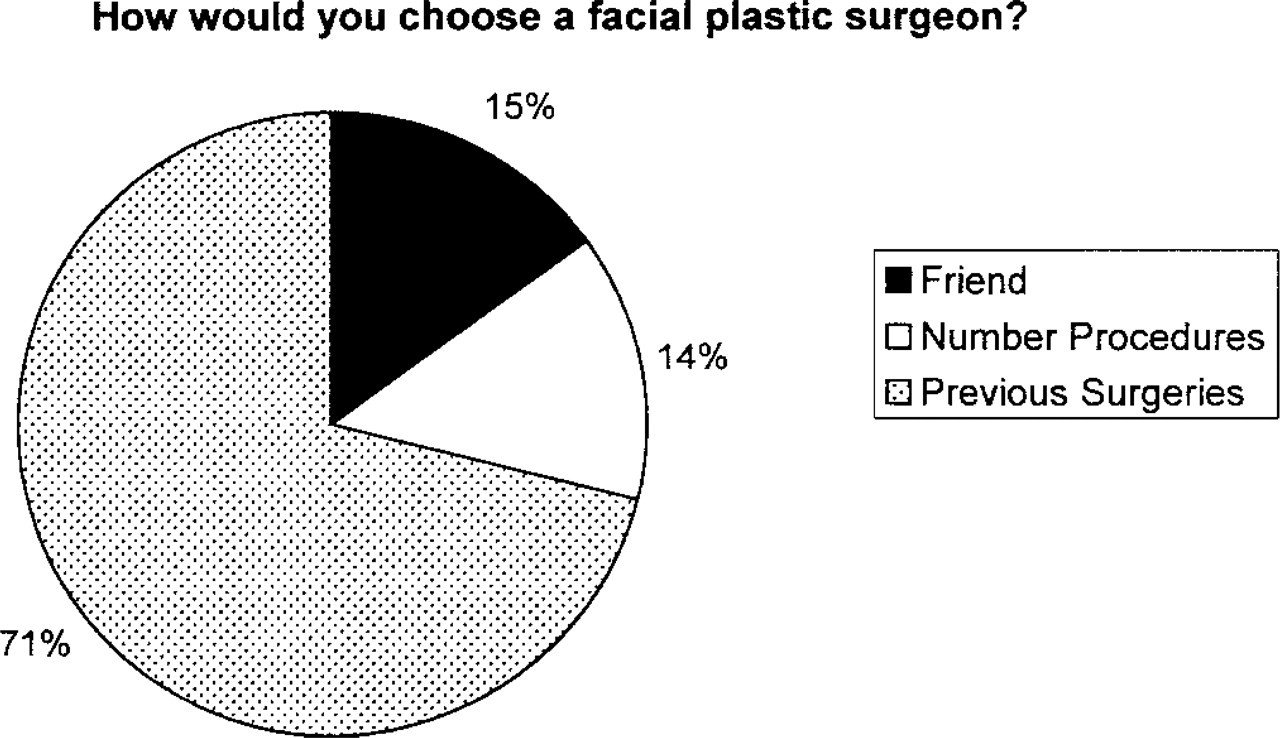
Criteria used by medical students to select a facial plastic surgeon. (Friend, recommended by a friend; number procedures, number of previous procedures performed; previous surgeries, results of previous surgeries performed.)
The survey was designed to be simple, easy to read, and nonintrusive with respect to personal information. At the top section of the questionnaire, there was a statement that there were no right answers to the questions asked. Survey responses were obtained by directly handing the questionnaire to the participating individuals.
RESULTS
A total of 339 individuals completed our survey with 217 from medical schools around the country and the remaining 122 respondents from the general public. There were 130 females and 138 males among the medical students from University of Michigan (33%), Georgetown University (33%), Oregon Health Sciences University (23%), and the University of Utah (11%). The students came from all 4 classes (Table 1) with an average age of 25.3 years. The general public was surveyed from southeastern Michigan (51%), Houston, Texas (25%), and the remainder from Portland, Oregon. Of this population, 58% were female and 93% had college degrees or better (Tables 1 and 2). The average age of this population was older than the medical student population (43.8 years old). The purpose of the “general population” survey was to compare the medical students with nonmedical, but well-educated people.
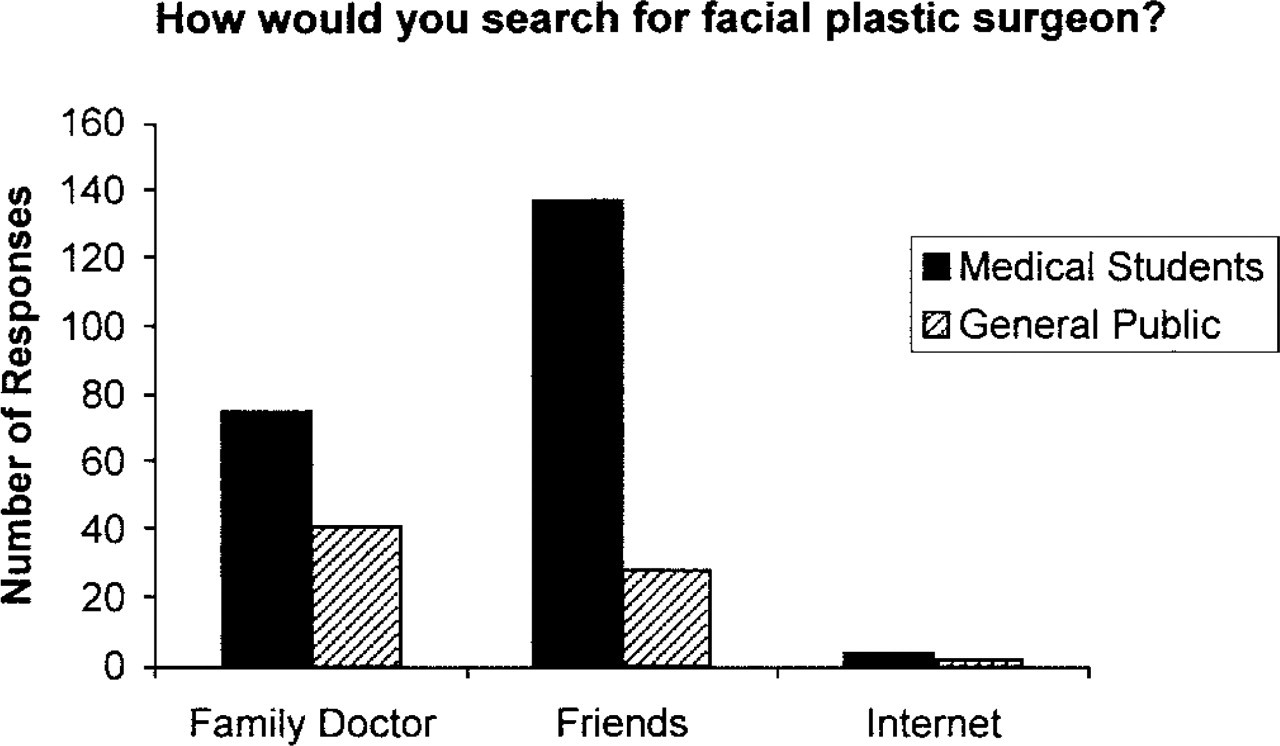
Influences in the search for a facial plastic surgeon.
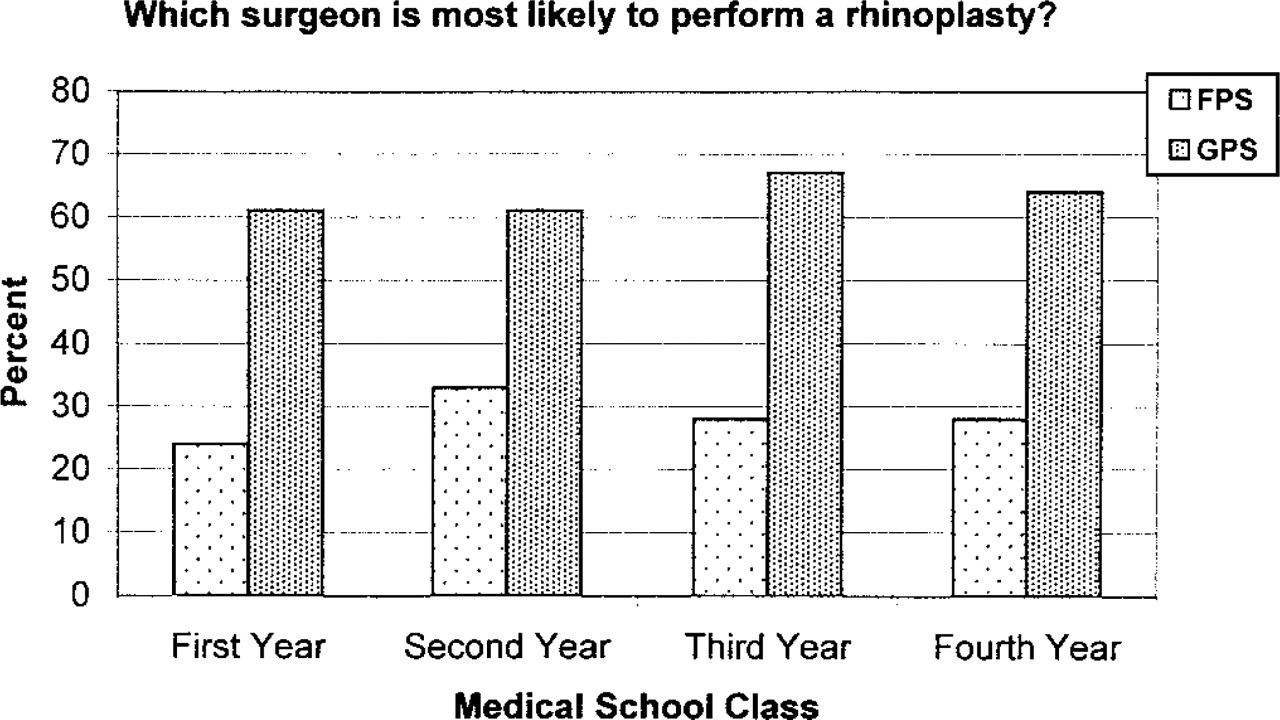
Choices by medical school students as to which surgeon is most likely to perform a rhinoplasty. There is little change over the years as medical students progress through their education. (GPS, general plastic surgery; FPS, facial plastic surgery.)
Most commonly selected choices in selecting a facial plastic surgeon
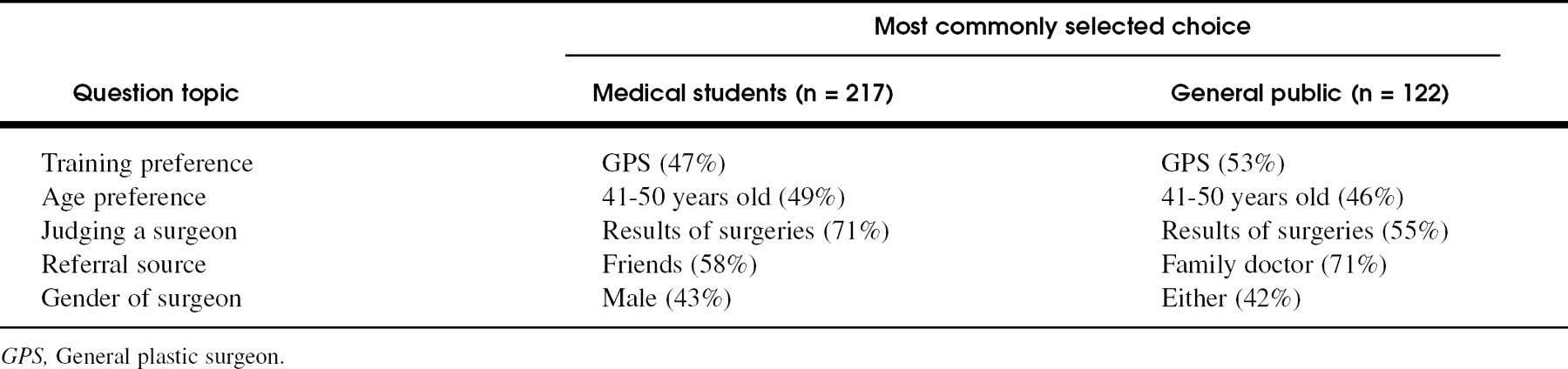
The survey was divided into 2 sections. The first asked what qualities the respondent would use to select a plastic surgeon. The second section asked what procedures were most commonly performed by various surgical specialties. When the general public was asked whom they would select to perform facial cosmetic procedures, most responded that they would prefer a plastic surgeon (46%), while others selected a maxillofacial surgeon (34%). The educated public and the medical students had similar responses (Table 3). The questionnaire showed that a male plastic surgeon between the ages of 41 and 50 was preferred (Fig 1) and would be judged on the result of previous surgeries (Fig 2).
Importantly, the majority of the public and a large percentage of the medical students would look to their family doctor for a referral (Fig 3).
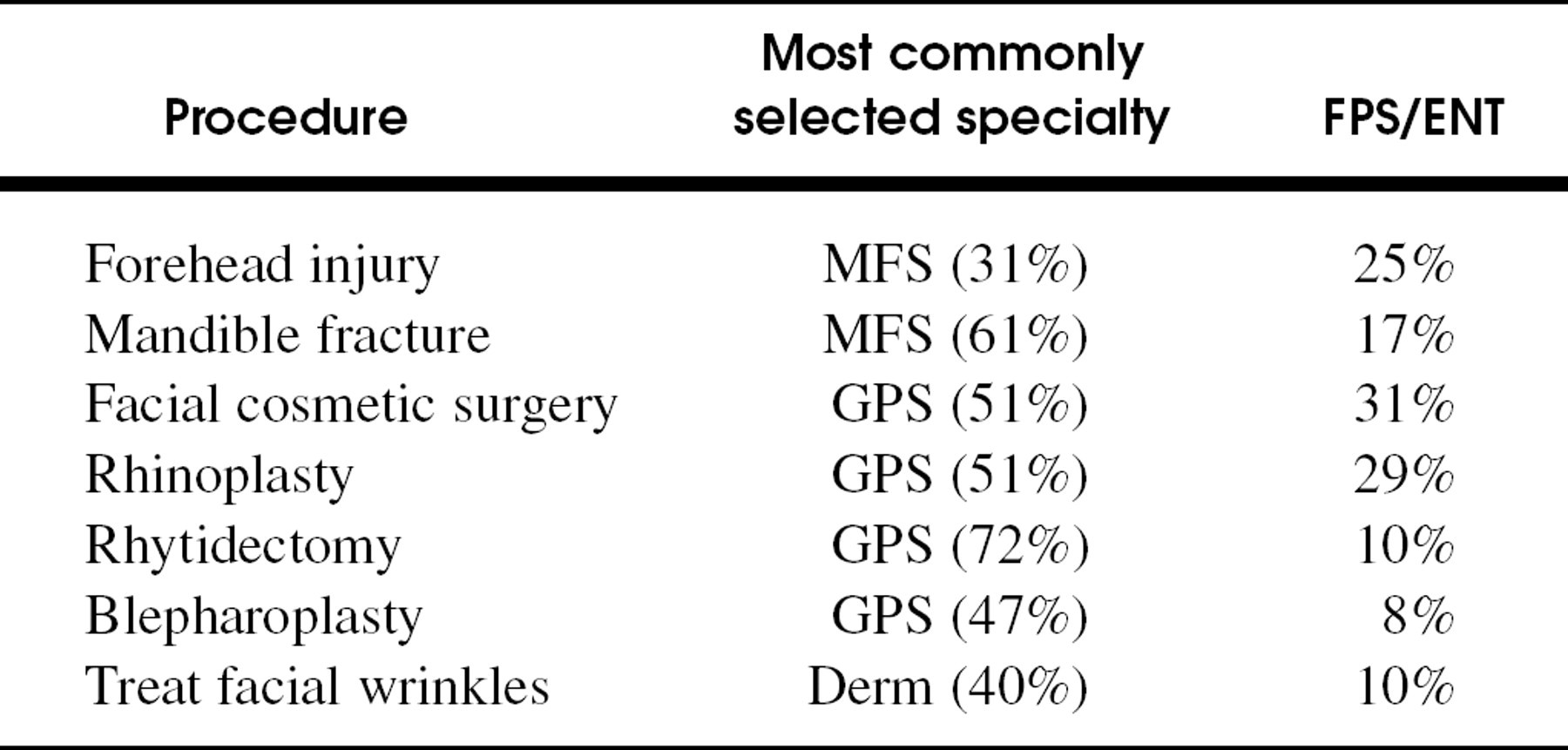
In the second section of the questionnaire, the survey asked which physician was most likely to perform a given procedure. The choices included oculoplastic surgeon, facial plastic surgeon, maxillofacial surgeon, general plastic surgeon, dermatologist, and “not sure.” When asked which physician is most likely to perform cosmetic surgery of the face, 33% responded FPRS (general plastic surgery, 54%), but when asked about specific procedures, the FPRS was consistently selected as less likely to perform rhinoplasty (Fig 4). General plastic surgery and dermatology were both selected as most likely to treat wrinkles of the face between both survey groups.
General plastic surgeons were consistently selected as most likely to perform rhinoplasty, 60% in the first and second year medical students and 62% in the second 2 years (Fig 4). Furthermore, although the fourth year students were less likely to select “not sure” than the first year students, there was not a significant difference between classes with regard to most choices. The most common answers for the public are listed with the percentages (Table 4). The percentages were similar between the 2 survey populations.
Responses from the general public as to who is most likely to perform procedures (oculoplastics, dermatology [Derm], facial plastic/ENT surgeon (FPS/ENT), maxillofacial surgeon [MFS], or general plastic surgeon [GPS]).
DISCUSSION
The goal of this study was to assess how medical students perceive the role of facial plastic surgeons. Understanding the role of the facial plastic and reconstructive surgeon in medical school is important so that students can refer patients properly as well as for selection of a residency. Survey results should help to direct medical school curricula and obtain a base line for future assessment.
Comparisons were made with a sampling of the well-educated public and between medical school classes. Surveys were collected from a well-educated group of adults to compare with the medical school population that have by definition finished college. The targeted distribution of the general public surveys was done to provide a basis for comparison of medical school student surveys. Given the small size, limited geographic area, and socioeconomic status of the general public respondents, this survey population should not be considered representative of the public perceptions across the country. Several different medical schools were targeted to assess the range of perception, and our efforts were focused on establishments where patrons were more likely to have cosmetic surgery performed (high-end retail stores).
The educated public and medical students had response rates that were similar (Table 5). The well-educated public was useful as a comparison to the medical students, although the number of surveys collected was smaller. In order to avoid institutional bias, several medical schools around the country were sampled. Because the numbers are small from each medical student class and follow-up surveys not yet completed, little can be said for certain about the changes in perceptions as students progressed through medical school. However, changes were within a few percentage points on most questions when the first 2 years were compared with the second 2 years of school. There also was a trend for first year students and the general public to select “not sure” or “I do not know” compared with the more senior medical students.
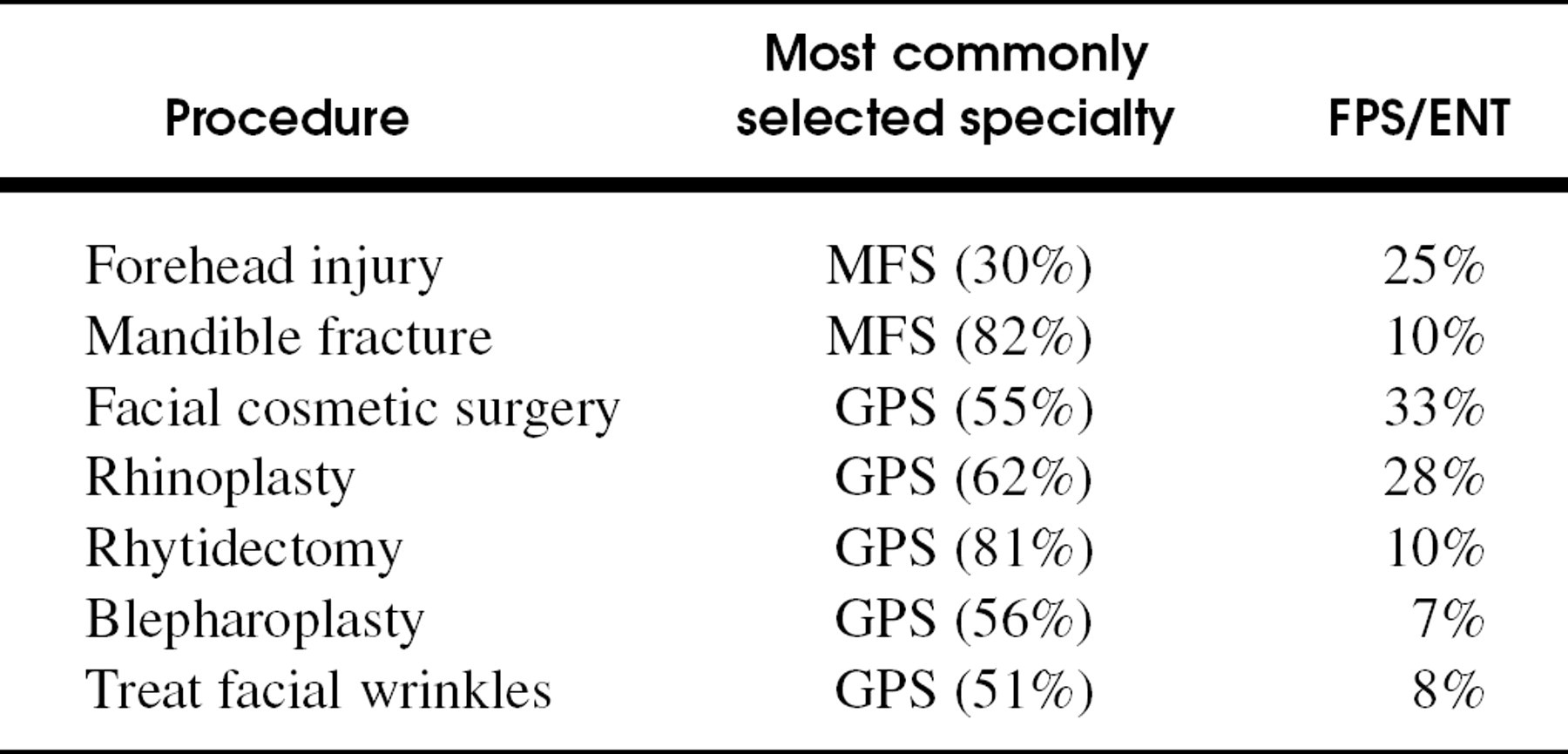
Responses from medical students as to who is most likely to perform procedure (oculoplastics, dermatology [Derm], facial plastic/ENT surgeon, (FPS/ENT) maxillofacial surgeon [MFS], or general plastic surgeon [GPS]).
Although there is no one specialty that should be considered as exclusive in performing aesthetic or reconstructive procedures, the facial plastic surgeon should be perceived at least as equal with other surgeons trained to perform these procedures. The survey results suggest that otolaryngologists and facial plastic and reconstructive surgeons are not perceived as experts in facial aesthetic and reconstructive surgery as compared with maxillofacial and general plastic surgeons. This is suggested by several findings of this study. First, similar responses were found among the general public and medical students. Second, general plastic surgery was chosen over facial plastic surgery for various procedures throughout the medical school classes. This was even true in procedures, such as rhinoplasty, that we expected to be the domain of otolaryngologists in most medical communities. Third, although the numbers of participants from within each class is not enough to reach significance, as medical students progressed through training, there was actually a shift toward selection of the general plastic surgeon. Initial perceptions on entering medical school were not altered, and those perceptions were similar to the general public with respect to who performs aesthetic facial procedures.
The goal of this study was directed at assessing the influence of otolaryngology education, specifically facial plastic and reconstructive surgery, among medical students. The results of this study suggest that facial plastic and reconstructive surgeons should play a larger role in medical education. Communicating the dedicated nature of the training in FPRS to medical students is important for the continued expansion of the specialty within medical community.
Over the past decade medical schools have made broad changes in the curriculum to focus classroom and clinical time on general practice or family-oriented medicine. There has been a concomitant trend toward de-emphasizing subspecialty involvement in the clinical medical school curricula. Academic otolaryngologists and facial plastic and reconstructive surgeons should continue to insist on playing a significant role in medical student education. Only through frequent positive pedagogic interaction with medical students at every level will the perceptions of medical school graduates change favorably for our specialty.