
Abstract
OBJECTIVE:
The study goal was to determine whether treatment of the tympanic membrane at the time of ventilation tube (VT) removal affects closure of the perforation.
STUDY DESIGN:
We conducted a retrospective chart review and telephone follow-up of children who underwent VT removal from 1995 through 1998.
RESULTS:
Among 109 patients (162 ears; 58% male), the mean age at VT removal was 6.7 years. Most VTs (59%) were T-tubes, and most (91%) were removed because of prolonged retention (mean 2.3 years). After VT removal, 111 ears (69%) received treatment, most commonly (44%) with 25% trichloroacetic acid (TCA). At the latest follow-up, 151 of the ears (93%) had healed without additional treatment. Treatment failure occurred more frequently in ears not initially treated with TCA (TCA 3% failure, other treatment 13%, no treatment 8%) and in ears with VTs removed because of otorrhea.
CONCLUSIONS:
Most perforations healed. TCA may promote closure, but a large randomized clinical trial is needed to eliminate physician bias.
Myringotomy with ventilation tube (VT) insertion is one of the most common surgical procedures performed in children. Although the placement of VTs decreases the incidence of acute otitis media, helps alleviate the symptoms of chronic middle ear effusion, and minimizes conductive hearing deficits resulting from chronic middle ear effusion, the procedure is not without risk. The formation of granulation tissue, tube extrusion into the middle ear space, cholesteatoma formation, external otitis media, and suppurative otitis media are some of the recognized complications. 1 In addition, defects can persist at the myringotomy site after tube extrusion or removal and result in a persistent perforation of the tympanic membrane (TM) and possible conductive hearing loss.
Previously, TM perforations after spontaneous or elective VT removal were not treated until the defect was deemed permanent, at which time tympanoplasty was considered. Now many surgeons treat the TM defect immediately after removing the tube. Treatments include freshening the edges of the perforation, paper patching, Silastic sheeting, patching with absorbable gelatin sponge or film (Gelfoam or Gelfilm; Pharmacia Corp, Peapack, NJ), bandage contact lens patching, and cauterization with trichloroacetic acid (TCA). 2 –6 The efficacy of these treatments, however, is debatable.
To better evaluate these options for the treatment of TM defects after VT removal at our institution, we compared the healing rates associated with observation alone with the healing rates after treatment with TCA, freshening the perforation edges, or patching the TM.
MATERIALS AND METHODS
By making use of the Mayo Clinic Surgical Information Recording System, we identified 135 patients (205 ears) between 0 and 17 years of age who had VTs surgically removed between January 1, 1995, and December 31, 1998. Of this group, 14 patients (24 ears) were excluded because of underlying medical conditions (cleft palate [n = 9], craniofacial deformities [n = 2], Down syndrome [n = 2], and Crouzon syndrome [n = 1]). Of the remaining 121 patients, 12 patients (19 ears) did not return for a follow-up visit and either could not be contacted or, when contacted during telephone follow-up, did not know whether the perforation had healed. The results presented here are from the 109 patients (162 ears) with sufficient postoperative follow-up.
Data collected included indications for VT insertion, findings at the time of insertion, site of VT placement, age at time of placement, and type of VT. In addition, the indication for surgical removal and the duration of VT retention were recorded. The type of treatment for the perforation at the time of surgical removal was indicated, as well as the presence of a perforation and subsequent treatments at the first and second follow-up visits. A history of adenoidectomy, allergies, or smoking in the home was also noted. Telephone surveys included data specific to treatments after operative VT removal and long-term follow-up.
For statistical analysis, the unit of analysis was an ear and the method of analysis accounted for the correlation between ears from the same patient. The outcome of interest was treatment failure, defined as the need for additional treatment after the initial treatment or the presence of a definite perforation or subtotal resolution at latest follow-up. The association between patient or clinical characteristics and treatment failure was evaluated univariately on the basis of fitting generalized estimating equation models by use of SAS software for the procedure PROC GENMOD (SAS Institute, Cary, NC). 7 An exchangeable correlation structure was specified to account for the correlation between the ears in patients who had VTs removed from both ears.
RESULTS
There were 109 patients, 63 boys (57.8%) and 46 girls, who had VTs removed in the operating room at our institution between January 1995 and December 1998. Fifty-three patients (48.6%) had VTs surgically removed from both ears; 27 (24.8%) from their right ear only, and 29 (26.6%) from their left ear only. The mean age at VT removal was 6.7 years (range 1.5–17.0 years). Fifty-seven VTs were inserted at other institutions, with the date of placement not available. In the remaining 105 ears, mean VT retention was 2.3 years (range 0.2–8.7 years).
Designs of the 162 VTs removed were as follows: 96 (59.3%) were T-tubes; 19 (11.7%), Paparella; 4 (2.5%), Shepard; 5 (3.1%), Armstrong; and 38 (23.5%), either unknown or another type. The most common indication for VT removal (90.7%) was prolonged retention (Table 1); of these, 64.6% had been in place at least 2 years. Of all VTs, 2% were in place for <6 months, and all VTs removed before 6 months were removed because of chronic otorrhea. At the time of VT removal, perforations in 111 of the ears (68.5%) were treated, primarily with TCA (43.8%).
Indications for ventilation tube removal
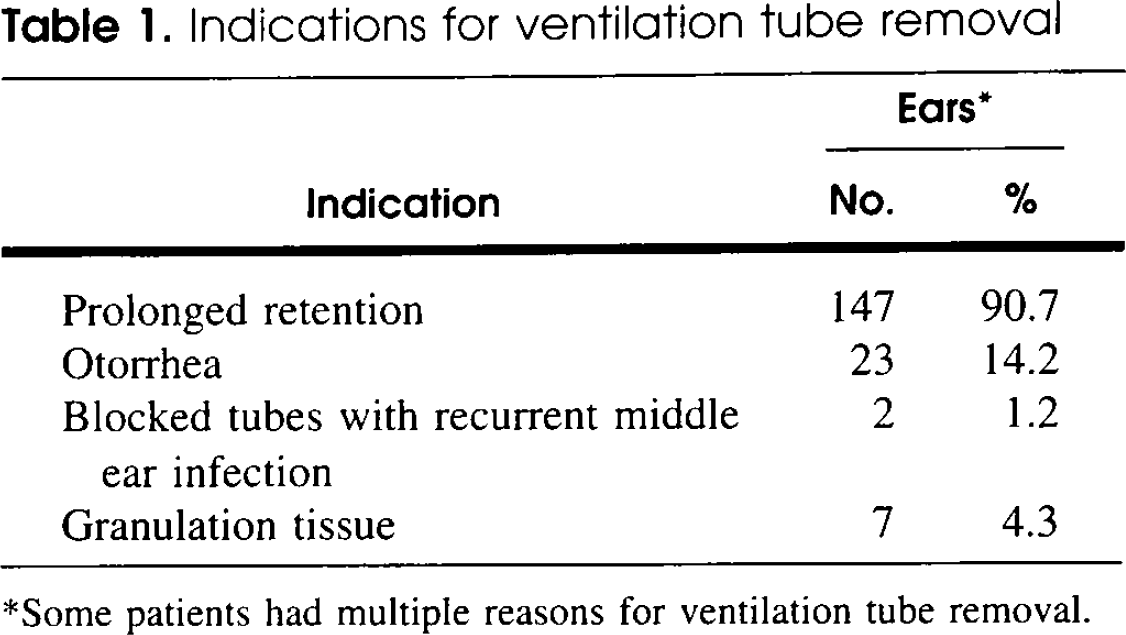
Some patients had multiple reasons for ventilation tube removal.
At latest follow-up (the date the perforation was noted to be healed or, if the perforation was still present, the latest known follow-up), 151 of the ears (93.2%) had healed after initial treatment. Six patients (7 ears) received additional treatment during follow-up (Table 2); presumably, the initial treatment failed. An additional 4 patients (4 ears) were known to have perforations at latest follow-up (Table 3), and these were also considered treatment failures. In total, initial treatment failed in 10 patients (11 ears). All failures occurred in patients with T-tubes (6 ears) or with an unidentified type of tube (5 ears).
Patients with initial treatment failure, defined as requiring a second treatment
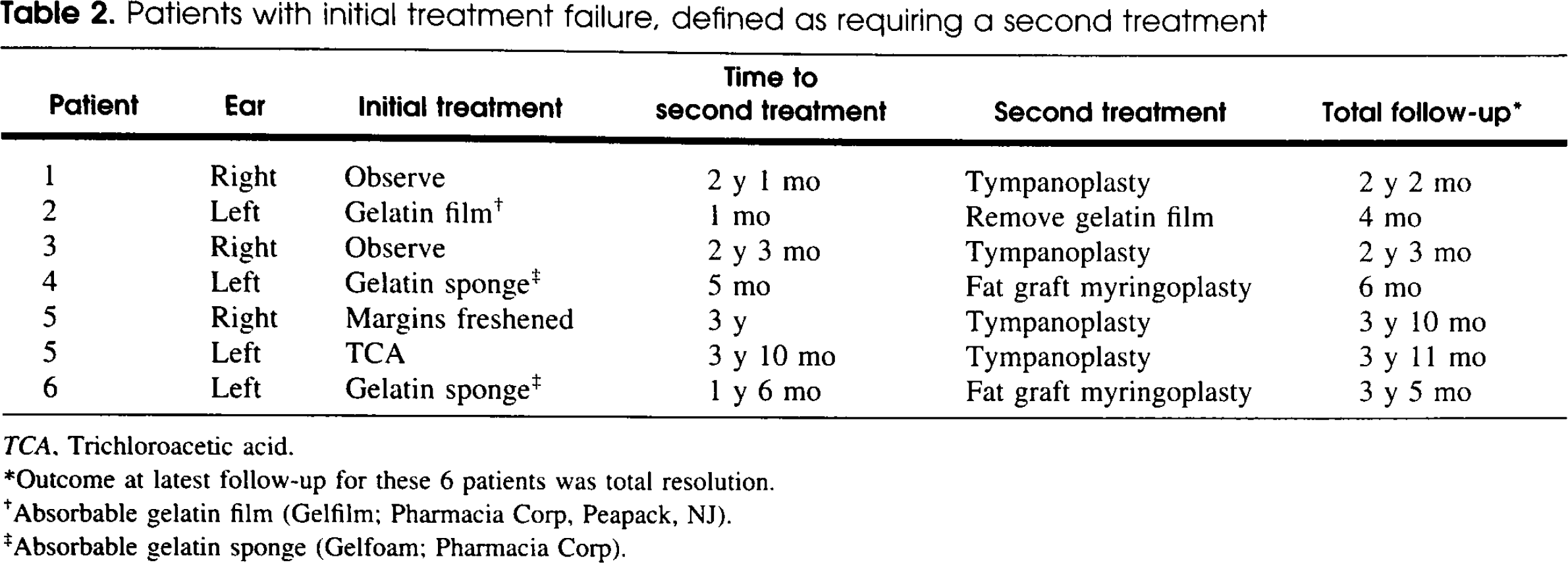
TCA, Trichloroacetic acid.
Outcome at latest follow-up for these 6 patients was total resolution.
Absorbable gelatin film (Gelfilm; Pharmacia Corp, Peapack, NJ).
Absorbable gelatin sponge (Gelfoam; Pharmacia Corp).
Patients with initial treatment failure, defined as subtotal resolution of the perforation or a definite perforation present at latest follow-up
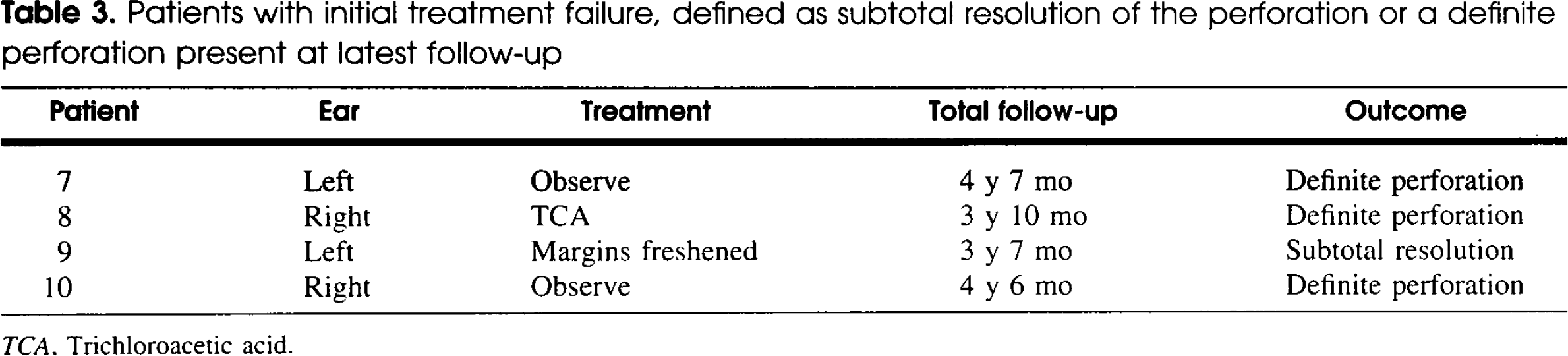
TCA, Trichloroacetic acid.
The presence of purulent, serous, or mucoid effusion did not influence healing of the perforation. Smoking in the home, previous adenoidectomy, adenoidectomy at VT placement, and allergies did not influence healing. In addition, the site of VT placement, reason for VT removal, reason for VT placement, patient's age at the time of VT placement, and duration of VT retention in the ear were not related to treatment failure, as none of these factors were statistically significant (Table 4). A history of having had a VT was significantly associated with treatment failure. Of the 88 ears with no previous VTs, there were 2 failures (2.3%), compared with 5 failures (9.4%) in ears with 1 previous VT (P = 0.09) and 4 failures (19.0%) in ears with ≥2 previous VTs (P = 0.02).
Association between clinical and patient characteristics and treatment failure*
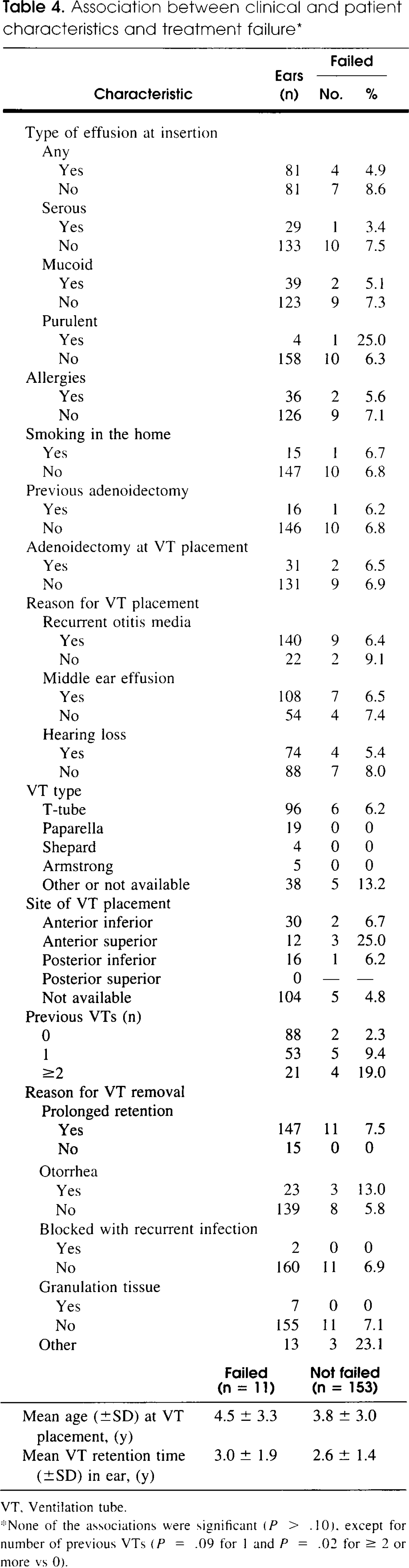
VT, Ventilation tube.
None of the associations were significant (P > .10). except for number of previous VTs (P = .09 for 1 and P = .02 for ≥ 2 or more vs 0).
There was no statistically significant association between type of initial treatment and healing (Table 5). However, ears treated with TCA tended to have a better outcome than ears receiving other treatments or no treatment (failure rate 2.8% vs 9.9%, P = 0.078).
Association between type of initial treatment and treatment failure*
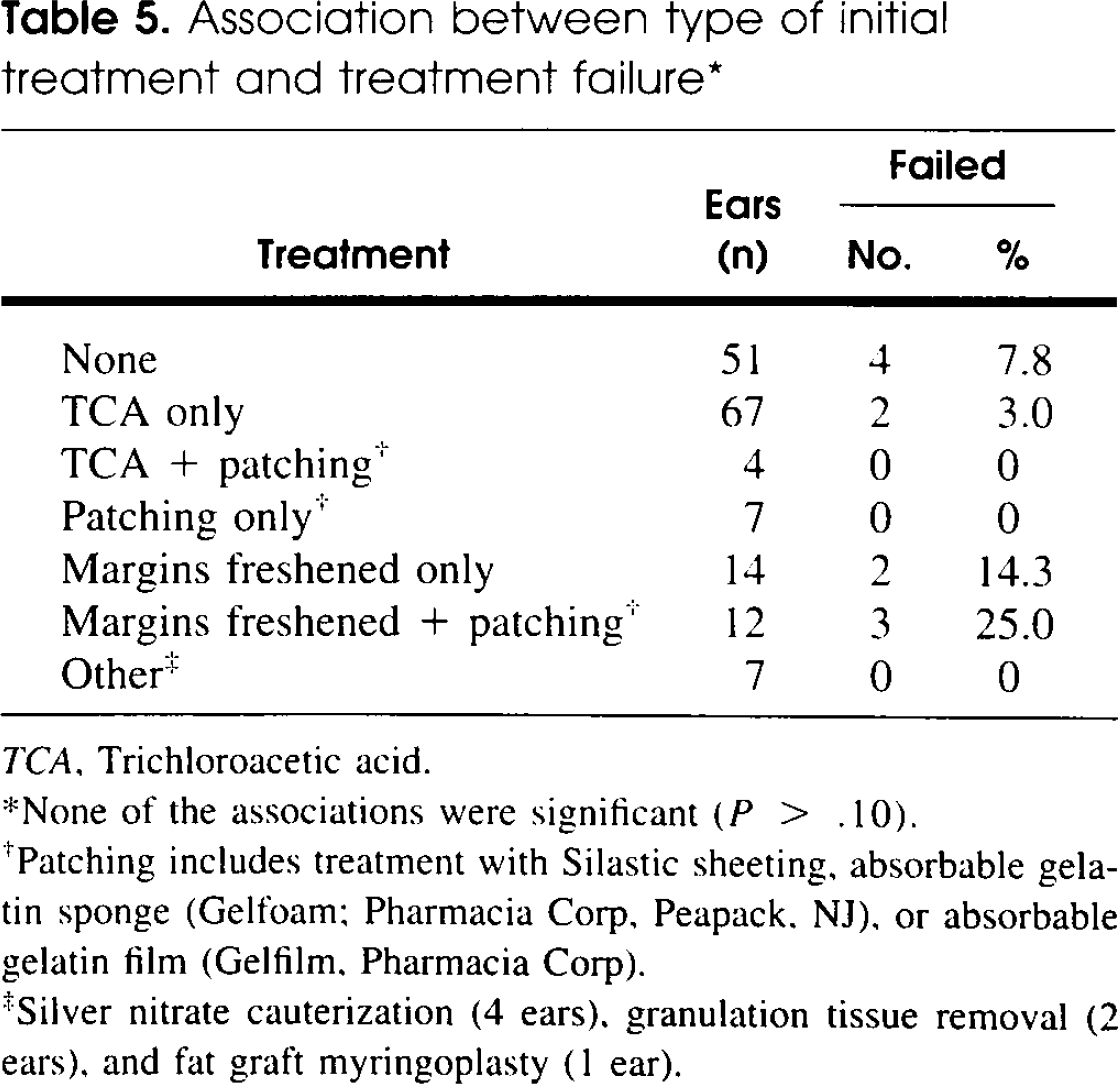
TCA, Trichloroacetic acid.
None of the associations were significant (P > .10).
Patching includes treatment with Silastic sheeting, absorbable gelatin sponge (Gelfoam; Pharmacia Corp, Peapack. NJ), or absorbable gelatin film (Gelfilm. Pharmacia Corp).
Silver nitrate cauterization (4 ears), granulation tissue removal (2 ears), and fat graft myringoplasty (1 ear).
DISCUSSION
Although VT removal is a common procedure, there is no consensus as to the best treatment of the resulting perforation. Various factors have been reported that may influence whether the defect heals or remains patent. It is widely accepted that the type of VT plays a role, with longer lasting T-tubes resulting in more persistent defects than short-term VTs. These rates range from 3% to 47.5% for T-tubes compared with a 0.5% to 2% perforation rate for short-term VTs. 8 –14 Our study supports these findings, because no persistent perforation was associated with short-term VTs (Table 4). Surgical placement of the VT may also play a role. Oluwole and Mills 15 reported an increased rate of persistent perforation when VTs were placed in an anteroinferior position with the TM. An increased risk of persistent perforation has also been reported in patients younger than 5 years when otorrhea occurs while the VTs are in place and in patients with a history of adenoidectomy. 14,16,17 In addition, there is no agreement as to whether elective surgical removal of VTs or spontaneous extrusion results in a higher rate of residual perforation. We were unable to identify other factors besides the number of previous VT placements that were associated with treatment failure 16,18 –20 (Table 4).
Although permanent perforation may be a desirable outcome for some patients, because it allows prolonged middle ear ventilation, a conductive hearing loss may result, the amount of which increases with the size of the defect. 1,15,17 Patients with TM defects are also at risk of middle ear infections associated with swimming and bathing, and migration of the squamous epithelium onto the medial surface of the TM may increase the risk of future cholesteatoma formation. 21,22 Therefore, it is usually desirable to close the perforation after spontaneous extrusion or surgical removal of VTs. However, it is unclear whether the TM should be actively treated to encourage closure or the defect should simply be observed and allowed to close on its own.
Therapy for TM perforations theoretically improves healing on the basis of principles outlined by Saito et al, 23 who suggested that breaking the stratified squamous epithelium covering the edge of the perforation, stimulating TM growth by creating an inflammatory reaction, and preventing epithelium ingrowth over the perforation margin by providing a bridge may help the defect to repair itself. Patching provides a bridge to promote repair, freshening the perforation margins breaks the epithelial cover that can inhibit defect closure, and agents such as TCA create an inflammatory reaction at the edges of the hole. None of these treatments alone accomplishes all 3 goals.
Many treatments have been described and applied at the time of VT removal. For example, patching the defect with Silastic sheeting, paper, absorbable gelatin sponge or film, or bandage contact lens to encourage healing has been advocated. However, results have been mixed. Nichols et al 3 found that paper patching did not improve perforation healing rates, and Pribitkin et al 24 found that paper patch myringoplasty significantly improved the outcome in ears with >3 previous VT insertions. Other studies have advocated the use of absorbable gelatin film for patching, and others claim that Silastic sheeting speeds up the repair process and decreases the rate of persistent perforation 4 Few studies, however, corroborate these findings.
TM patching was not a common treatment at our institution, with only 13.0% of the ears in our study population receiving an absorbable gelatin sponge or film patch and 2.5% of the ears receiving other patching material. We found that patching the TM did not significantly improve the final outcome of patients (ie, it did not increase the likelihood of the perforation healing completely).
Freshening the edges of the perforation, which involves excising the margins with a surgical instrument, has also been reported to increase the healing rate. 2 Also, faster healing rates have been noted in ears with a traumatic perforation edge at the time of operation. 2 In our study, 16% of the ears had their perforation margins freshened, without a significant increase in TM healing (Table 5).
The most frequent treatment in our patient population was cauterization with TCA. Immediately after VT removal, 25% TCA was applied to the edges of the perforation. Although published studies discussing TCA treatment after operative VT removal are scarce, the use of TCA is prevalent at our institution (43.8% of patients in our study). Pribitkin et al 24 reported that TCA used with paper patching may induce regeneration but did not discuss the use of TCA alone. In our study, patients treated with TCA appear to have a lower occurrence of persistent perforation (3% failure with TCA vs 13% with other treatment and 8% with no treatment), but because of the small number of patients with a perforation that did not heal initially, the results are not statistically significant (Table 5).
CONCLUSION
Most children undergoing VT removal in the operating room experience complete healing of the resultant perforation (93% in our study). For the remaining children, it remains unclear whether specific initial treatments promote healing of the defect at the site of VT removal. Our results suggest that TCA may promote this healing. However, so few patients experience permanent perforation that statistical significance is difficult to demonstrate. A large, randomized clinical trial is needed to identify a sufficient number of treatment failures to have acceptable statistical power and to eliminate physician bias.