
Abstract
OBJECTIVE: Our study goal was to study fungus-specific immunoglobulins G (sIgG) and E (sIgE) in polypoid rhinosinusitis with and without evidence of allergic fungal rhinosinusitis (AFS).
STUDY DESIGN AND SETTING: A prospective analysis was conducted of fungal sIgG and sIgE using a 9-mold RAST panel in 13 AFS, 11 AFS-like, and 27 non-AFS polypoid rhinosinusitis patients. Nonpolyp controls included 17 volunteers with allergic rhinitis and 11 with no atopic history.
RESULTS: All groups had elevated fungal sIgG levels. Polyps, increasing polyp severity, and AFS were associated with elevated fungal sIgG to a greater number of molds. The AFS group had sIgE elevations (≥class II) to an average of 5 molds versus only 0.1 in the non-AFS polyp group. Total IgE was 971 U/mL versus 64 U/mL, respectively.
CONCLUSIONS: Multiple elevations of fungal sIgE are adequate diagnostic evidence of these fungi when fungal cultures and histologic examinations are negative in diagnosing AFS. The significance of increased fungal sIgG remains unclear.
SIGNIFICANCE: Early recognition of AFS may be facilitated by screening polypoid rhinosinusitis patients with total serum IgE and RAST testing.
The teleologic origin of AFS has remained elusive since it was first recognized more than 20 years ago. Marple's 1 2001 review provides an excellent and thorough overview of the subject. Whereas it has been estimated to occur in approximately 7% of patients undergoing surgery for chronic rhinosinusitis (CRS), the disease often remains unrecognized in its early stages. 2 The exact pathophysiology remains unknown, and it is a subject of ongoing investigation and controversy. A preponderance of evidence suggests that an IgE-mediated process is involved in the pathogenesis of AFS. 3–5 Whether this is the primary factor in the pathogenesis, or merely the consequence of another, is still not certain.
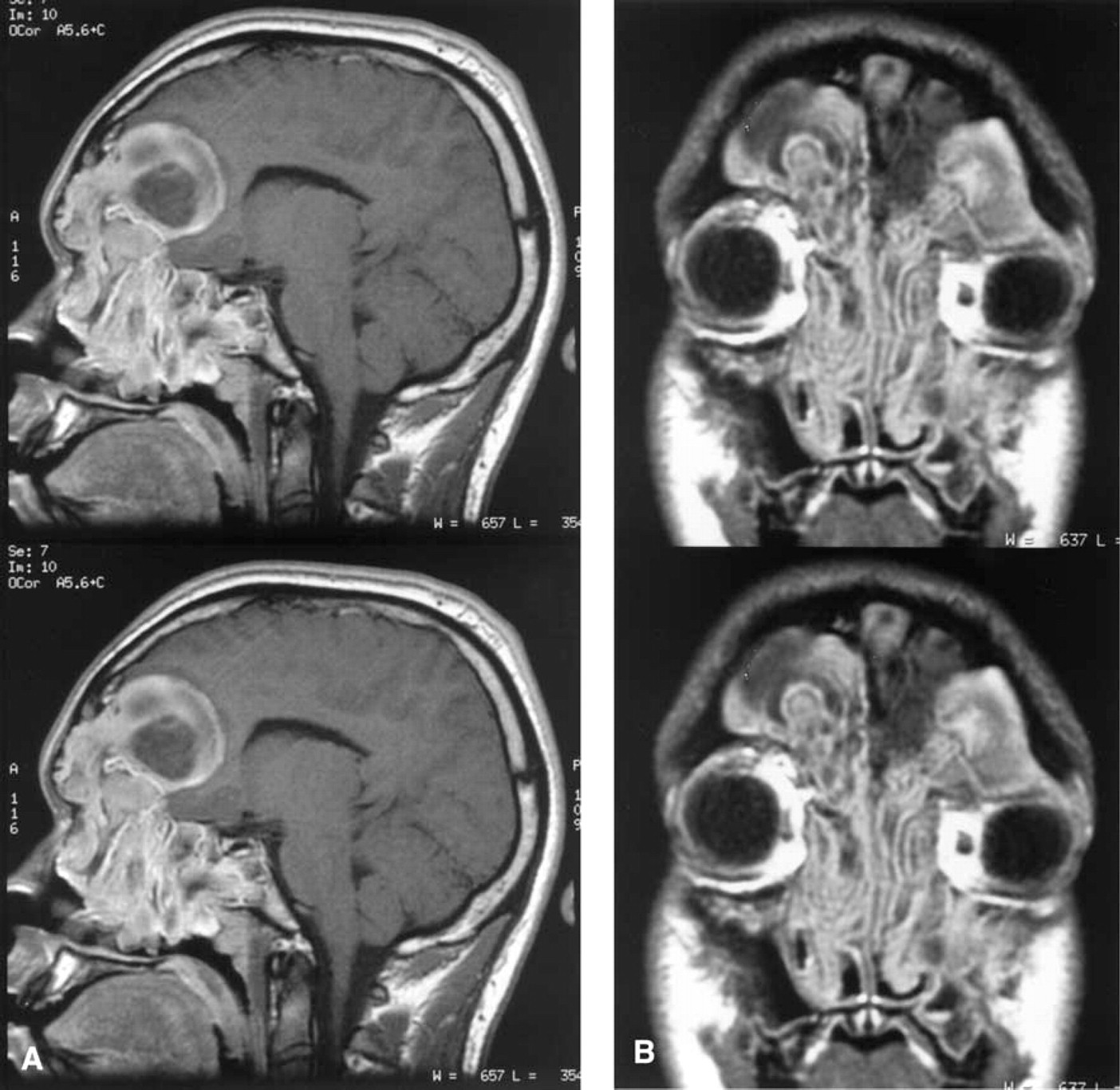
Various sets of basically similar diagnostic criteria have been suggested and used. 4,6,7 The traditional gold standard criterion has been the demonstration of allergic mucin and noninvasive fungi from a patient with polypoid CRS. It is during the early stages when it is most difficult to distinguish the subset of patients with polypoid CRS that have AFS. Unfortunately, most laboratories have difficulty in consistently demonstrating the involved fungi by standard culture and staining techniques. Due to these difficulties and the possibility of a saprophytic contaminant, some authors have specifically abandoned this as a required criterion. 8 The histologic demonstration of allergic mucin and noninvasive fungal elements is still required, although often equally difficult unless deliberate sampling techniques and special stains are used. Collection of the gross allergic mucin and communication with the pathologist are essential in maximizing the chances of accurate and consistent diagnosis. Polymerase chain reaction, in situ hybridization, DNA probes, and novel methods for specimen collection and analysis have been used to try to overcome some of these difficulties. 9–12 These assays and methods as a whole are indeed significantly more sensitive and specific in isolating and identifying fungi than conventional fungal culture and staining techniques. However, in the absence of allergy, or rather specific IgE antibodies to these fungi, these tests are not diagnostic of what is generally known to be AFS. The mere presence of fungi within the nose and sinuses does not appear to cause AFS. The pathogenesis is likely multifactorial, but the key appears to be related to the susceptible individual's hyperimmune response to these fungi. A test that could demonstrate this response and the inciting fungi would be ideal. It would also facilitate earlier diagnosis, referral, and treatment, which would help avoid the potentially destructive effects of advanced AFS (Fig 1.). As a simpler means of accomplishing this, serum fungal sIgG and sIgE can be measured by radioallergosorbent test (RAST). In vitro testing via modified RAST is an accepted standard in screening and diagnosing inhalant allergy, including molds. 13–15 Unfortunately, there have been no controlled studies to examine the diagnostic efficacy of these values for AFS.
Sagittal
In allergic bronchopulmonary aspergillosis (ABPA), there are elevations of fungal sIgG, which are associated with a type III Gel and Coombs reaction (immune complex reaction). This has led to the supposition of a similar role in AFS, but this remains speculative.
In review of the literature, elevations of sIgG and sIgE are often referred to as a characteristic of AFS, but there are actually relatively few reported cases that document this finding. 3,16–21
This pilot study serves to investigate sIgG and sIgE using RAST in a spectrum of patients including nonatopic controls, non-AFS polypoid CRS, AFS-like, and AFS subjects. Our results are consistent with previous studies that show elevated sIgE to multiple fungi in AFS patients. This suggests that this finding in a patient with polypoid CRS and allergic mucin is adequate to establish a diagnosis of AFS in the absence of a positive fungal culture or stain.
METHODS
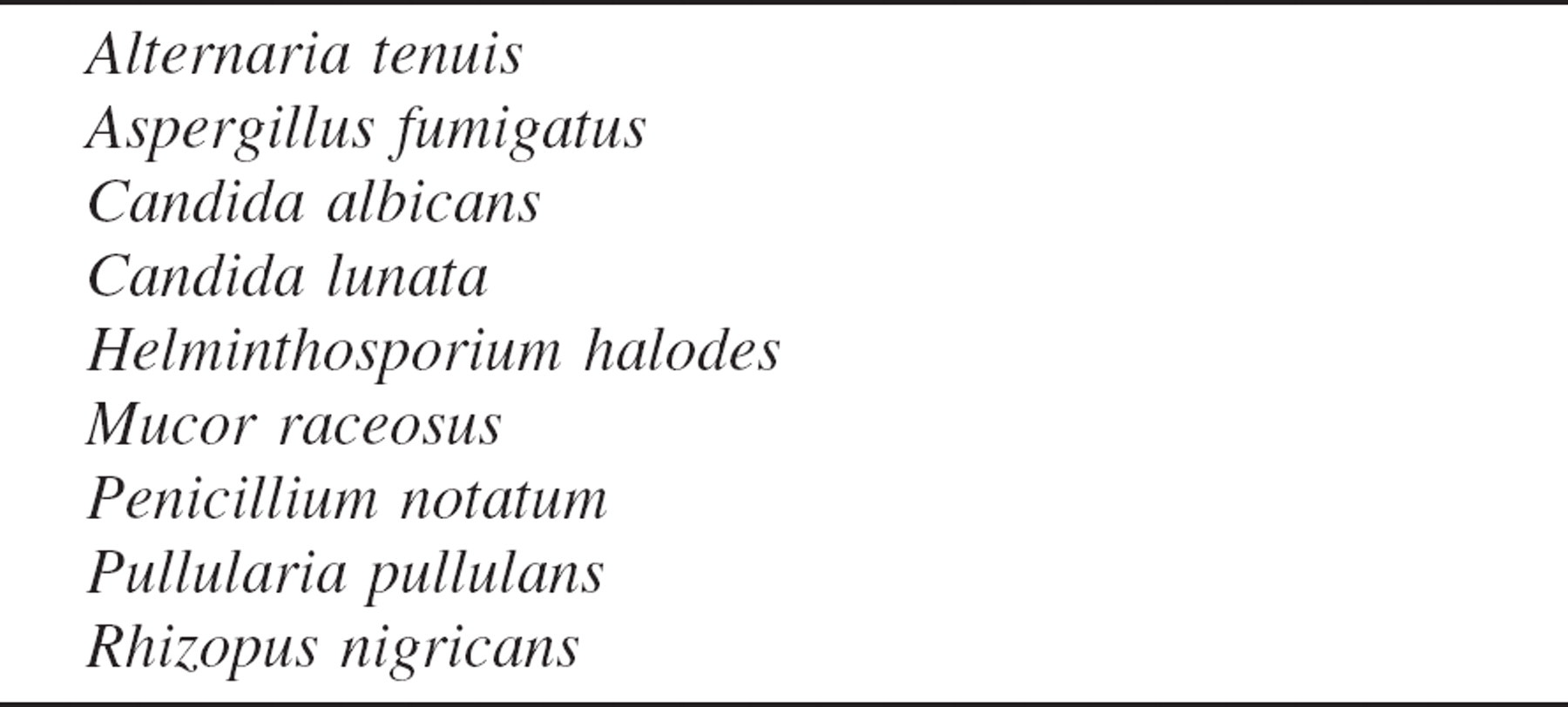
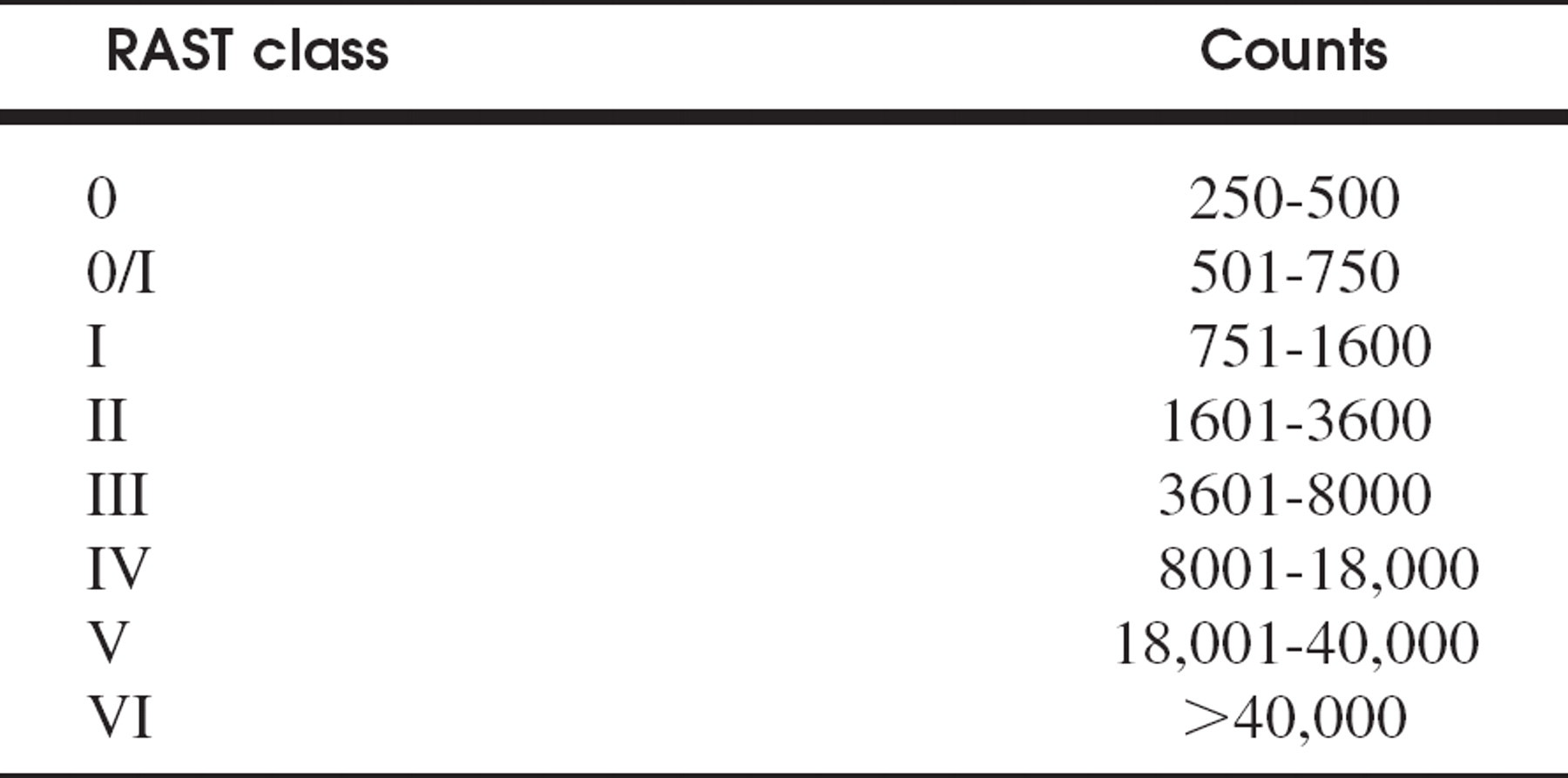
This institutional review board-approved study was conducted at a tertiary care military treatment facility. The majority of patients included in this 1993–1994 study are from the original protocol to study the pathophysiology of AFS and the impact of immunotherapy. During this period, consecutive consenting patients undergoing surgery for polypoid CRS, including those suspected of having AFS, were included. Since 1997, data from additional AFS patients have been included. Serum was examined for total IgE and for fungal sIgG and sIgE by modified RAST versus 9 fungi reported to cause AFS (Table 1).
Specimens from surgery were examined for evidence of allergic mucin and noninvasive fungal elements and were submitted for fungal culture. Thirteen patients were diagnosed with AFS based on the demonstration of allergic mucin both grossly and histologically and a positive fungal culture or stain. Allergic mucin is defined as lamellated sheets of eosinophilic mucin with eosinophils in various stages of degeneration, with or without Charcot-Leydon crystals. These patients also had characteristic radiographic findings on computed tomography scanning and, in some cases, magnetic resonance imaging. These included a unilateral predominance of disease, often with expansion of the involved sinuses, and serpiginous high-attenuation areas on computed tomography corresponding to the allergic mucin interspersed among the polyps. Eleven were highly suspected of having AFS but had negative fungal stains and cultures or no histologic evidence of allergic mucin, despite the presence of gross allergic mucin at surgery. Gross allergic mucin is defined as thick, green-to-brown material of peanut butter consistency interspersed among the polyps. Table 2 summarizes the characteristics of these patients.
Nine-mold RAST panel
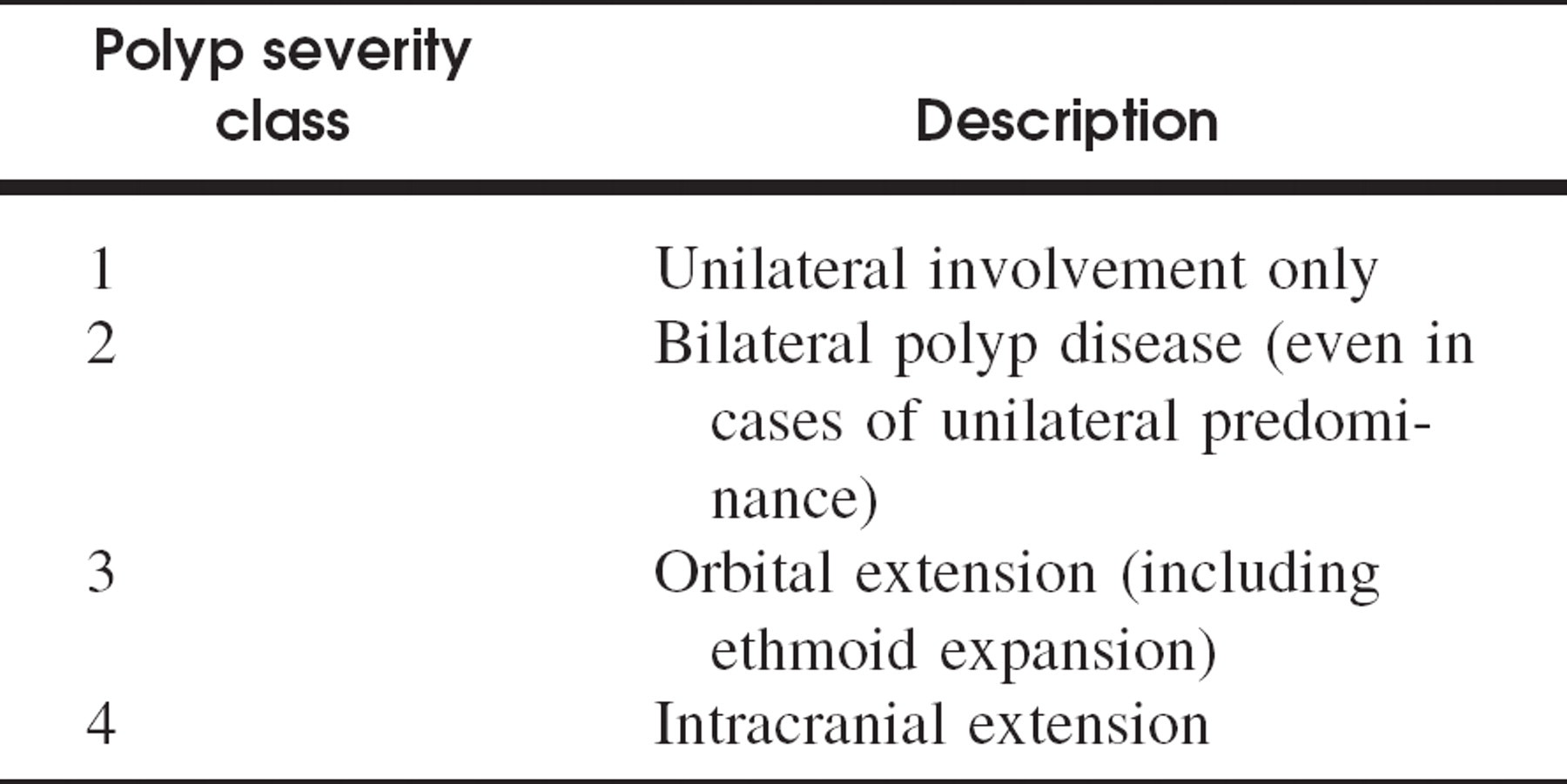
These 24 AFS and AFS-like patients were compared with 27 patients with non-AFS polypoid CRS. Non-AFS polyp patients had no evidence of allergic mucin, negative fungal cultures/histology, and negative fungal skin testing (if done) and lacked characteristic radiographic findings. Polyp severity was also graded and compared based on a scale used by the senior author (D.H.H). (Table 3). Controls included 11 nonatopic volunteers and 17 additional volunteers who reported a history of allergic rhinitis but had no stigmata of polypoid CRS.
Different laboratories were used during the study period to perform RAST testing (Allergy Testing Laboratory [now Esoterix], Brentwood, TN, and Commonwealth Medical Laboratories, Fairfax, VA). The standardized scoring system for the Fadal/Nalebuff modified RAST was used to classify sIgE (Table 4).
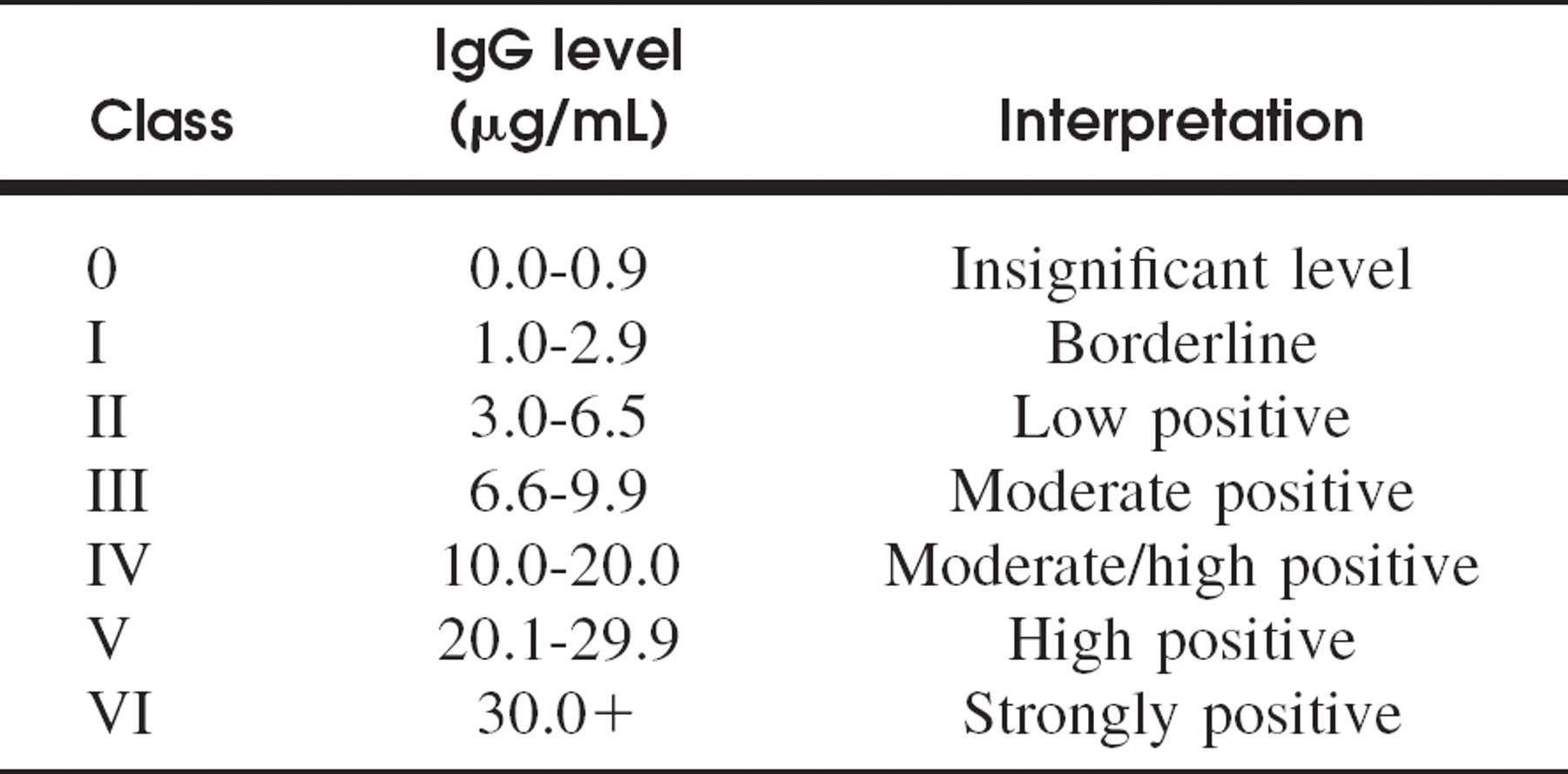
For sIgG, different scales were used. Table 5 shows the one currently used. We used the commonly accepted standard of considering a class II or higher score as clinically significant for sIgE. There are no data on what constitutes a clinically significant sIgG level in AFS, so both class II and class III cutoffs were considered separately. RAST and total IgE results were compared among the different patient groups as well as according to polyp severity.
AFS-like patient group
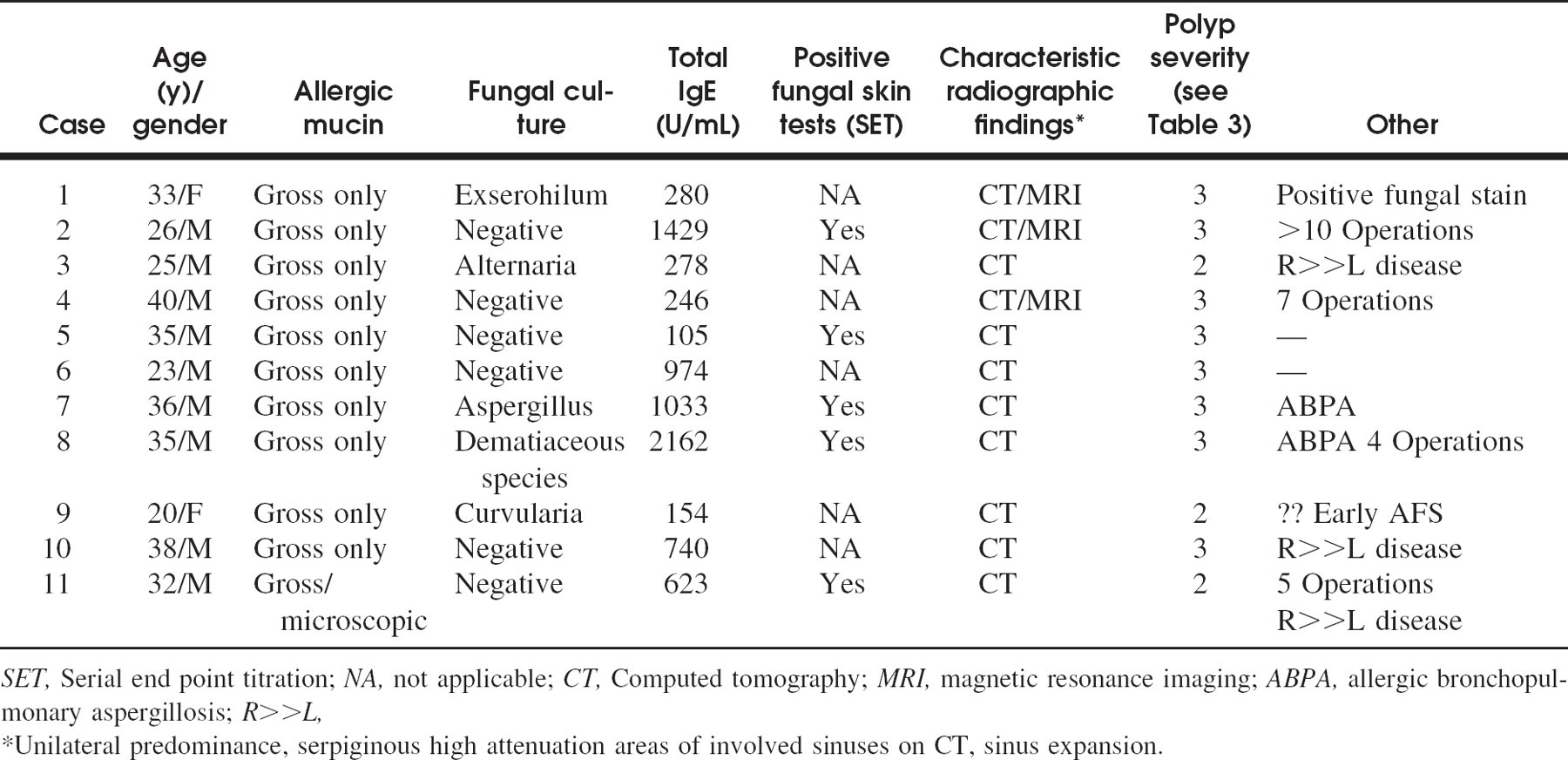
SET, Serial end point titration; NA, not applicable; CT, Computed tomography; MRI, magnetic resonance imaging; ABPA, allergic bronchopulmonary aspergillosis; R>>L,
Unilateral predominance, serpiginous high attenuation areas of involved sinuses on CT, sinus expansion.
Polyp severity classification
Fadal/Nalebuff modified RAST 32
Specific IgG: Esoterix laboratory
Overall significance values were tested by Kruskal-Wallis method. For each group, multiple comparison tests were carried out as rank-sum tests using the Bonferroni approach for selecting P values.
RESULTS
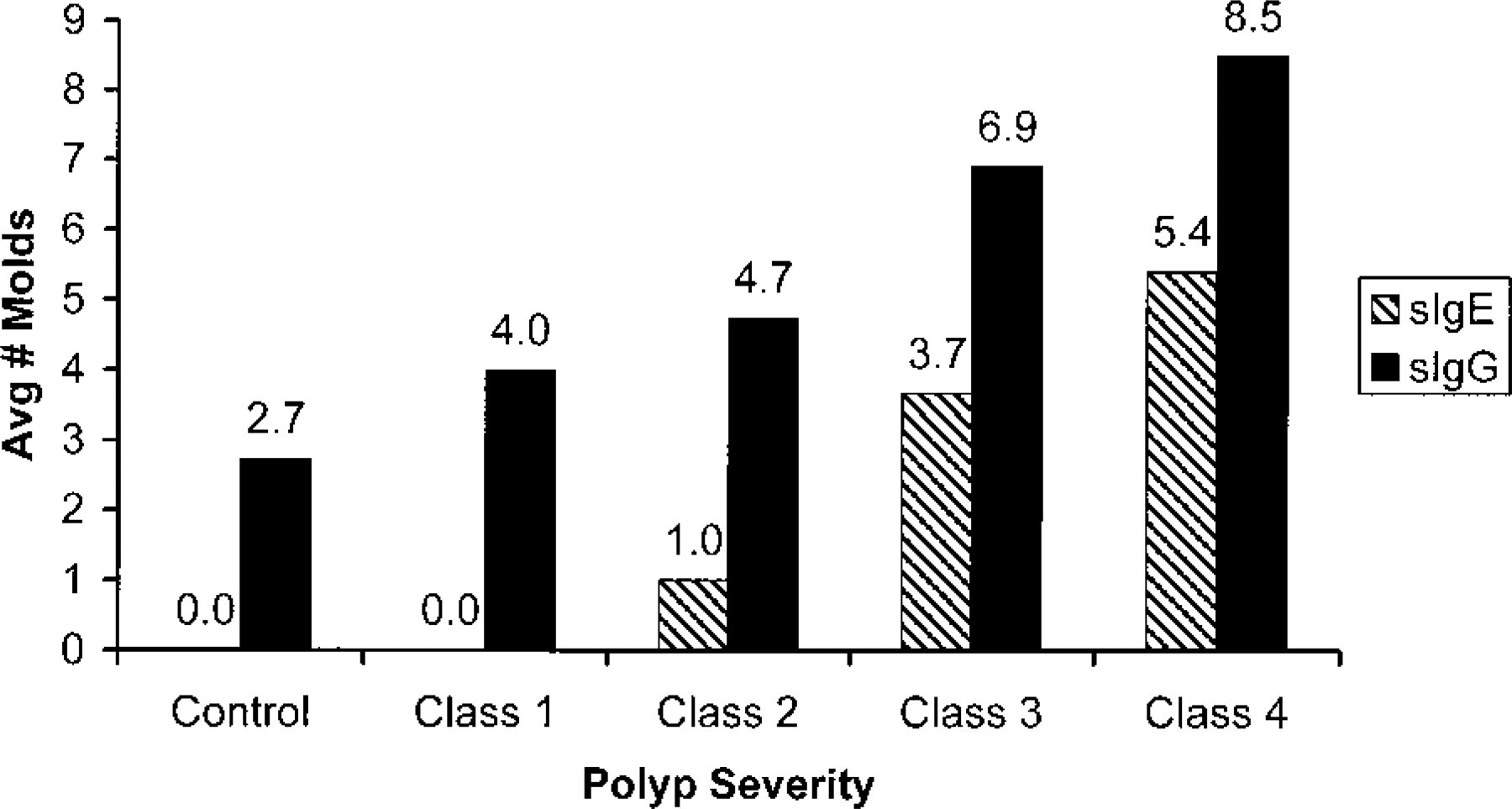
Fungal sIgG and sIgE were evaluated in 2 ways. Figure 2 considers a RAST class II and higher as a significant score. Figure 3 considers only RAST class III and higher as significant. The number of fungi (of the 9 tested) with a significant RAST score was summed for each patient and then averaged for each patient group.
Patients in the AFS and AFS-like groups demonstrated elevations of both sIgG and sIgE to multiple fungi. AFS patients had significant elevations of sIgE (class II and higher) to an average of 5.0 of the 9 fungi tested compared with 3.4 in the AFS-like group and only 0.1 in the non-AFS polypoid CRS group (Fig 2.). There were significant differences between the non-AFS polypoid CRS group compared with the AFS and AFS-like groups (P < 0.001, P < 0.001) but not between the AFS and AFS-like group (P = 0.136). This pattern was duplicated when only sIgE class III and higher elevations (Fig 3.) were considered (P < 0.001, P < 0.001, P = 0.752).
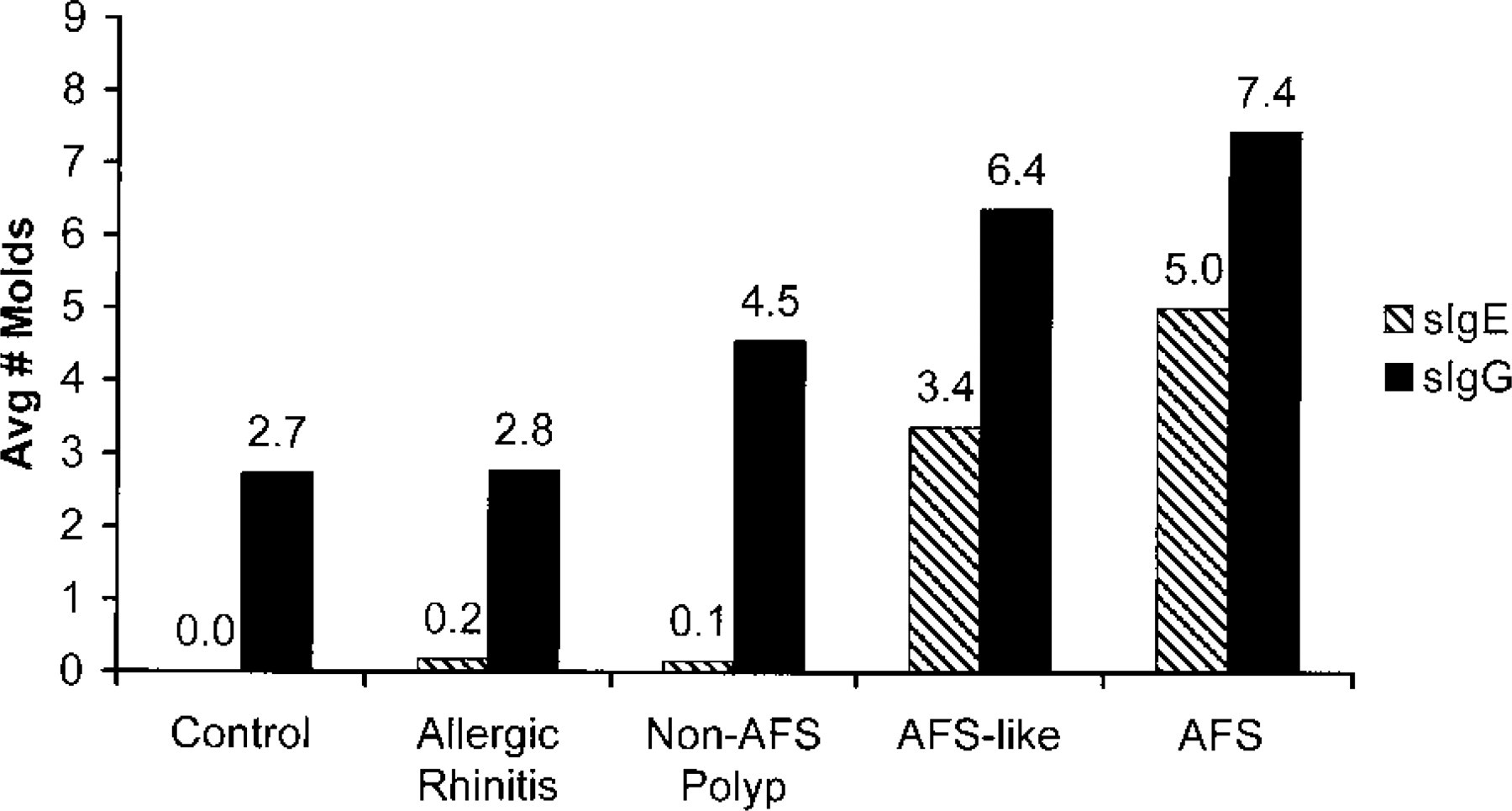
RAST class II and higher for sIgG and sIgE.
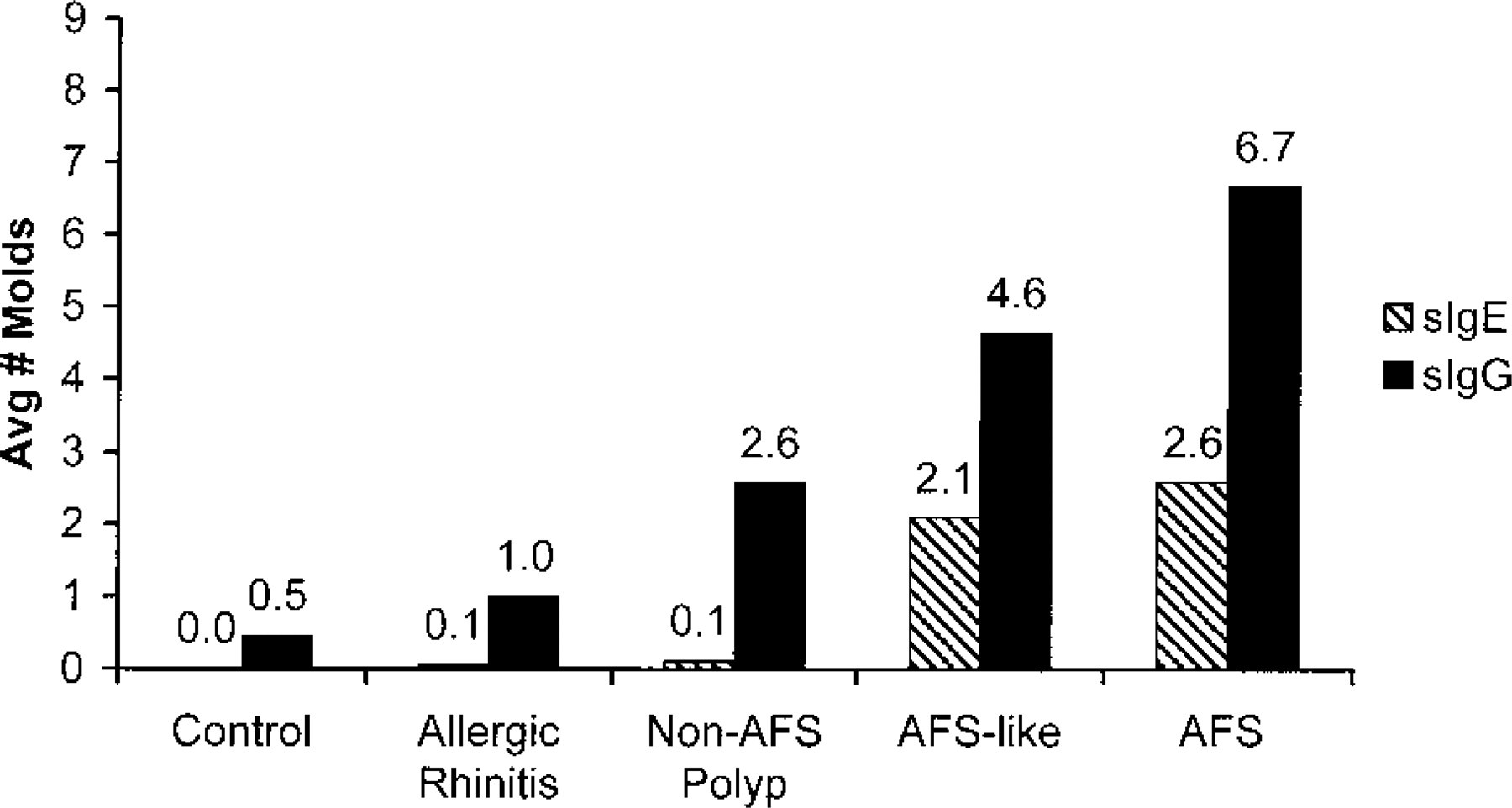
RAST class III and higher for sIgG and sIgE.
Elevations of fungal sIgG were seen in all patients (Fig 2.). However, patients with polyps (AFS, AFS-like, non-AFS polyp groups) had sIgG elevations of class III or higher (Fig 3.) to more of the fungi compared with nonatopic controls (P = 0.001, P < 0.001, P = 0.004) and allergic rhinitis patients (P < .001, P < 0.001, P = 0.018). The difference between the non-AFS polyp group and those with allergic rhinitis was not statistically significant as the method of analysis required a P value of <0.005 or better. The AFS group was significantly different from the non-AFS polypoid CRS group when class III and higher sIgG elevations (Fig 3.) were considered (P < 0.001) but not with class II and higher elevations (P = 0.006) (Fig 2.). As with sIgE, sIgG elevations in the AFS and AFS-like groups were not significantly different.
Polyp severity and RAST class II and higher for sIgG and sIgE.
Increasing polyp severity was associated with elevations of sIgG and sIgE to an increasing number of fungi as shown in Figures 4 and 5. Of note, although the majority of AFS and AFS-like patients had an unquestionable unilateral predominance of disease, only 4 patients were classified as class 1 (unilateral) polyp severity as most of these patients had some evidence of polypoid disease on the less-involved side. Five patients were classified as class 4 polyp severity, 12 as class 3, and 30 as class 2. The average polyp severity score was 3.0 for the AFS group, 2.6 for the AFS-like group, and 1.9 for the non-AFS polyp group.
The average total IgE was significantly higher (P < 0.001) in the AFS group at 971 U/mL compared with only 64 U/mL in the non-AFS polypoid CRS group (Fig 6.). Total IgE in the AFS-like group (730 IU/mL) was also significantly higher compared with this group (P < 0.001) but not statistically different from the AFS group (P = 0.469). The ranges of total IgE in the AFS, AFS-like, and non-AFS polyp groups were 201 to 3830 U/mL, 105 to 2162 U/mL, and 8 to 129 U/mL, respectively.
When total IgE and polyp severity were compared (Fig 7.), class 3 (864 U/mL) and class 4 (1643 U/mL) were significantly higher compared with class 2 (184 U/mL) (P < 0.001 and P = 0.004, respectively). Class 3 was different from class 1 (P = 0.004), but class 4 did not reach the required significance of P < 0.008 compared with class 1 (P = 0.014). Classes 3 and 4 were not statistically different (P = 0.692).
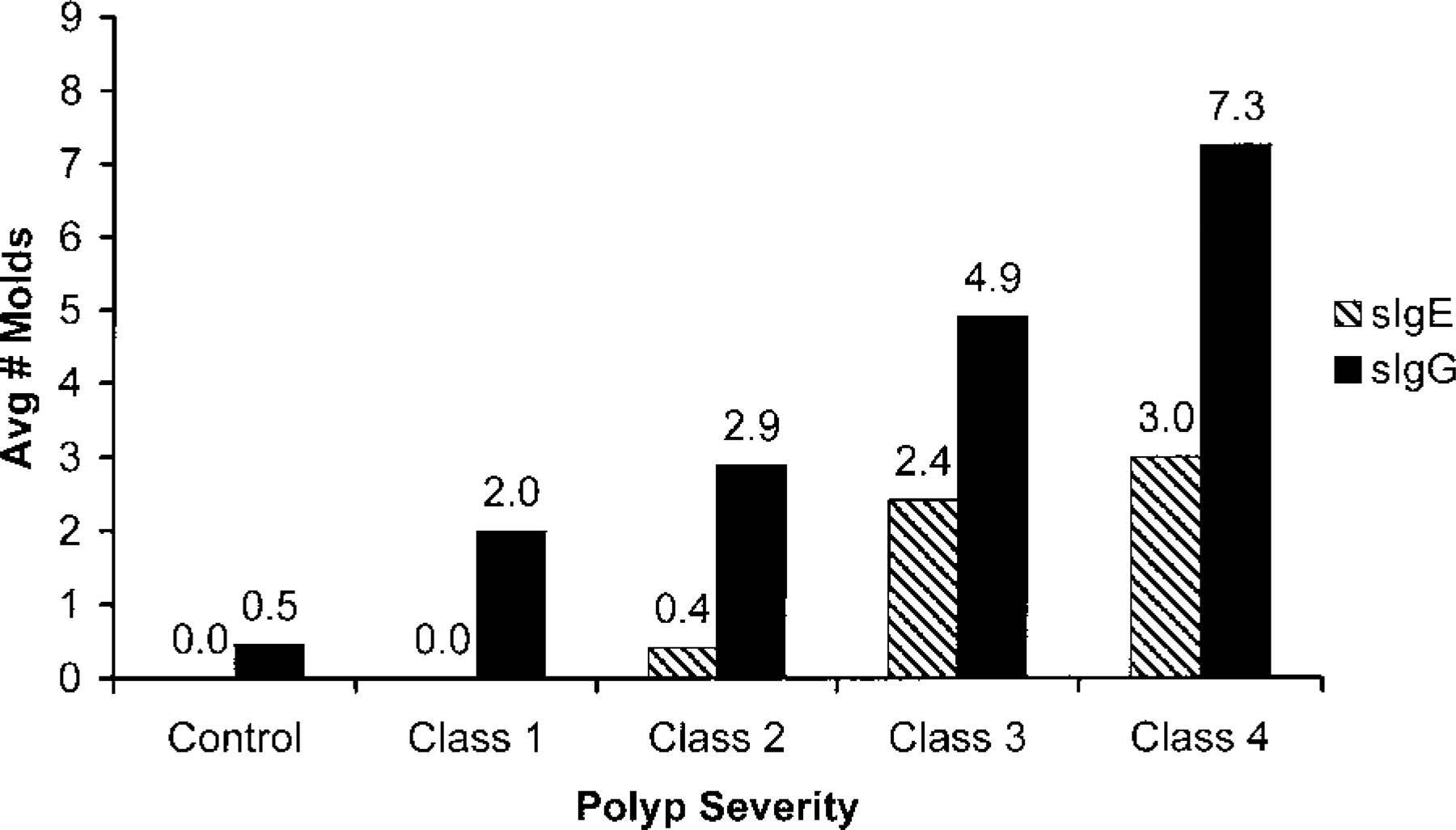
Polyp severity and RAST class III and higher for sIgG and sIgE.
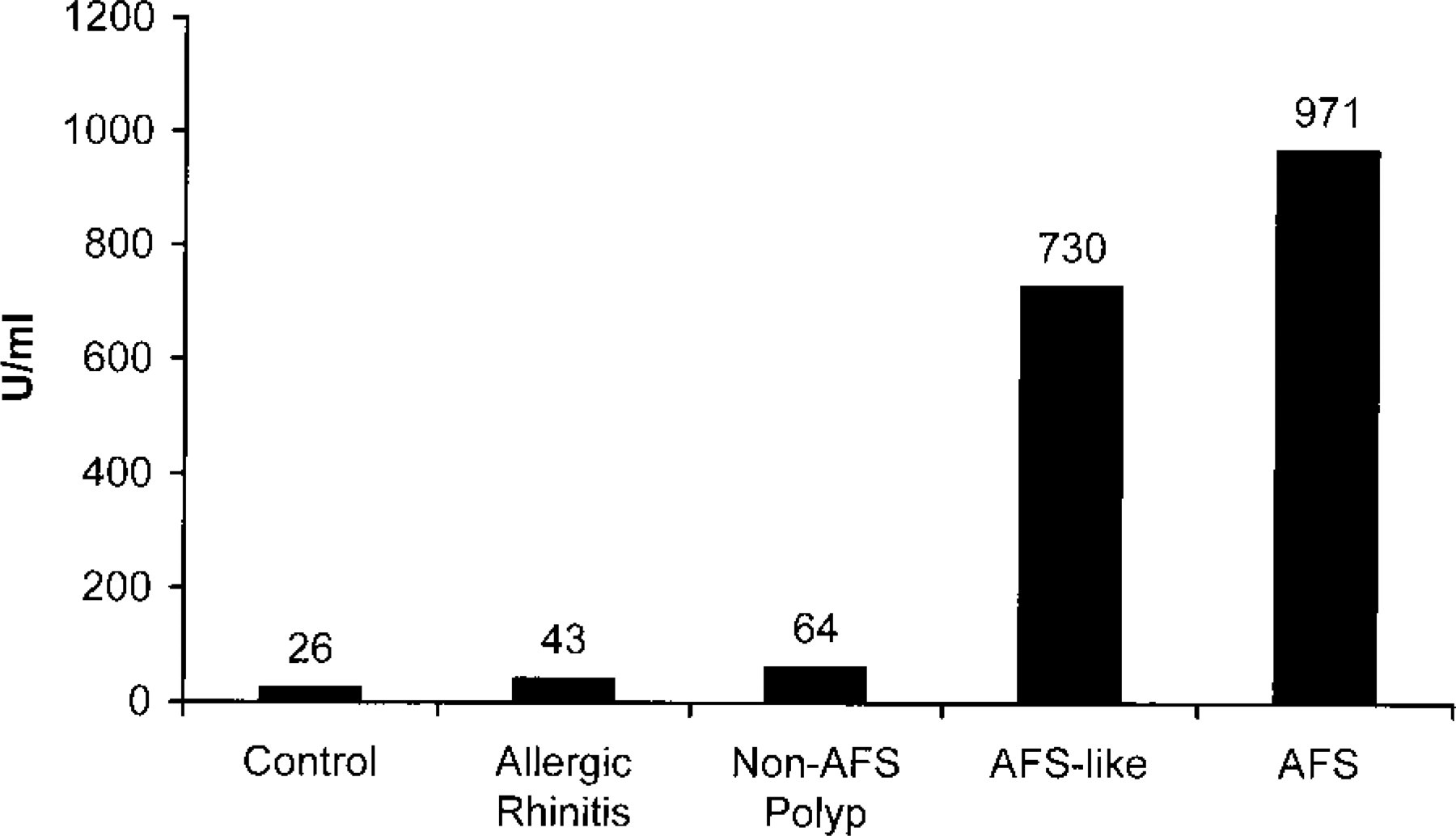
Total IgE among patient groups.
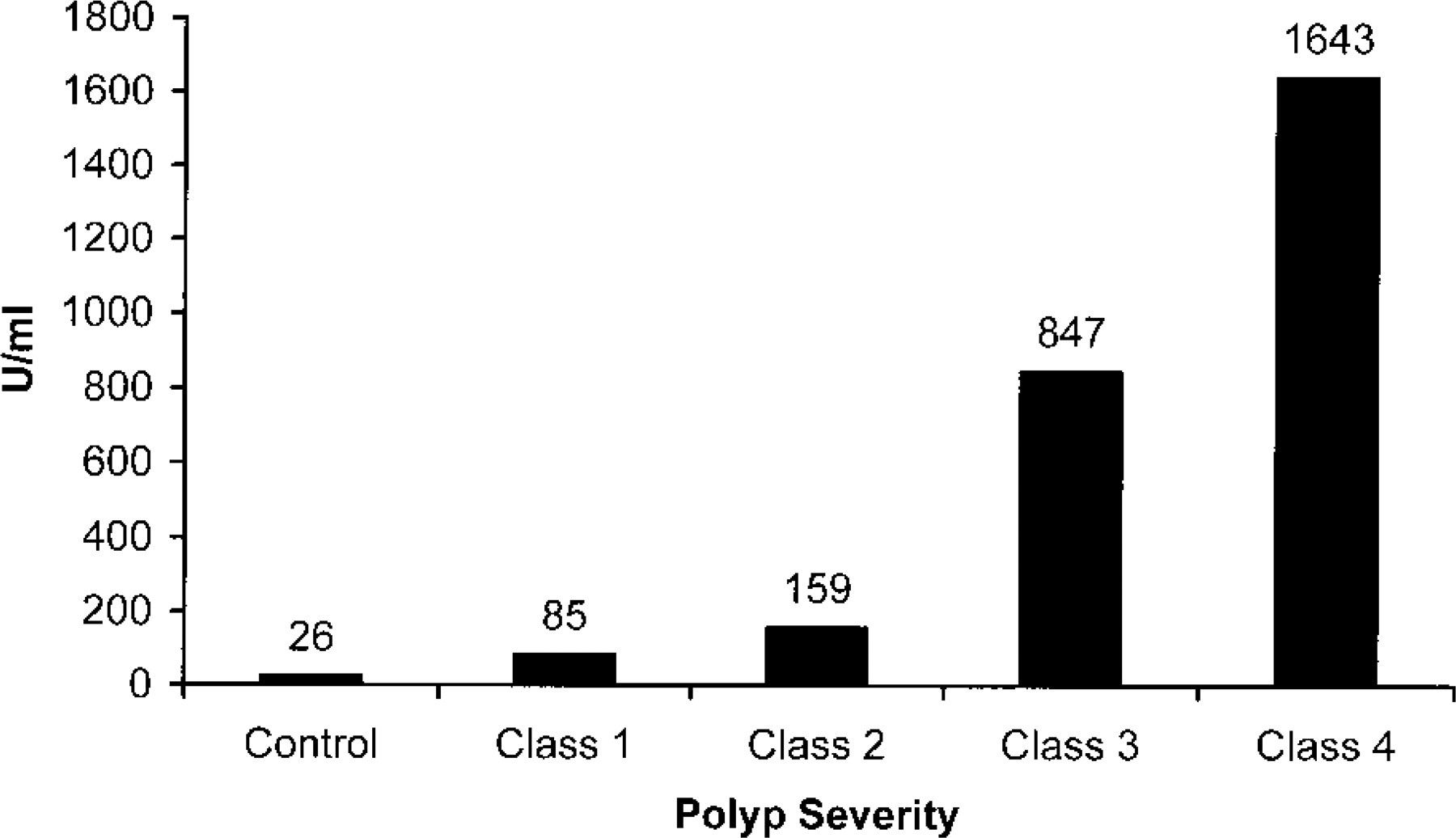
Total IgE and polyp severity.
DISCUSSION
The traditional gold standard criterion has been the demonstration of allergic mucin and the presence of fungi from a patient with CRS. Other criteria have included characteristic radiographic findings, polyps, and fungal atopy. There are many AFS-like patients who exhibit most of the classic characteristics but fail to have positive fungal cultures or stains. In clinical practice, these AFS-like patients are usually managed as AFS patients because of the perceived difficulty in confirming fungal presence. Those authors who report treating AFS-like patients as having “AFS” would welcome a more confirmatory and accepted substitute when fungal elements are not identified. Even though the pathophysiology of AFS is not completely understood, most of the evidence at least suggests a major role for an IgE-mediated process. This pilot study attempts to support the theory that the presence of elevated sIgE to multiple fungi may be an adequate substitution for direct evidence of fungal elements in the AFS-like patient. RAST is a simple means of identifying and quantifying sIgG and sIgE versus the most common fungi implicated in AFS.
RAST
In vitro testing via modified RAST is an accepted standard in screening and diagnosing inhalant allergy, including molds. 13 Tandy and Mabry 13 compared RAST and skin end point titration (SET) testing for Alternaria, Helminthosporium, and Cladosporium and found that RAST under-classified in only 1.09% of 92 tests. The sensitivity of RAST and its higher specificity compared with SET complement its other advantages of reproducibility, quantification, safety, and patient convenience. 22 It has become relatively inexpensive and clinically available and can be used to determine initial and even final immunotherapy doses when coupled with some form of skin testing such as a vial safety test. 14 Its use along with other in vitro techniques for sIgE analysis has been reported in the AFS literature, although no study reviewed to date has conducted any significant analysis of sIgG in AFS.
Specific IgE and IgG Elevation in AFS
In Katzenstein et al's 23 initial description of allergic Aspergillus sinusitis in 7 patients, they showed elevation of sIgG in only 1 patient and of sIgE in another. Brummond et al 16 demonstrated sIgG, sIgE, and serum precipitins from a culture-positive Curvularia–AFS patient. Numerous authors have subsequently reported additional cases in which both sIgE and sIgG were elevated. 3,17–21,24
Holman et al compared 20 16 Bipolaris–AFS patients with controls who had no history of asthma, polyps, or chronic sinusitis and found that 93% had elevated Bipolaris sIgG and 82% had elevated sIgE compared with only 1 of the 6 controls. The type of antibody exhibited by the control was not specified.
Schubert and Goetz 7 studied 45 patients with Bipolaris–AFS. All of these patients had a positive culture and skin prick test to Bipolaris. Patients were tested for serum precipitins and Bipolaris sIgG and sIgE by enzyme-linked immunosorbent assay. No other fungi were tested for. The authors' data showed that serum precipitins were elevated in only 3 of 45 patients, sIgG was elevated in 30 of 45, and the mean sIgE was not elevated. The fact that sIgE was generally not elevated despite positive skin prick tests to Bipolaris was attributed to the greater sensitivity of skin testing versus the in vitro test.
Manning and Holman 3 prospectively examined 8 Bipolaris–AFS patients for sIgG by RAST and for sIgE by enzyme-linked immunosorbent assay. All AFS patients had positive skin tests to Bipolaris and all had elevations of sIgG and sIgE. One of the 10 nonasthmatic, nonsinusitis control patients had a positive skin test and elevated sIgG and sIgE. One other control had an elevated sIgG, and the remainders were negative.
Mabry et al 21 followed sIgE and sIgG levels in their AFS patients being treated with immunotherapy. Both were generally elevated before therapy, and sIgE tended to remain the same or to rise slightly. No specific pattern for sIgG was shown.
The data presented here give further evidence that elevations of fungal sIgG and sIgE are present in AFS. All of our AFS and AFS-like patients had significant elevations of sIgE compared with control subjects and patients with polypoid CRS without evidence of AFS. Specific IgG elevations were significantly different between the AFS and the non-AFS polyp group only when class III and higher scores were considered. However, there was a definite trend of increasing fungal sIgG elevations when considering the spectrum of patients from nonatopic controls to those with AFS. The number of sIgG elevations was higher in patients with polyps compared with nonatopic controls and those with allergic rhinitis (Figs 2 and 3). This increased further with more extensive polyp disease (Figs 4 and 5). The increased number and magnitude of fungal sIgG elevations seen in patients with polyps and AFS may represent the patient's defensive response to the presence of saprophytic multifungal colonies growing in mucus retained by polyps. This may reflect a Gel and Coombs type III reaction in AFS as postulated for ABPA. 1,25
Further study of the role of IgG in polyps and AFS is required.
Multiple Fungal sIgE Elevations in AFS
Mold-allergic patients frequently have been shown to have sensitivities to multiple mold species. Some have argued that this is due to cross-allergenicity or a fungal panallergen, whereas others attribute this to independent sensitization to different mold species. 23,26 Multiple fungal sensitivities have also been shown in AFS. 26
Manning et al 5 compared 16 patients with histologic and culture proven AFS with 5 controls with a similar preoperative clinical picture, including a history of atopy, CRS, and massive polyposis. All patients were tested with modified RAST for sIgE against Helminthosporium, Curvularia, Alternaria, and Aspergillus. Fifteen of the 16 had sIgE (RAST class II or higher) to at least 1 of the dematiaceous fungi and 12 of 16 had sIgE to all 3 dematiaceous tested. The remaining patient had sIgE to Aspergillus fumigatus. Control patients did not have elevated sIgE to any of the fungi tested.
Mabry and Mabry 27 conducted skin tests in 10 AFS patients for 12 different fungi. Most patients had sIgE to multiple fungi, with all having positive results for Helminthosporium, Alternaria, and Stemphylium. Marple et al 28 later reported that they had not encountered any AFS patient without sIgE to Alternaria and Helminthosporium. When they compared SET and RAST testing for 11 fungi in 10 AFS patients, they found that all patients demonstrated sensitivity to almost every fungal antigen tested. 29 They also found that a total IgE of >1000 units/mL was an excellent predictor of AFS.
Kuhn and Javer 30 reported elevated sIgE to an average of 3.5 fungi per patient from a group of 10 AFS patients, ranging from 1 to 10 fungi per patient. All of our AFS patients had multiple sIgE elevations to the tested molds. By comparing sIgE results between various different patient groups, we found that only patients who had AFS or were AFS-like had elevated sIgE to multiple fungi. The most important differentiation was between the non-AFS polypoid CRS patients and the AFS/AFS-like group. We believe that the AFS and AFS-like patients represent the same spectrum of disease. Ferguson 31 proposed an immunologically distinct disease, termed eosinophilic mucin rhinosinusitis, to describe many of these AFS-like cases in which fungal evidence was lacking. She found 44 patients in the literature and added 29 additional patients who were AFS-like but did not have fungal elements isolated. Unfortunately, there were no significant data on fungal sIgE or sIgG available for the patient population.
Screening polypoid rhinosinusitis patients with total IgE and RAST for fungal sIgE and IgG may help identify AFS patients earlier. A group of patients at risk for developing advanced AFS will probably be identified. These patients may not yet have developed the classic clinical picture that has become familiar, and the question arises of whether these patients should also be managed as aggressively with surgery, steroids, and possibly immunotherapy. Some of these patients probably would never go on to develop advanced AFS, as several predisposing factors are probably required in the AFS cycle, as described by Marple. 1 Nonetheless, earlier diagnosis will facilitate earlier treatment and help avoid the situation in which AFS has already resulted in locally destructive disease, requiring more extensive surgical management and resulting in a poorer outcome. Early immunotherapy and extirpative surgery may help prevent escalation of the AFS cycle.
Gross Allergic Mucin
Although Ponikau et al 10 histologically demonstrated allergic mucin in 96% of 101 CRS patients with and without polyps, it is clear that the vast majority of these patients did not have what is generally accepted to be AFS. Our experience has been that the presence of gross allergic mucin at the time of surgery, in the context of a patient with polypoid CRS, elevated total IgE, characteristic radiographic findings, and multiple fungal allergies, is exceedingly specific for AFS. This is regardless of what is shown histologically. Histologic analysis remains necessary to help confirm the diagnosis of AFS and to rule out other pathology.
Several of our earlier cases, which are categorized as AFS-like, failed to have histologic evidence of allergic mucin despite the clear presence of gross allergic mucin at surgery. This was most likely attributable to inadequate collection of allergic mucin at surgery and/or ineffective communication with the pathologist. Establishment of a diagnosis is almost always based on tissue analysis, which is not the case with AFS. We now meticulously collect the allergic mucin in addition to the tissue specimens. After cultures are taken, it is separately placed in formaldehyde and sent for permanent section analysis. In addition to hematoxylin-eosin, special silver stains (eg, Gomori's methenamine and Fontana Mason) are performed to help identify fungal elements. This has drastically increased diagnostic yield, including with fungal cultures.
CONCLUSION
It appears that virtually all patients with rhinosinus polyps have multifungal colonies growing in the mucus retained by the polyps. The present study suggests that there is an association of increasing levels of sIgG with polyps, worsening polyp severity, and AFS. However, it is unclear whether this represents only increasing fungal exposure or a potentially pathologic immunologic defense mechanism as seen with ABPA.
RAST testing is a simple, sensitive, and specific means of identifying sIgG and sIgE elevations to the most common fungi associated with AFS. The subset of polypoid CRS patients who have AFS may be distinguished early by detection of elevated sIgE to multiple fungi. This finding combined with an elevated total IgE, which is found in most reports, is additional evidence supporting a critical role for a type I Gel and Coombs reaction in the pathogenesis of AFS. Therefore, the authors contend that elevation of sIgE by RAST is adequate evidence of the role of each identified fungus when diagnosing AFS in the absence of a positive fungal stain or culture. Consistent and accurate histologic diagnosis of AFS requires a high index of suspicion, adequate collection of gross allergic mucin at surgery, and communication with the pathologist.
Earlier recognition and treatment of AFS, through total IgE and RAST screening in polypoid CRS patients, can potentially reduce the incidence of the destructive effects of AFS. Additional studies to confirm are under way.
Footnotes
The authors wish to acknowledge Robert H. Riffenburgh, PhD, for his statistical input in this work.