
Abstract
OBJECTIVE: We present the application and initial results of a CO2 laser technique for the treatment of medically refractory chronic granular myringitis (CGM).
STUDY DESIGN AND SETTING: Retrospective case series of 15 treated ears in 13 consecutive patients between the ages of 6 and 14 years (median age, 9.0 years) cared for in a tertiary care specialty hospital.
RESULTS: Eleven of 15 treated ears had total resolution of CGM and associated symptoms; median follow-up time was 10 months. Three ears were improved, and 1 ear remained unchanged. Three of 5 preoperative tympanic membrane perforations healed after laser treatment; 1 patient developed a postoperative, dry perforation. Hearing was not impaired in any patient tested.
CONCLUSION: Preliminary results suggest that CGM, when refractory to medical treatment, can often be treated effectively by a single laser treatment.
Chronic granular myringitis (CGM) is an inflammatory disease of the tympanic membrane (TM) about which there has been renewed interest in the otolaryngology literature. 1–3 Myringitis usually manifests as painless otorrhea originating from a focus of nonepithelialized TM; additional potential symptoms include mild hearing loss, subjective aural fullness, and, rarely, otalgia. The spectrum of disease severity ranges from an asymptomatic ear with minimal moistness noted incidentally on otoscopy to large masses of granulation tissue causing malodorous drainage. 4
The etiology of CGM remains unknown. The majority of children with CGM have undergone prior otologic surgical procedures, thereby theoretically altering normal TM epithelialization. This is thought to give rise to a nonhealing ulcer, chronic inflammation, and CGM. 4 Although Staphylococcus aureus and Pseudomonas aeruginosa are commonly cultured from the otorrhea associated with CGM, the infectious role of these microorganisms in CGM pathogenesis is unclear.
Mild forms of the disease may respond to topical antibiotic-corticosteroid drop treatments directed at the infectious/inflammatory component. Relapsing disease, however, frequently occurs especially in previously operated patients because such therapy does not promote TM reepithelialization. 1,5 Other reported medical therapeutic options include the installation of topical antiseptics (alcohol, salicylic acid), the application of caustic materials (silver nitrate, boric acid, trichloroacetic acid, carbolic acid), and even treatment with topical formalin solution. 6 Surgical procedures under local or general anesthesia such as debridement or excision of the involved portion of TM with grafting have been inconsistently successful according to reports in the literature 3 and from personal experience (R.D.E.). Treatment options are further limited in children due to the need for cooperation requirements. The search to assist such patients with refractory CGM fortuitously led to the use of OtoScan CO2 laser with encouraging preliminary success.
MATERIALS AND METHODS
A retrospective chart review including office visits and operative reports was performed over a 21-month period to identify all pediatric patients who underwent laser treatment of CGM refractory to conservative medical therapy. Clinical criteria for laser application required CGM to be “incurable” by conventional antibiotic-corticosteroid drop therapy for at least 3 months. This decision was based on clinical criteria that included otoscopic appearance consistent with myringitis, audiometric results, and occasionally computed tomography of the temporal bone to rule out alternative underlying pathology (Fig 1). Children whose otorrhea was determined to be due to other middle ear pathology were excluded from the study.
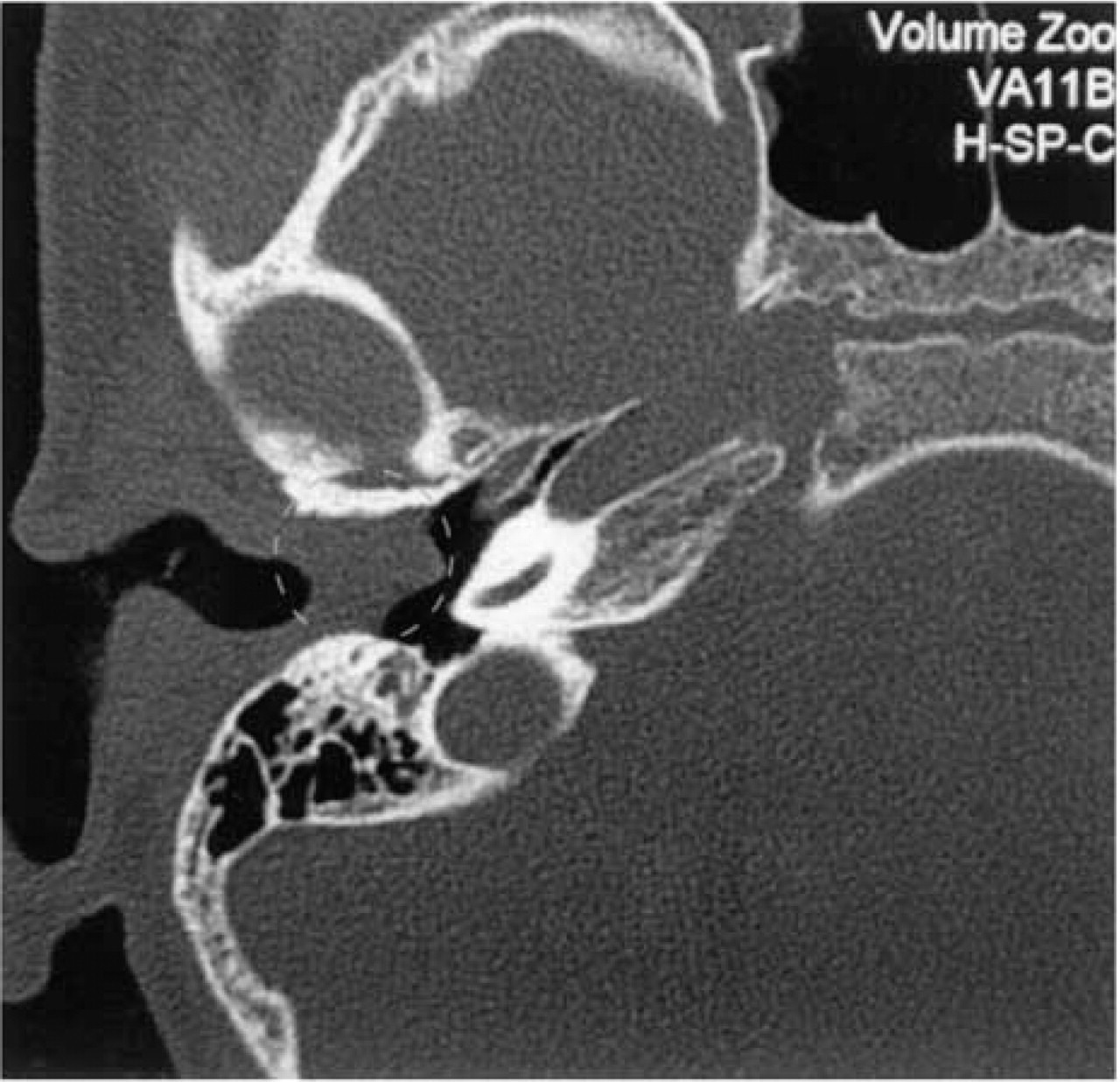
High-resolution axial CT scan of the right temporal bone at the level of the external auditory canal and middle ear in patient RS before laser treatment. A soft tissue mass fills the medial canal adjacent to the TM (black circle) correlating with the clinical findings of a mass of granulation tissue arising from the TM. The middle ear (∗) and mastoid are normal, a finding confirmed intraoperatively.
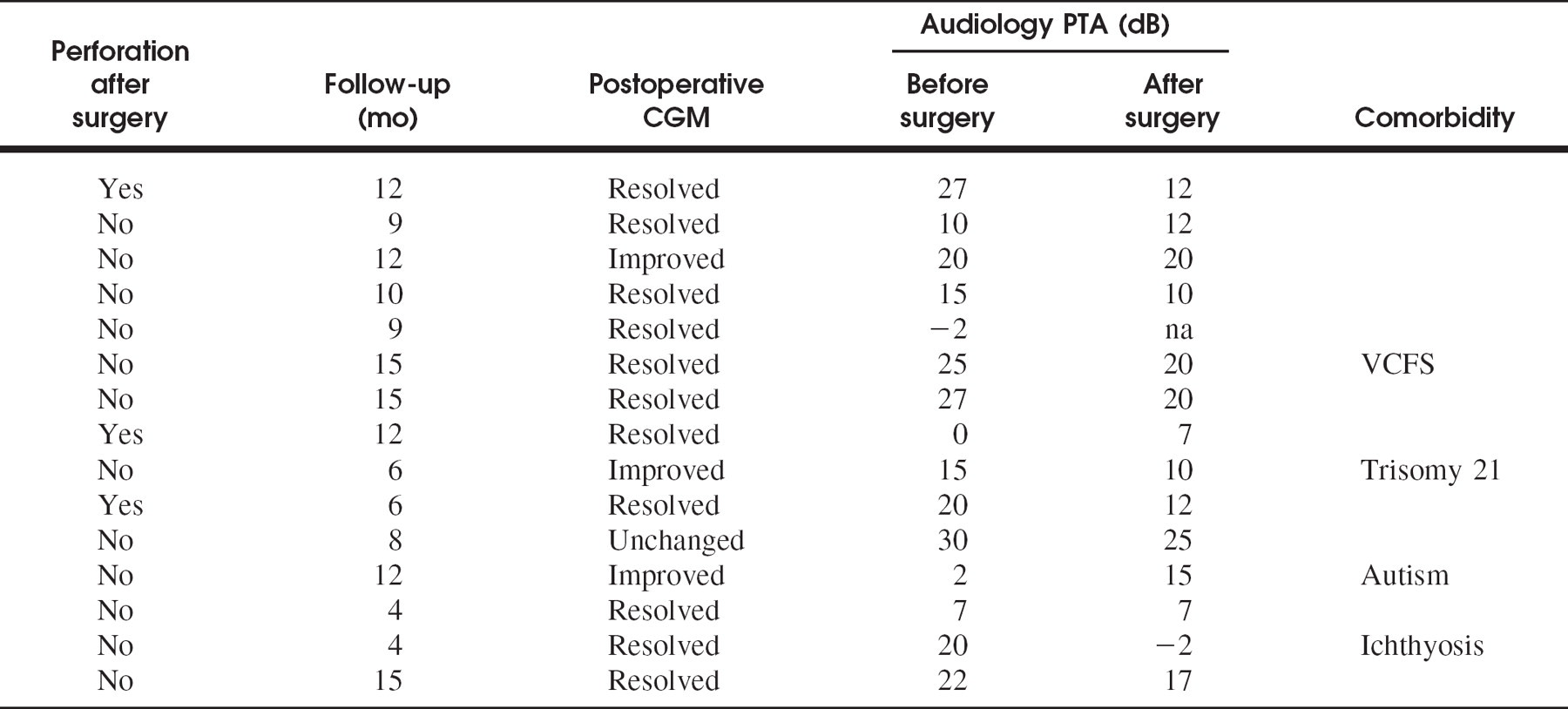
Thirteen consecutive patients with a total of 15 affected ears (11 right and 4 left ears) were identified (Table 1). All patients had undergone prior otologic procedures for prior middle ear disease, including tympanostomy tube placement, tympanoplasty, or tympanomastoidectomy, at least 1 year before laser treatment. Patient information including age, gender, length of symptoms, presence or absence of TM perforation, laser settings, complications, length of follow-up, and audiometric data was recorded. Audiologic data included preoperative and postoperative pure tone averages (PTAs) as determined by the best 2 of 3 test frequencies (500, 1000, and 2000 Hz).
Laser Procedure
All procedures were performed in the operating room under general anesthesia using the operating microscope for initial evaluation. The CO2 OtoScan laser (ESC Sharplan, Needham, MA) used for treatment is a freestanding unit with a handheld delivery system consisting of a CO2 laser scanner and illuminated video-otoscope. Laser energy settings were customized to the individual TM findings and ranged from 10 to 22 W with a spot size between 1.2 to 3.0 mm. Grossly evident granulation tissue was carefully lasered down to the level of the lamina propria of the TM. Such areas of granulation tissue were often additionally surrounded by an abnormal epidermal edge, which was similarly treated. The operative goal was to use the laser to resurface the TM to achieve a charred, dry, flat appearance that extended to include a narrow perimeter of epidermized, normal TM. A deliberate TM perforation (laser myringotomy or tympanotomy) also was created when necessary either to rule out middle ear disease or to freshen the edges of a preoperative perforation, which was present in 5 patients. Topical antibiotic-corticosteroid suspension drops (polymyxin B sulfate and neomycin sulfate with hydrocortisone) were instilled after the procedure and continued postoperatively until the first follow-up visit.
Follow-up
Patients were followed in the office for at least 3 months with the initial follow-up visit approximately 3 weeks after the procedure. The postoperative outcome was assessed by interim clinical history and office examination findings. For the latter an otoendoscope was routinely used, providing both an amplified view of the TM and enhanced parental education. For the purpose of this review, treated ears were categorized into 1 of 4 hypothetical outcomes grades: “Resolved,” an intact, completely epithelialized TM without otorrhea, moistness, or subjective complaints; “Improved,” marked improvement in both physical signs and preoperative subjective symptoms; “Unchanged,” little or no improvement of the TM appearance or symptoms; or “Worse,” the preoperative subjective symptoms had exaggerated, there was increased postoperative otorrhea, or the myringitis or granulation tissue occupied a larger area of the TM.
Initial Patient Report
A 6-year-old girl from the Middle East presented (to R.D.E.) with a history of copious right ear otorrhea that had been treated unsuccessfully by means of topical and systemic antibiotics for several months. Historically, she had undergone bilateral tympanostomy tube insertion with subsequent extrusion before onset of the otorrhea. Physical examination at the time of presentation revealed otorrhea filling the conchal bowl and draining onto the proximal neck; even with suctioning, the right TM could not be well visualized. The left TM demonstrated findings consistent with otitis media with effusion. Because the patient was due to return home within 48 hours, she was taken the next day to the operating room, where a ventilation tube was inserted in the left ear using laser myringotomy technique under general anesthesia. The right ear demonstrated focal granulation tissue involving approximately 15% to 20% of the TM with a pinhole perforation consistent with CGM. Because medical management had failed repeatedly and because the patient would not be available for follow-up if surgical debridement and skin grafting were performed, an alternative technique was necessary, creating the opportunity to use the same laser in innovative fashion. The laser procedure vaporized the granulation tissue with little bleeding, and an intentional circular myringotomy was created that included a peripheral rim of uninvolved TM. The otorrhea ceased within 7 days, and the myringotomy site had closed spontaneously by report from her local otolaryngologist. The TM appeared dry, intact, and epidermalized at the time of an eventual return office visit several months later.
RESULTS
Patient Data
The age of the patients in the study group ranged from 6 to 14 years (median, 9.0 years). Gender breakdown was nearly equally divided with 7 boys and 6 girls. The duration of otorrhea ranged from a minimum of 3 months in 6 patients to more than 2 years in 5 patients. The follow-up time ranged from 4 to 15 months (median, 10 months). Some patients had comorbid conditions, including trisomy 21 (patient 8), velocardiofacial syndrome (patient 6), congenital ichthyosis with cryptocia (patient 12), and autism (patient 10).
Outcome
At the initial outpatient follow-up visit at approximately 3 weeks postoperatively, 10 of the 15 treated ears showed total resolution of CGM after a single laser treatment procedure. At the end of the observation period (median time, 10 months), 11 of 15 (73%) ears continued to be disease free, and 3 ears remained significantly improved. One ear remained unchanged; interestingly, beyond the official follow-up period for this study, that ear also completely dried but was not recategorized as “resolved.”
Five of the 15 ears had TM perforations preoperatively (Fig 2). Three TM perforations (patients 2, 4, and 6) healed postoperatively and these TMs remained dry and intact throughout the observation period. Two dry perforations (patients 1 and 8) continued to be present at the end of the 3-month minimum observation period; neither of these 2 patients had any remaining evidence of CGM. In only 1 patient did a deliberately performed TM perforation not heal spontaneously after the laser procedure despite successful CGM treatment.
Audiologic data (PTAs) analysis was performed using the paired Student's t test. Although there was a trend toward better hearing with resolution of CGM, this postoperative change was not statistically significant.
DISCUSSION
The application of the CO2 Flashscan laser appears to be a simple and effective procedure to address CGM that fails to respond to medical management. Such “persistent” or “refractory” CGM resolved in 11 of 15 ears. Furthermore, 3 of 5 preoperative TM perforations healed. The laser procedure produced no adverse impact on hearing thresholds or other complications.
CGM is a chronic inflammatory process of the TM usually associated with a secondary infectious component. The TM granulations observed in CGM typically arise from an intact lamina propria in areas of epidermal disruption. 1,7 The initial event in the pathogenesis of CGM is suspected to be injury of the TM surface; however, most injuries to the superficial layers of the TM heal spontaneously by reepithelialization from the surrounding normal TM. 4 For CGM to develop, an arrest of this physiologic process of repair must occur that inhibits normal epithelial migration, leading to keratin accumulation and infectious destruction of the protective epithelial lining. 8 One hypothesis to explain the effectiveness of CO2 laser resurfacing over traditional nonsurgical treatment approaches is that the laser vaporizes not only granulation tissue but also the surrounding altered epithelium. Therefore, the normal physiologic healing process can reinitiate from areas of the TM not affected by CGM or its precursor conditions.
Relevant patient data
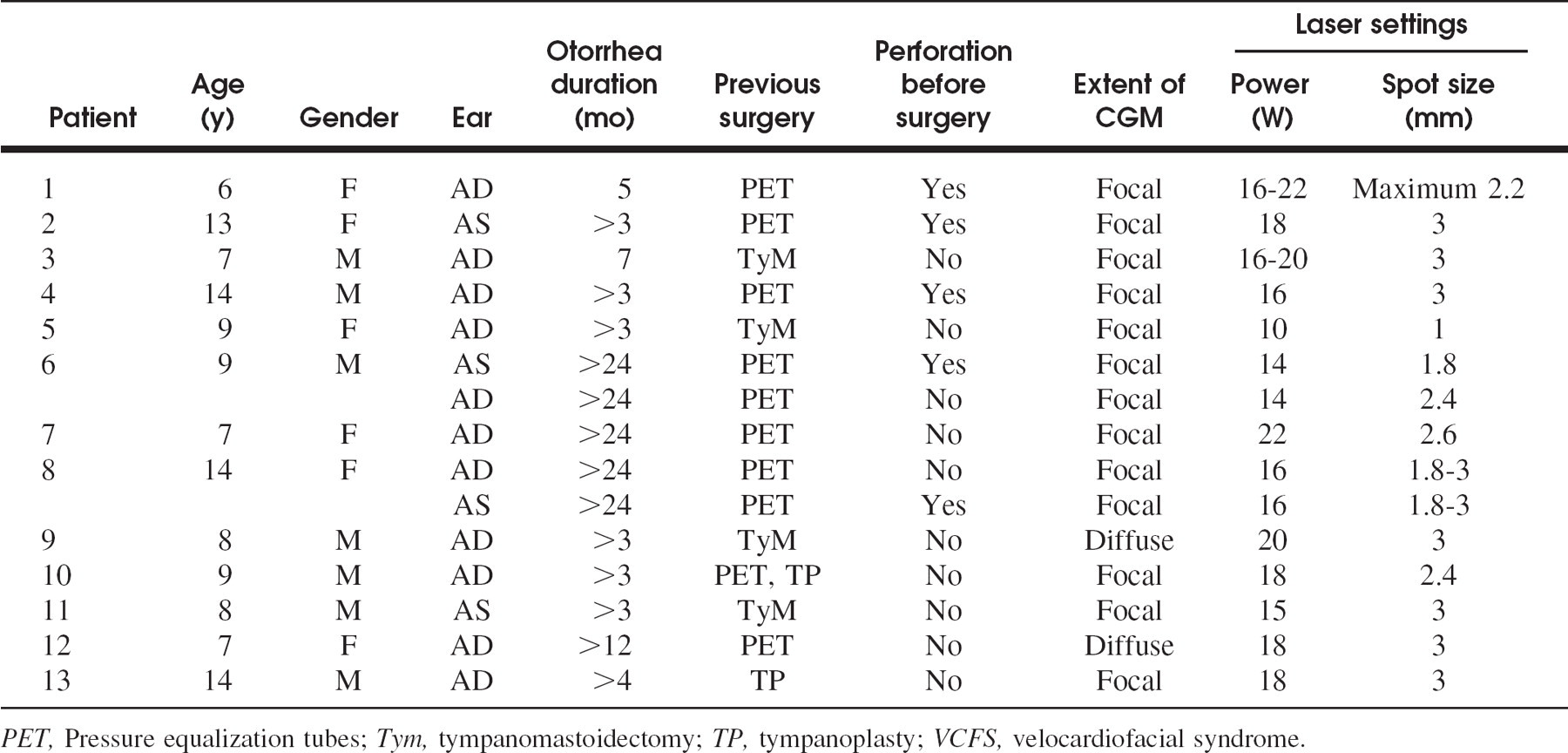
PET, Pressure equalization tubes; Tym, tympanomastoidectomy; TP, tympanoplasty; VCFS, velocardiofacial syndrome.
The CO2 laser resurfacing procedure is performed under video-magnification. Laser settings appropriate for both the diseased surface area as well as the depth of treatment can be precisely controlled. Vaporization in most cases is performed to the level of the lamina propria allowing reconstitution of the superficial layers of the TM from the healthy periphery, an approach that can help to avoid unintentional TM perforation. Alternatively, laser myringotomy or tympanotomy can purposely be performed either to rule out the possibility of middle ear disease or to freshen the margins of an existent perforation. Such laser-created, tube-sized perforations have a documented closure rate as high as 97.9% when laser-assisted tympanostomy is used to treat middle ear disease. 9
Notably, in our series, 3 of 5 preexisting TM perforations closed spontaneously after laser treatment, presumably by promotion of TM reepithelialization from the now disease-free perimeter of the perforation (Fig 2). Only 1 ear had a persistent, intentionally created perforation postoperatively. This perforation was successfully treated after an observation time of 6 months by means of a transcanal inlay cartilage graft/butterfly tympanoplasty. 10
Laser resurfacing is not intended to replace the initial medical management of uncomplicated CGM. Such therapy may be effective, particularly in selected CGM patients who have not undergone prior otologic procedures. 11 Silver nitrate application in the office also can be effective in the cooperative child from personal experience (R.D.E.). A recent study of 9 children with focal CGM reported good response to topical measures, including antibiotic and phenol with successful disease eradication. 2 However, in contrast to our patient population, none of the children in that report had prior otologic surgery. In agreement with our experience, a larger series of more than 90 adult and pediatric patients reported much less favorable medical treatment results; all 26 medically treated patients developed recurrences, sometimes leading to spontaneous TM perforation. 1 These authors recommend an aggressive surgical treatment approach to CGM consisting of curettage of granulations, elevation of a tympanomeatal flap, cartilage/perichondrium underlay graft, and lateral skin graft coverage of the denuded areas. Recurrences occurred in only 2 of 48 patients. 1 Unfortunately, similar surgical success was not achieved in another smaller series using the techniques of TM excision and fascia grafting with or without skin grafting to treat refractory CGM. All patients had undergone tympanoplasty and tympanomastoidectomy; 4 of 5 patients developed recurrences. 3
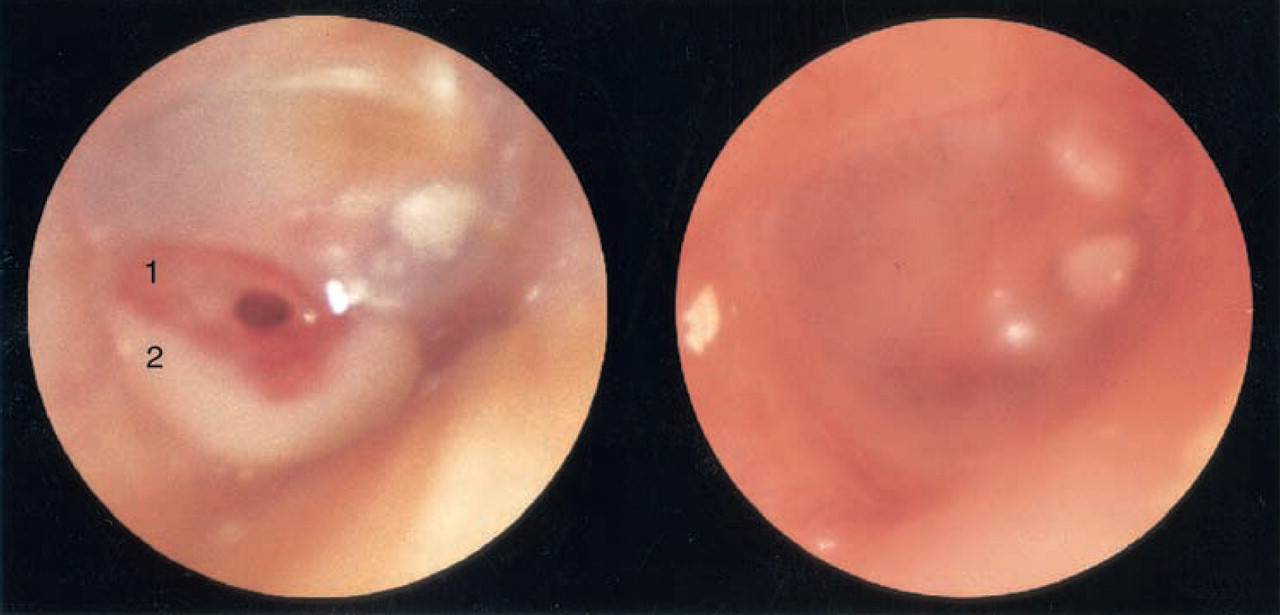
A, An otoendoscopic view of a right ear demonstrating (1) focal erythematous CGM involving the inferior TM with an associated microperforation and (2) purulence. B, The TM is intact and completely epidermized after a single laser treatment.
Given the variable success of aggressive surgical management of CGM, we suggest the alternative option of CO2 laser resurfacing treatment for cases refractory to medical treatment. This technique appears especially applicable to patients with a history of prior otologic surgery; such patients historically have demonstrated poor outcomes. Particularly for children who may not be cooperative, the CO2 laser resurfacing procedure offers promise given the potential requirement of general anesthesia anyway whether for surgical TM intervention, cleaning of the external auditory canal for diagnosis, or possibly the application of caustic medications. Interestingly, in the preparation of this manuscript we discovered an additional case report of the successful use of the CO2 laser in a CGM patient with resultant improvement of a secondary conductive hearing loss. 12
The CO2 laser is an effective, minimally invasive technique that can be performed safely and easily by an otolaryngologist already experienced with the use of the OtoScan CO2 laser for laser-assisted myringotomy. The technique provides a viable alternative to more aggressive surgical treatment approaches in patients with CGM refractory to medical management.