
Abstract
OBJECTIVE: We sought to assess skin whealing with glycerin-containing control injections for intradermal skin tests.
DESIGN: Observational.
METHODS: Wheal sizes were measured at 0, 10, and 15 minutes after intradermal injection of 0.01 and 0.02 mL of phenolated normal saline and 0.5% and 5% concentrations of glycerin in the same quantity of phenolated saline.
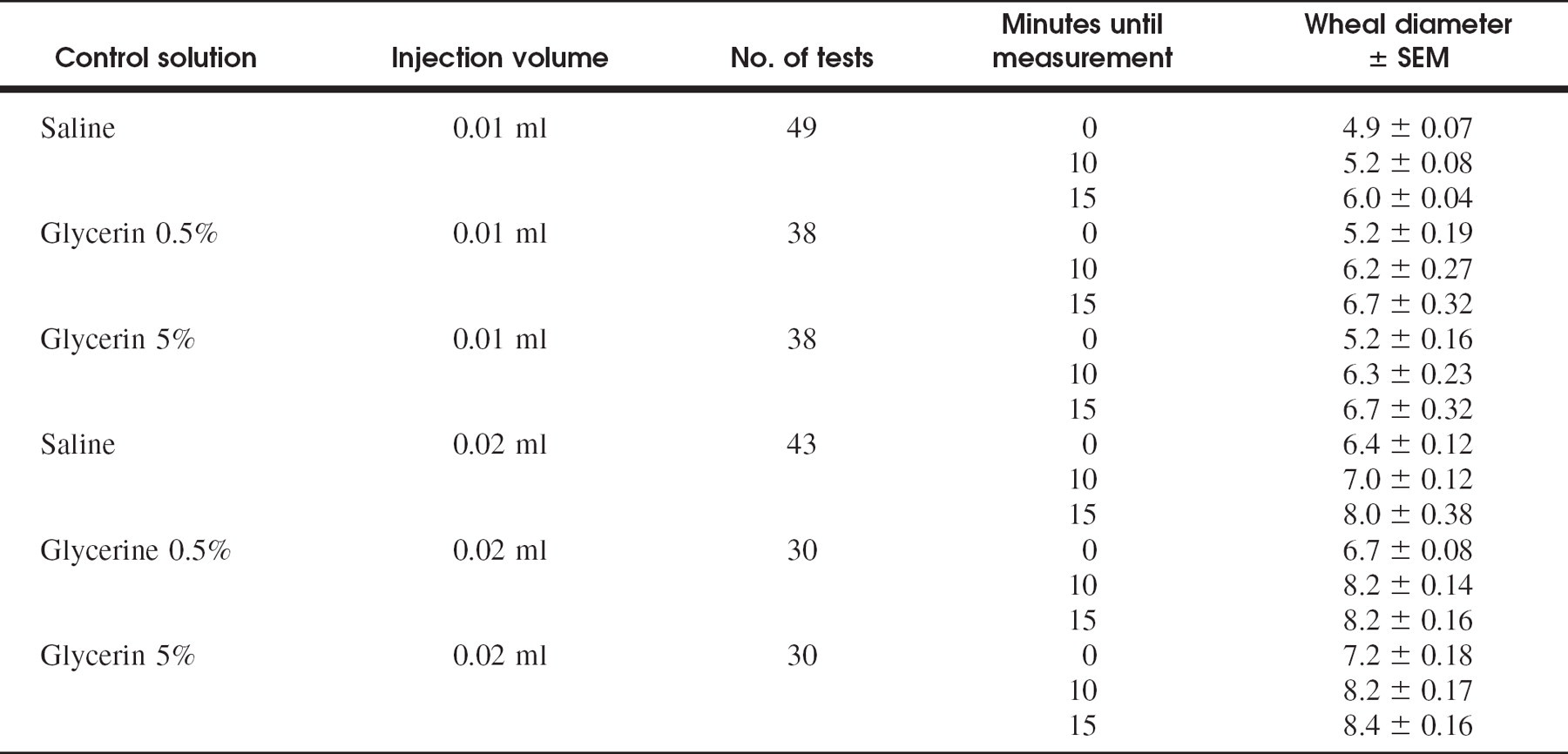
RESULTS: Intradermal injection of 0.01 mL of phenolated saline produced an average 4.9-mm wheal, which expanded to 5.2 mm at 10 minutes and to 6.0 mm at 15 minutes. Intradermal injection of 0.02 mL of phenolated saline produced a 6.4-mm wheal, which expanded to 7.0 mm at 10 minutes and 8.0 mm at 15 minutes. The addition of glycerin produced proportionally larger wheals.
CONCLUSIONS: Because glycerin increases whealing beyond that with phenolated saline, skin tests containing glycerin must be compared with glycerin-containing negative controls. Intradermal skin tests that fail to compare findings in this manner contain an inherent methodologic flaw and are uninterpretable.
A major issue in allergy testing is deciding whether the observed skin response is truly indicative of the patient having a clinically relevant, IgE-mediated reaction. 1 Skin test results are influenced by many variables, including patient skin response, specific technique, and tester consistency. Wheal measurement, comparisons with positive and negative control solutions, and interpretation are of equal importance. The development of in vitro methods for allergy diagnosis has helped to independently verify the accuracy of skin tests. In some cases, poor standardization of antigen sources and testing techniques has been shown to lead to discrepancies between skin tests and in vitro IgE antibody results of more than 100-fold. 2 It is also possible for skin tests to be falsely negative, as has been shown by comparing IgE blood tests with both skin tests and challenge tests. 3 Conversely, skin tests may be falsely positive because of nonspecific irritants, such as glycerin, present in allergen solutions. 4,5
Recommendations for immunotherapy must be based on clinical appropriateness as related to valid testing of proposed therapeutic agents. Recent reports by Nelson et al 6 and Wood et al 7 have suggested that skin prick tests (SPTs), even when negative, are sufficiently sensitive to diagnose clinical atopy without the need for further intradermal skin tests (IDTs). Both authors describe performance of a single IDT with injection of 0.02 mL of antigen solution. The basic tenant of their methodology is that all wheals resulting from an IDT measuring 6 mm or greater, accompanied by erythema, are to be recorded as positive. Nelson et al took measurements at 15 minutes, and Wood et al took measurements at an unspecified time. We were concerned that their methodology for IDTs created many false-positive results. This led to the condemnation of IDTs by these authors, stating that “a positive intradermal skin test response to Timothy grass in the presence of a negative skin prick test response to Timothy grass did not indicate the presence of clinically significant sensitivity to Timothy grass.” 6 We found the conclusion based on their particular IDT method to be suspect for 2 reasons: (1) it categorically assumes that an injection of 0.02 would produce a wheal of less than 6 mm and (2) it ignores the effects of small concentrations of the preservative glycerin, used in most all allergy test solutions, on whealing. Either assumption would lead to frequent false-positive skin test interpretations and discredit 60 years of intradermal testing. We therefore sought to evaluate control tests appropriate for use with the methodologies published in the general allergy literature to determine whether a 6-mm wheal with erythema should appropriately be interpreted as a positive or as a negative test.
METHODS
Forty-nine patients with clinically diagnosed allergic rhinitis, presenting consecutively over a 2-week period to 1 of 3 otolaryngic allergy practices were enrolled. All signed consent agreements to participate in this prospective study wherein each patient had negative control intradermal testing performed on the volar surface of the forearm according to both the IDT methods described in the general allergy literature, 6,7 using 0.02 mL injections, and the American Academy of Otolaryngic Allergy (AAOA) endorsed serial dilutional IDT method, using 0.01 mL injections. Both cited studies used negative IDT controls containing 0.03% human serum albumin in phenolated saline, without any added glycerin. Yet for their antigen testing Wood et al used an antigen concentrate at 10,000 BAU/mL in 50% glycerin and Nelson et al used antigen concentrates at 100,000 BAU/mL in 50% glycerin. Therefore, our test IDT solutions were made from a 50% antigen-free glycerin solution diluted ten-fold with phenolated normal saline to 5% glycerin content and then diluted 10-fold a second time with phenolated normal saline to 0.5% glycerin content. Allergy syringes of 0.5 mL capacity, with 28-gauge, fixed-hub, intradermal needles, were used. Each wheal was measured at the maximum and orthogonal diameters, averaged, and recorded at 0, 10, and 15 minutes after injection. Flares were also recorded.
The AAOA guidelines for IDT skin testing 8 specify the use of a positive histamine control, a negative control of phenol-saline, and negative dilution controls of glycerin at the same concentrations as each of the antigen-containing dilutions. 9 The guidelines also specify 10 that each IDT be made so as to create a 4-mm wheal that spreads to about 5 mm at 10 minutes. Because this method has proved to require approximately 0.01 mL of solution for injection, we also sought to evaluate appropriate use of controls using 0.01 mL injections.
RESULTS
Measured wheal diameters are presented in Table 1. Thirty percent of patients exhibited a flare response to injections containing glycerin compared with no flares observed from phenolated saline injections. The addition of glycerin to the test solutions increased both initial and subsequent wheal diameters in 100% of patients compared with phenolated saline injections.
Mean wheals resulting from 0.02 mL injections read at 15 minutes for all 3 negative control solutions exceeded 6 mm (8.0, 8.2, and 8.4 mm). We found that injecting 0.01 mL of normal saline produced a mean wheal of 4.9 mm that grew to 5.2 mm at 10 minutes. Wheals from 0.01 glycerinated solutions of 0.5% and 5% produced 5.2-mm wheals that grew to 6.2 and 6.3 mm at 10 minutes and 8.2 and 8.4 mm at 15 minutes, respectively.
DISCUSSION
These experimental findings cast substantial doubt on the conclusions regarding the lack of validity of IDT as reported by both Nelson et al and Wood et al. Their statements that IDT offers less clinical correlation than a negative SPT were based on an arbitrary 6-mm criteria for a positive antigen wheal reaction. All of their comparisons with in vitro tests, nasal challenges, or symptom scores to show clinical relevancy of IDT versus SPT were based on this criteria. Rather, our demonstration that antigen-free control solutions from a 0.02 mL injection produce wheals and erythema that meet or exceed 7 mm serves to suggest a major flaw in their methodology.
Several studies have attempted to access the relative diagnostic merits of SPT compared with IDT. Although the SPT offers high specificity and ease of use, its sensitivity can be less than 45%, 11 making it a poor choice for diagnosing atopy when there is only mild or moderate elevation of IgE. For low sensitivity patients, SPT results are often negative, and often only IDT may be positive. 12 Skin prick testing has been shown to suffer from extremely variability. Dreborg 13 notes that SPT may be used to determine potency of allergens “provided quadruplicate tests with at least three 10-fold concentrations are used.” He showed the coefficient of variation for SPT is more than 20% using the diameter of the wheal. Antico et al 14 studied the precision of the deposit of skin test solution using SPT and reported the median volume of inoculum to range from 0.42 to 82.25 nL. The American Academy of Asthma, Allergy and Immunology (AAAAI) has recognized this shortcoming of the SPT in the 1995 Practice Guideline, 15 which states that if atopic disease is clinically suspected in the presence of a negative SPT, an IDT is “recommended to confirm a truly negative percutaneous skin test.” Yet, although single IDTs are both very sensitive and very specific, 16 and more reproducible than SPT, 17 they have been suspected of producing clinically irrelevant false-positive results.
Mean wheal diameter of negative control intradermal injections
Equally important is the question of clinically relevant sensitivity when testing individual antigens. Skin testing is regarded by most allergists to correlate with clinical disease more closely than any other test. There is known to be significant variability between a positive in vivo or in vitro test and direct challenge test, whether by pollen, cat dander, or foods. Clinical relevance on challenge by an allergen is dependent on a variety of additional parameters including season, total allergy exposure, sensitivity threshold, etc. van der Veen et al 18 have shown that “the degree of sensitivity does not contribute to the prediction of the allergic response after allergen inhalation.” Dilutional IDT offers increased accuracy, because several increasing concentrations of antigen produce quantitatively increasing wheals. It is for these reasons that the AAOA has long endorsed dilutional IDT, referred to as skin endpoint titration (SET), as the skin testing method 10 of preference. The clinical value of IDT is also supported by both the American Medical Association Committee on Scientific Affairs (AMA Council) and by the European Academy of Allergology and Clinical Immunology (EAACI). 19 Dilutional IDT have become the standard by which all new allergens are quantified at the National Institutes of Health. 20
It is essential that all scientific experiments use accurate positive and negative controls, without which it is impossible to establish any value of clinical significance. Several methods exist for interpreting single IDT using 0.02 mL injections. The studies by Nelson et al and Wood et al chose a 6-mm wheal diameter as a positive response, which, in conjunction with erythema, they thought should indicate significant allergic sensitivity. Yet they found these corresponded poorly with nasal challenges of the same allergen. Our finding of mean wheals from 0.02 mL injections read at 15 minutes to average 8 mm would suggest a high incidence of false-positive results using their criteria. Although the AAAAI does not officially recommend a particular method for IDT, several articles in their literature do recommend the use of negative controls with dilutions of the preservative. 21,22 Finally, EAACI members also commonly perform IDT by injecting 0.02 mL of 10-fold dilutions that is interpreted after 15 minutes. 19,23 They stipulate the use of control tests with dilution buffer and describe the wheal diameter for clinically significant disease to be from 7 to 10 mm, 24 although they also fail to stipulate size in relation to the control test wheal. Our tests found that there is a normal, physiologic skin response for negative control wheals produced by 0.02 mL injections that ranges from 7.0 to 8.2 mm at 10 minutes and from 8.0 to 8.4 mm at 15 minutes, depending on the glycerin concentration.
Our clinical experience with IDT agrees with the observations of Menardo et al 5 and Guerin and Tioulong 4 that wheals containing glycerin show significant wheal growth compared with wheals containing only phenolated saline. According to AAOA guidelines, for a wheal to be considered a positive indicator of atopy, the wheal size must measure 2 mm or more than a negative control with comparable glycerin concentration. Many patients exhibit nonspecific wheal-and-flare reactions to concentrations of glycerin greater than 2% wt/vol, and some react to concentrations of 0.08% or less. Flares and erythema are not considered significant because they are not dependent on IgE-mediated inflammation. 25 Consequently, when using 0.02 mL for IDT, wheals would need to be greater than 8.2 mm for 0.5% glycerin and 8.3 mm for 5% glycerin-containing solutions to be considered a valid positive reaction. When glycerin is present in allergen test solutions, arbitrarily choosing a wheal size of 6 mm or even 7 mm as the criterion for positivity can cause truly negative tests to be misinterpreted as positive. The findings of Wood et al and Nelson et al of many false-positive tests served to decrease the apparent specificity of IDT, thus discrediting the test procedure in their conclusion, leaving only prick testing for the allergist to use. This would be true if it was not necessary to ensure that wheals made with concentrated allergen dilutions always be compared with concentration-matched glycerin-containing negative controls. A positive or negative wheal interpretation cannot be made based on any arbitrary wheal size.
Our findings clearly demonstrate that accurate diagnosis with any IDT method requires the use of appropriate negative controls, particularly the use of glycerin-containing controls at the same concentration as exists in the antigen containing test solutions. Failure to compare antigen tests to appropriate glycerin controls results in false-positive skin test interpretations and has lead to the publication of inaccurate and misleading research reports. 6,7
CONCLUSION
This study demonstrated that intradermal injections of 0.5% and 5% concentrations of glycerin in phenolated normal saline produced wheals that were larger than comparable saline wheals at both 10 and 15 minutes postinjection. Furthermore, glycerin also often causes erythematous skin flaring that mimics antigen injections. To be valid, a positive IDT wheal must exceed the size of the appropriate negative control. Because glycerin increases the skin whealing response beyond that caused by normal saline, when allergen test solutions are prepared from glycerinated aqueous concentrates, it is essential to compare these skin tests with glycerin-containing controls at the same concentrations as exist in the allergen-containing tests. All allergy studies that use IDT methods that fail to test and report results compared with such glycerin-containing controls contain an inherent methodologic flaw and should be regarded as uninterpretable.
The authors wish to thank Hollister Stier (Redmond, WA) for technical information and Antigen Labs (Liberty, MO) for assistance and supplying Brown-Murrow needles.