
Abstract
BACKGROUND: Graves' orbitopathy can produce proptosis, compressive optic neuropathy, and extraocular motility abnormalities; symptoms result from an increase in orbital volume due to expansion of intraorbital fat, with or without extraocular muscle involvement.
STUDY DESIGN: We conducted a chart review of patients who underwent orbital decompression to treat Graves' orbitopathy. Twenty-two orbits (13 patients) underwent orbital bone decompression, of which 17 orbits (9 patients) underwent the combined medial and lateral “balanced” decompression.
RESULTS: All patients had significant improvement with an average decrease in proptosis of 5.9 mm in the balanced decompression group. Restoration of normal optic nerve function was achieved in all patients with compressive optic neuropathy. Diplopia was noted in 4 patients (30.7%) preoperatively. Two patients had new postoperative diplopia (15.35%).
CONCLUSION: In our experience, “balanced” decompression results in a reduction of proptosis and improved optic nerve function and has a low incidence of complications.
MATERIALS AND METHODS
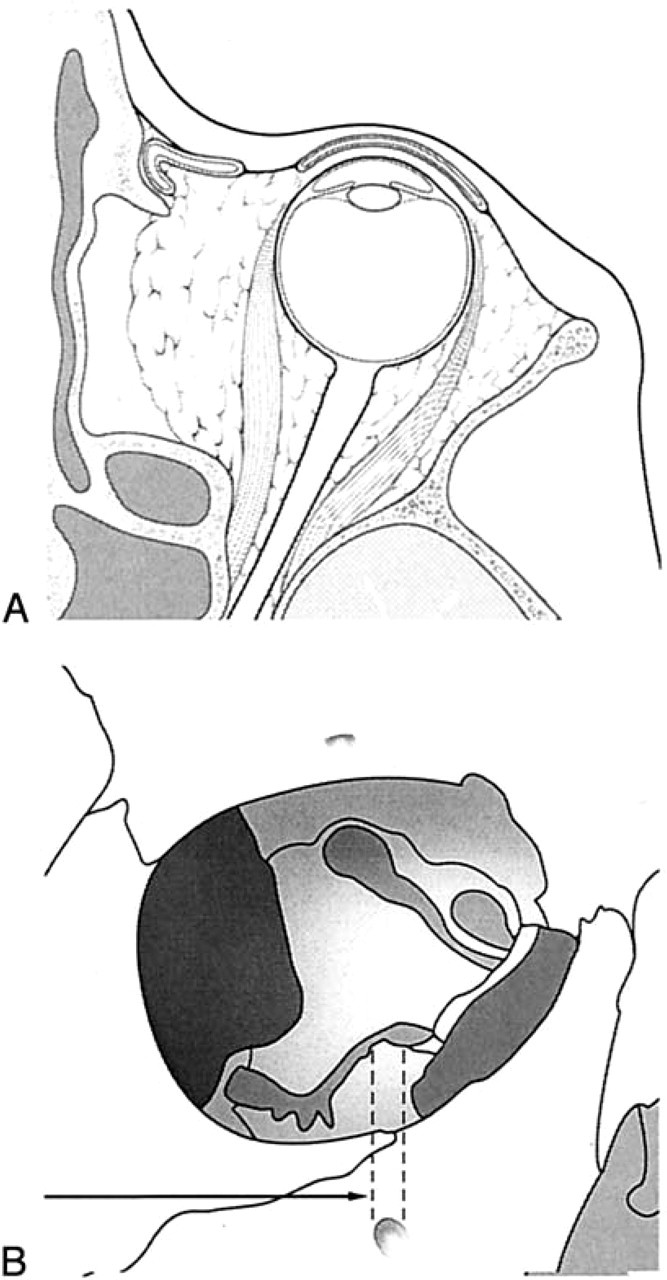
The charts of 410 patients who underwent treatment for Graves' orbitopathy over a 3-year period (1998 to 2000) at New York Presbyterian Hospital were reviewed; 85 orbital decompressions were performed in 45 patients. Bony decompression was performed in 22 orbits, and fat decompression was performed in 63 orbits. Indications for surgery, preoperative and postoperative Hertel measurements, optic nerve function, orthoptic measurements, and complications were analyzed (Table 2). Patients underwent either (1) combined endoscopic medial endonasal and lateral internal “balanced” decompression (Fig 2), (2) fat and 1 orbital wall (medial or lateral) compression, or (3) fat decompression only. The choice of surgery depended on the clinical findings and orbital pathology. Indications for balanced decompression procedure included compressive optic neuropathy and severe proptosis with enlarged extraocular muscle volume.
Assessment of severity of Graves' orbitopathy
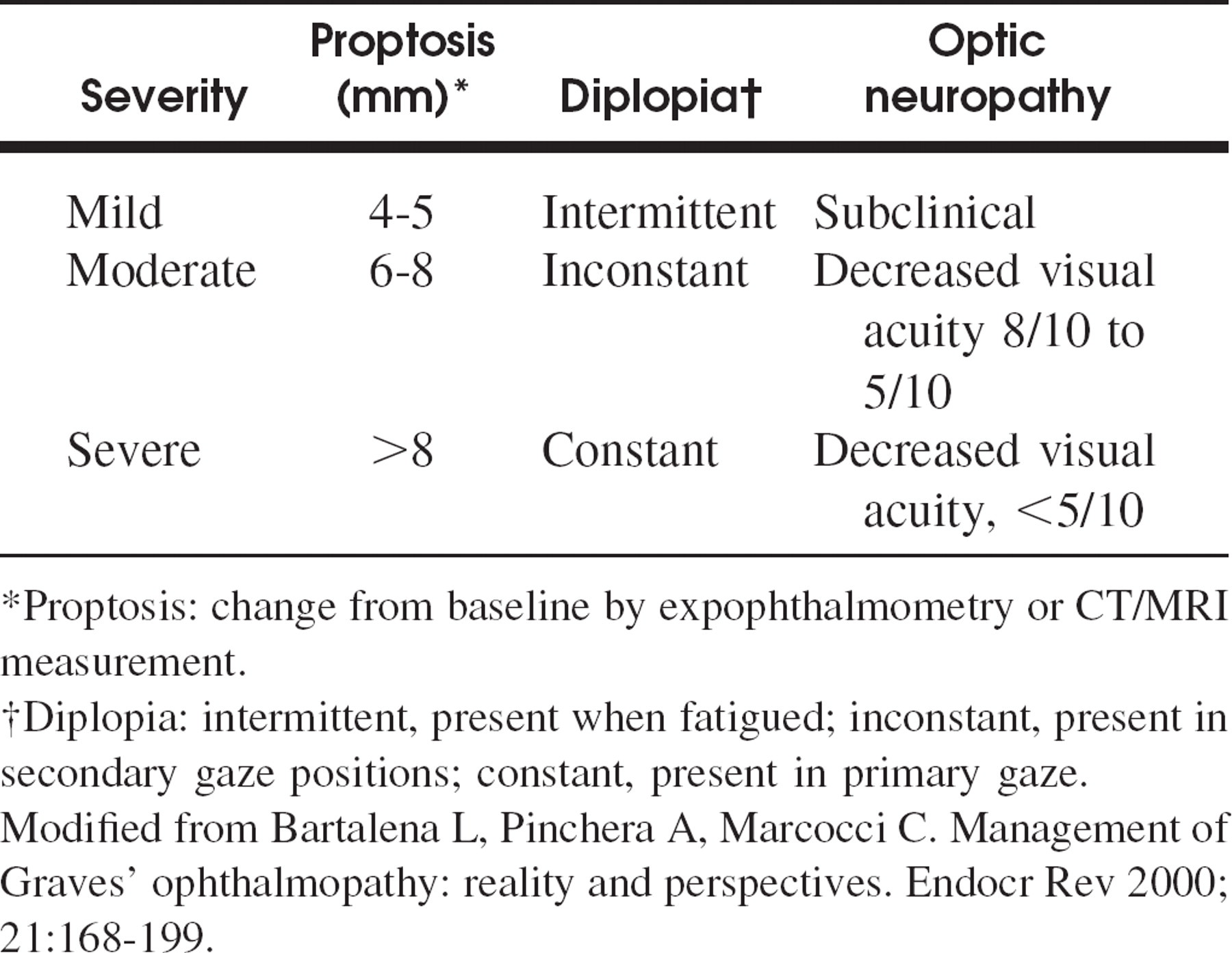
Proptosis: change from baseline by expophthalmometry or CT/MRI measurement.
Diplopia: intermittent, present when fatigued; inconstant, present in secondary gaze positions; constant, present in primary gaze.
Modified from Bartalena L, Pinchera A, Marcocci C. Management of Graves' ophthalmopathy: reality and perspectives. Endocr Rev 2000;21:168–199.
All surgery was performed via a joint otolaryngology and ophthalmology team approach by the senior authors.
Procedure
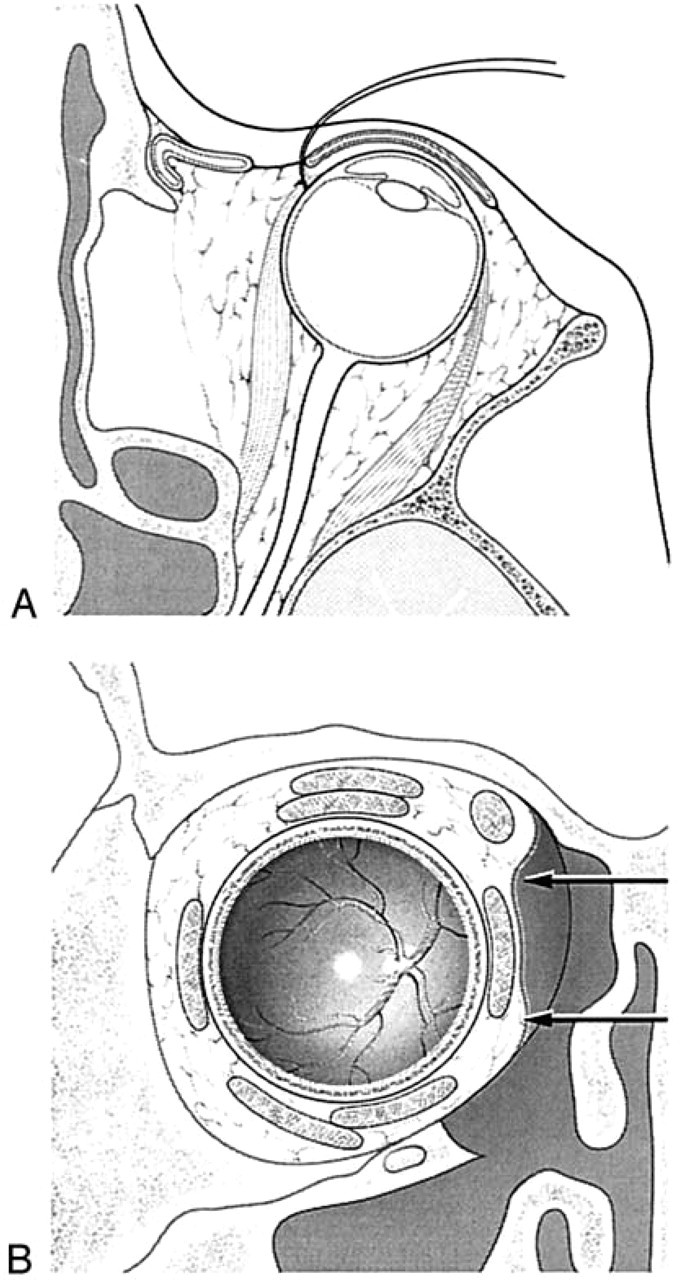
In cases requiring periorbital incision, a 4–0 suture was placed beneath the tendon of the medial rectus muscle to facilitate anterolateral retraction. This maneuver tented the septum orbitale adjacent to the medial rectus muscle and prevented injury of the muscle by the endoscopic surgeon (Fig 3). The septum orbitale was then incised above and below the muscle with a fine curved scalpel, from posterior to anterior to avoid obstruction of the operative field by the herniated fat.
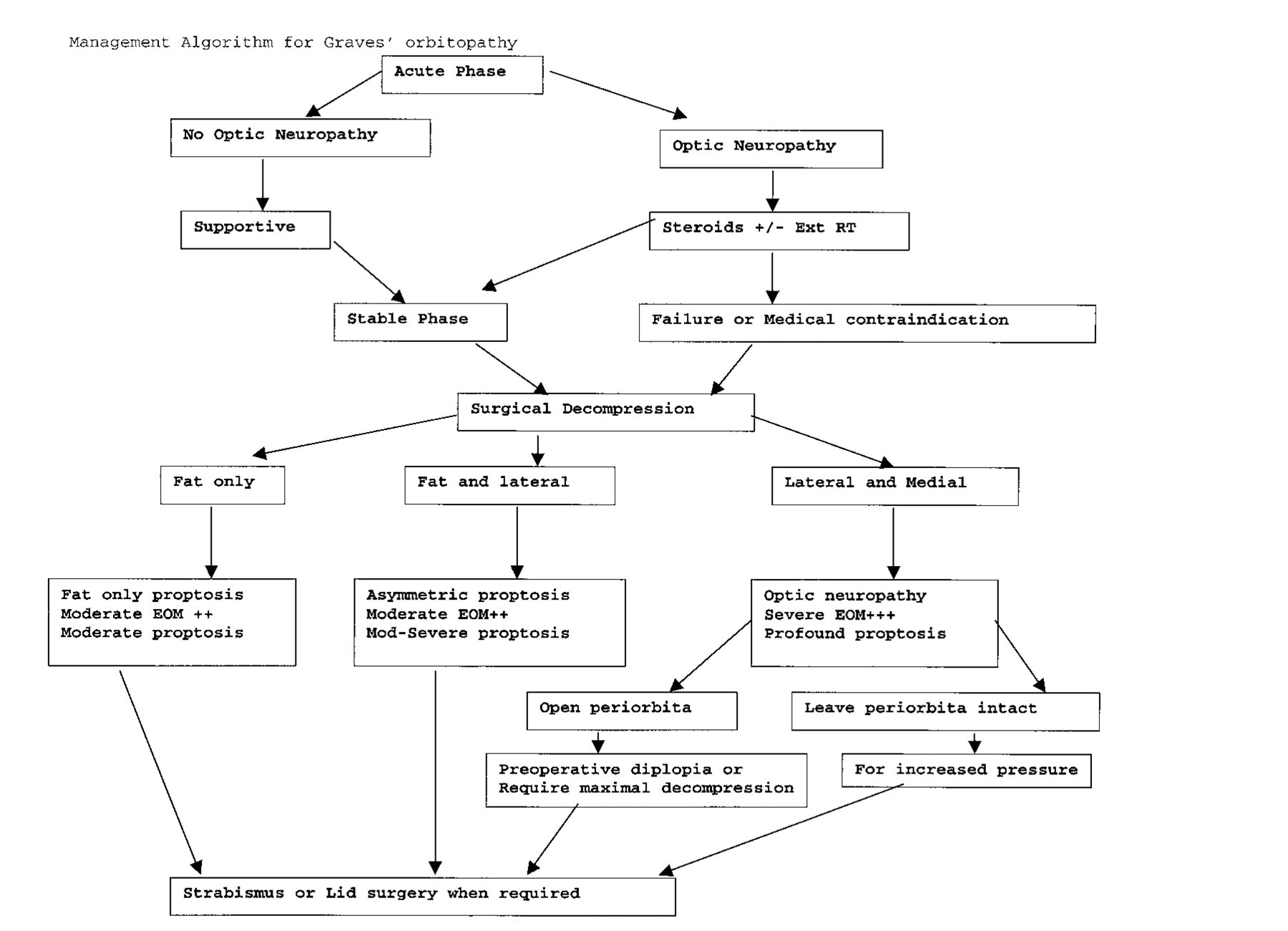
Management algorithm for Graves' orbitopathy. EOM, Extraocular muscle hypertrophy; +, mild; ++, moderate; +++, severe.
Indications for decompression
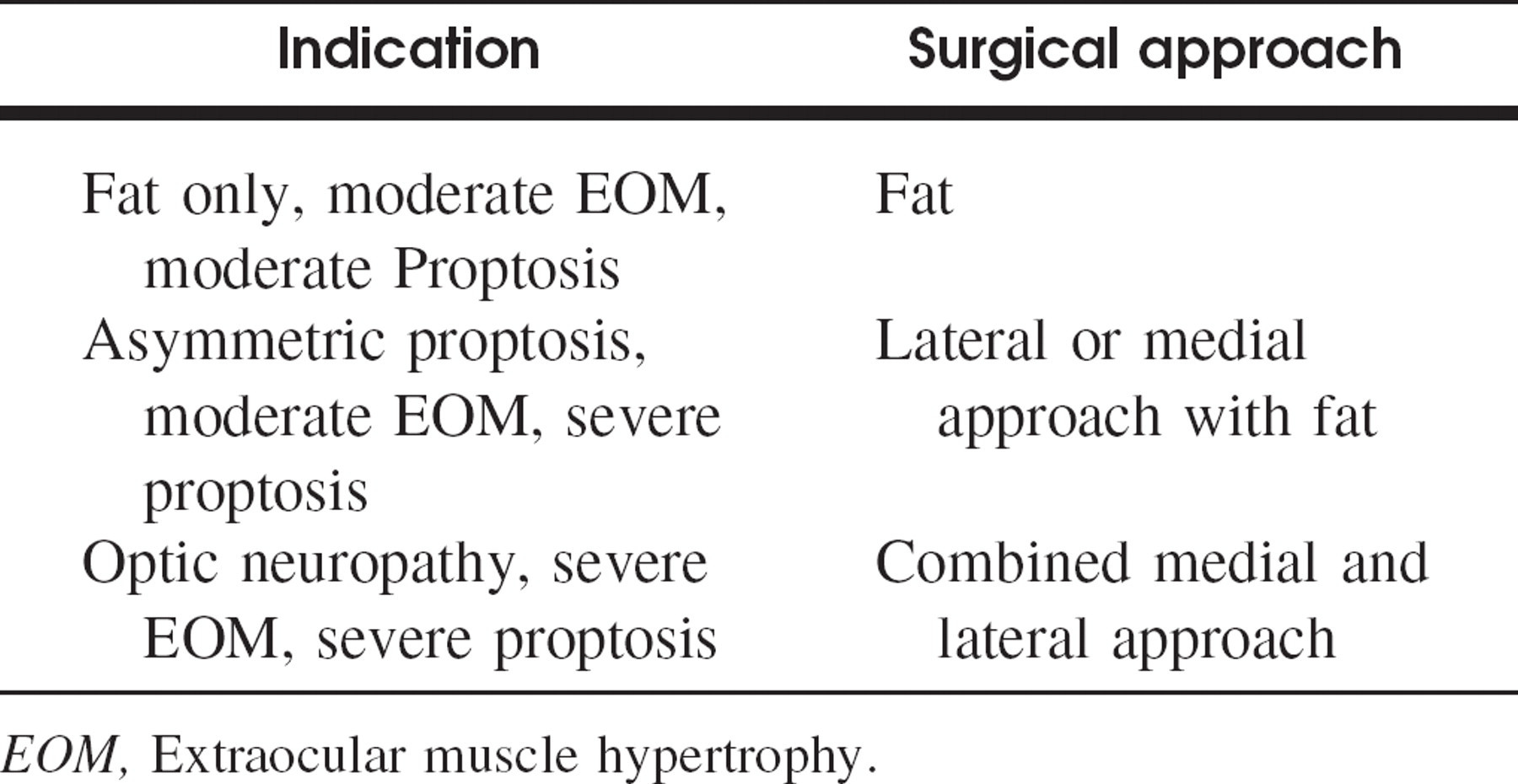
EOM, Extraocular muscle hypertrophy.
RESULTS
Twenty-two orbits in 13 patients underwent bony orbital decompression. Eleven patients were women and 2 were men (mean age, 50.3 years; age range, 26 to 70 years). Indications for decompression were symmetric proptosis in 4 patients, asymmetric proptosis in 4 patients, and optic neuropathy in 5 patients. Hertel measurements of the orbits revealed asymmetric proptosis in 4 patients and symmetric proptosis secondary to severe muscle hypertrophy in 9 patients.
Nine patients (17 orbits) underwent balanced decompression; 4 patients (5 orbits) underwent fat removal and orbital wall decompression on either the medial or lateral wall only (3 lateral and 1 medial-bilateral orbits). The reduction of proptosis achieved with fat and lateral or medial internal decompression was an average of 3.5 mm (range, 3 to 4 mm). With combined endoscopic medial endonasal and lateral internal decompression, the average reduction was 5.9 mm (range, 3 to 10 mm). In all 5 patients, preoperative optic neuropathy was reversed.
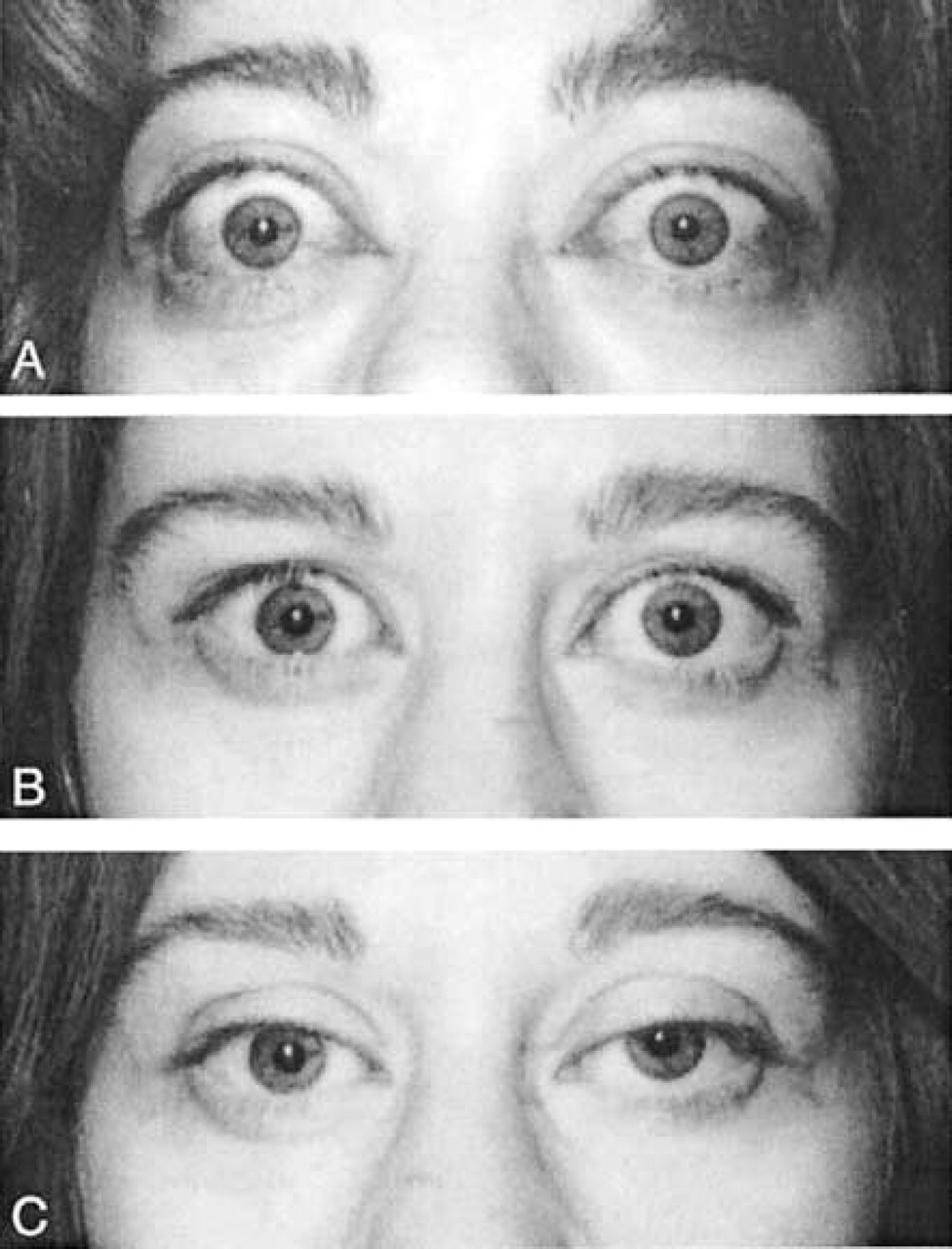
Four patients (30.7%) had preoperative diplopia. Two patients (30.7%) had persistent diplopia (2 of 13, 15.35%), 2 patients had a worsening of diplopia (2 of 13, 15.35%), and 2 patients without preoperative diplopia had new-onset postoperative diplopia (2 of 13, 15.35%) (Table 3). Eight patients underwent lid or extraocular muscle surgery after orbital decompression, to correct diplopia.
DISCUSSION
Graves' orbitopathy can be divided into an acute (active) phase and a chronic (stable) phase. Patients in the active phase can have severe ocular involvement characterized by compressive optic neuropathy. The treatment options include corticosteroids, orbital external beam irradiation, or surgical decompression. In our treatment algorithm, surgical decompression in the acute phase is reserved for patients for whom medical treatment fails or cases in which there is a medical contraindication to these modalities. Less commonly advocated therapies include somatostatin analogs and intravenous immunoglobulins; however, neither of these has proven efficacy. Patients enter the chronic (stable) phase after an average of 1 to 3 years. Mild orbital involvement requires only supportive measures. More severe chronic orbital involvement may require orbital decompression, followed by extraocular muscle or eyelid surgery.
Incidence of preoperative and postoperative diplopia, muscle, and lid surgery
At our institution the surgical management is tailored to the anatomic cause of proptosis (fat compartment versus extraocular muscle hypertrophy), the severity of Graves' orbitopathy, and/or the presence of asymmetry between eyes. 7,8 High-resolution computed tomography or magnetic resonance imaging was performed in all of our patients to define the orbital pathology (Fig 4). In our series, 63 orbits in 32 patients underwent decompression of fat only. Patients with asymmetric proptosis of >5 mm underwent orbital wall and fat removal. Patients with severe proptosis or optic neuropathy underwent combined endoscopic medial endonasal and lateral internal decompression to achieve a balanced decompression (Fig 5).
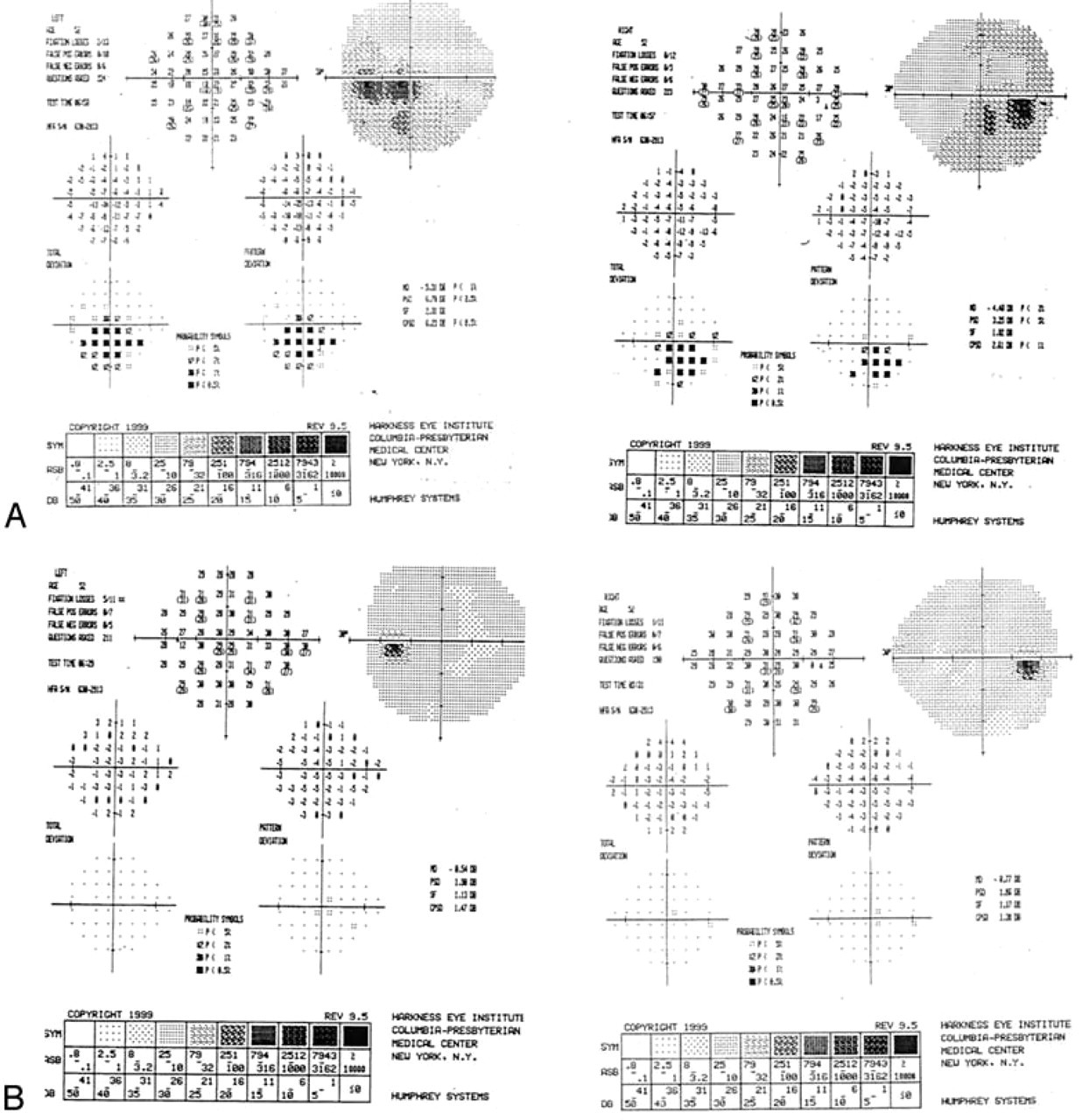
There are several advantages to combined endoscopic medial endonasal and lateral internal decompression. “Balanced” decompression leads to maximal decrease in proptosis and reversal of optic neuropathy when present (average decompression of 5.9 mm in our series). Furthermore, balanced decompression may reduce the incidence of postoperative strabismus and minimizes the need for rehabilitative eye muscle surgery because it does not lead to an inferomedial displacement of the globe (Fig 6). In contrast, solely endoscopic medial and inferior endonasal decompression or transantral decompression has high rates of postoperative diplopia, approaching 66% in some series. 9 It has been noted in the literature that this traditional endoscopic approach produces an asymmetric decompression, with a shift of the globe medially and inferiorly, which may contribute to the higher incidence of new or worsened diplopia. 10 The average reduction of proptosis has been reported as 4.7 mm in the transantral technique group. 9 In studies evaluating only medial endoscopic techniques, the average decrease in proptosis ranged from 3.79 to 4.4 mm. 10–13 Kennedy et al 12 in 1990 reported an average reduction of 4.7 mm; however, in 2 of the 5 orbits studied, the endoscopic approach was coupled with Caldwell-Luc antrostomies. The reduction in proptosis is improved with the addition of lateral orbital approaches 14 (Table 4).

Computed tomography scan (axial and coronal) showing fat and muscle hypertrophy.
Shepard et al 15 in 1998 published their data on “balanced” orbital decompression in 11 patients. The mean reduction of proptosis in their series was 4.6 mm. Two patients had new-onset diplopia (18.2%), and 2 patients required lid or muscle surgery even though 7 patients had persistent or new-onset diplopia. 15 In contrast, our series had a 15.35% incidence of new-onset diplopia, and 8 patients (6 muscle surgeries and 2 lid surgeries) required surgery to correct diplopia or eyelid abnormalities.
Both combined endoscopic medial endonasal and lateral internal decompression and transantral decompression have the advantage of no visible external scar; and each offers maximal access to the orbital apex. 13
A variation of the endoscopic medial and lateral internal decompression or transantral decompression is the transconjunctival or transcaruncular approach. 16 This variation enables removal of the medial and inferior walls with a low incidence of new-onset postoperative diplopia (range, 6% to 41%). However; decompression of the posterior ethmoids and orbital apex is more difficult. A 3-wall orbital decompression can be achieved by combining a transantral approach with a lateral translid approach or a coronal approach. 17 This approach has a lower incidence of diplopia than transantral approach alone. The disadvantages of this approach include less effective decompression of the orbital apex and possible injury to the infraorbital nerve. Kalmann et al 17 achieved an average reduction of proptosis by 4.3 mm using this technique.
A composite picture showing preoperative Hertel measurements of right eye (24 mm) and left eye (25 mm)
Surgical approach and reduction of proptosis
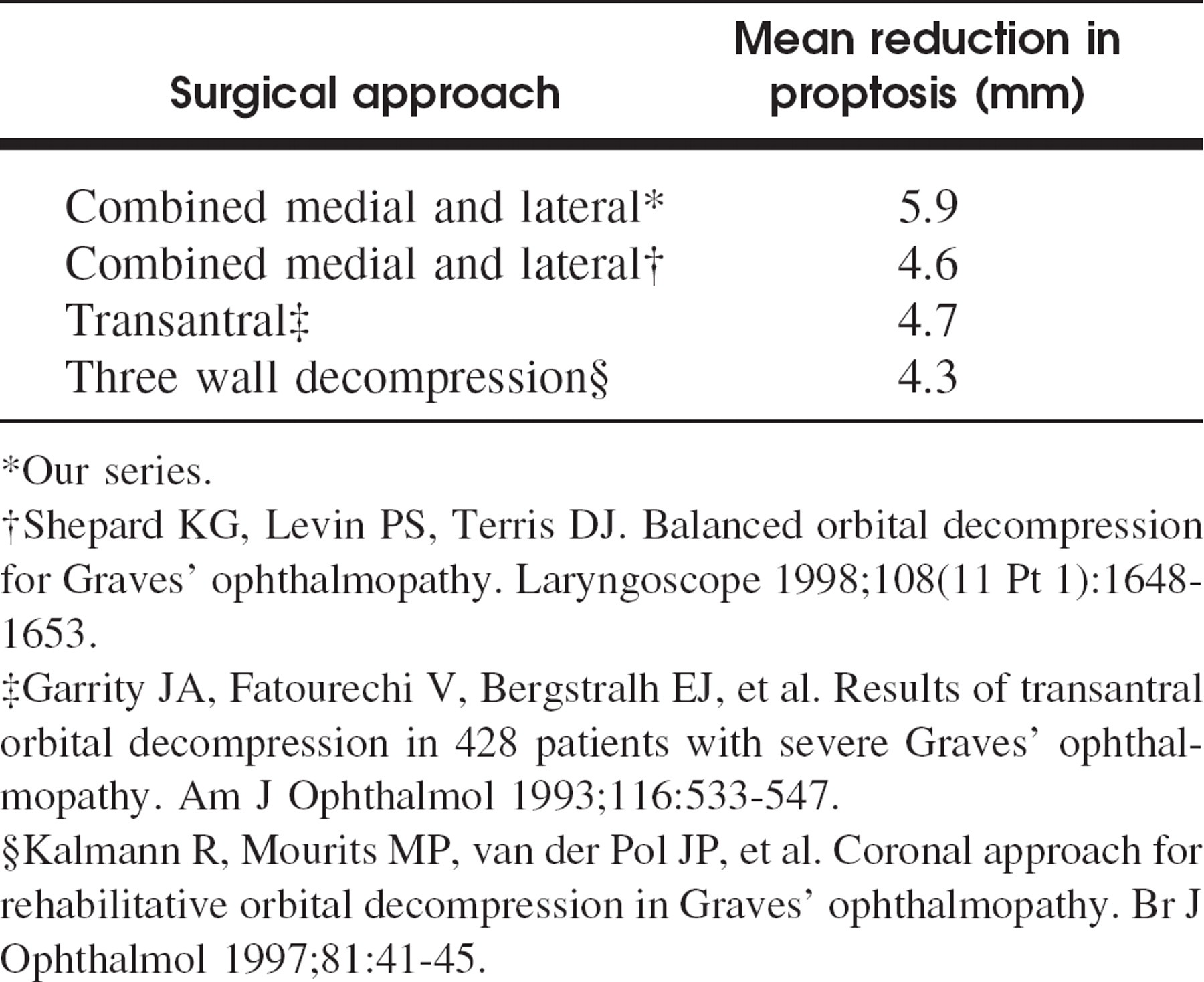
Our series.
Shepard KG, Levin PS, Terris DJ. Balanced orbital decompression for Graves' ophthalmopathy. Laryngoscope 1998;108(11 Pt 1):1648–1653.
Garrity JA, Fatourechi V, Bergstralh EJ, et al. Results of transantral orbital decompression in 428 patients with severe Graves' ophthalmopathy. Am J Ophthalmol 1993;116:533–547.
Kalmann R, Mourits MP, van der Pol JP, et al. Coronal approach for rehabilitative orbital decompression in Graves' ophthalmopathy. Br J Ophthalmol 1997;81:41–45.
Prolapsed orbital contents with patent maxillary and sphenoid ostium.
A 4-wall orbital decompression is reserved for the most severe cases of proptosis (>35 to 40 mm). Although this approach produces the greatest reduction in proptosis, severe complications have been reported in the literature, including intracranial hemorrhage, damage to frontal lobes, meningitis, and pulsatile proptosis. 18,19
Complications are not an infrequent occurrence, with a reported rate of 21% for the conventional transantral approach and 10% for coronal 3-wall decompression. These rates excluded diplopia. 20 In our study, there were no early (bleeding/orbital hematoma) or delayed (sinusitis) complications. The absence of delayed complication of sinusitis may be attributed to the fact that we perform large maxillary, frontal, and sphenoid sinusotomies, which are still patent after the orbital contents have prolapsed into the ethmoid bowl (Fig 7).
CONCLUSION
A balanced orbital decompression can be performed by the combined endoscopic medial endonasal and lateral internal decompression. This technique allows for maximal decompression, including the orbital apex, and has a low incidence of new-onset diplopia. Inferior support is maintained and the incidence of injury to the medial rectus muscle is minimized. The average reduction of proptosis in our series was 5.9 mm. This is the preferred approach of orbital decompression in patients with severe proptosis with optic neuropathy at our institution.