
Abstract

CASE STUDY
A 36-year-old man was seen in the ENT clinic with a long history of chronic allergic rhinitis and nasal congestion refractory to medical treatment including nasal steroid sprays. The patient had previously undergone a septoplasty with bilateral inferior turbinate cauterizations at another facility, which did little to improve the symptoms. After examination and consent, the patient underwent decongestion with topical anesthetic and a vasoconstrictor (2% lidocaine and 0.5% phenylephrine) applied directly to the nasal mucosa in spray form and on cotton pledgets placed in contact with the inferior turbinate and left in place for 5 minutes. A tuberculin syringe was loaded with 1 mL of triamcinolone acetonide (40 mg/mL) and 0.5 mL was slowly injected into the anterior portion of each inferior turbinate with a 25-gauge needle. Blanching of the inferior turbinate mucosa was seen bilaterally.
Within 2 minutes of the injection the patient was noted to have a blanching of the right medial forehead, the right medial canthal area, and the right nasolabial fold. Flushing of the right lateral forehead and right check was also noted. Within 5 minutes of the injection, the patient began to have right-sided ocular pain and blurred vision. Immediate opthalmalogic consultation was obtained, and the patient was found to have multiple end arterial emboli throughout the retinal circulation concentrated about the macula (Figs 1 and 2). Visual acuity at that time was found to be 20/30 in the affected eye. The left eye remained at baseline of 20/16. Flourescein angiography was used to confirm the diagnosis of choroidal and retinal arteriolar embolization, with multiple filling defects in the arteriolar phase of the angiogram and multiple occlusions of the perifoveal retinal capillaries. The patient reported that the ocular discomfort and blurred vision had completely resolved by the following morning. The patient was seen in the ophthalmology department 9 days later for follow-up, and at that time, the right eye visual acuity had returned to 20/16.
DISCUSSION
Visual loss from turbinate injections is a rare but potentially devastating complication. The visual symptoms are transient for most reported cases, but permanent loss of vision has been reported. 5 The estimated incidence rate of visual loss after injection into the inferior turbinates has been estimated at 0.006%. 5 The mechanism of embolization seems to be retrograde flow from the anterior tip of the inferior turbinate, through anastomosis with the anterior and posterior ethmoid arteries to the ophthalmic artery, followed by anterograde flow. The particles then lodge in the end arteries of the choroid and retinal vessels. Larger particle corticosteroids, such as methylprednisone, are thought to present an increased risk. The injection material used in this case was triamcinolone acetonide in which 90% of the particles measure 10 μm or less. Guidelines have been published by McCleve and Goldstein 4 and by Mabry 1 for turbinate injection.
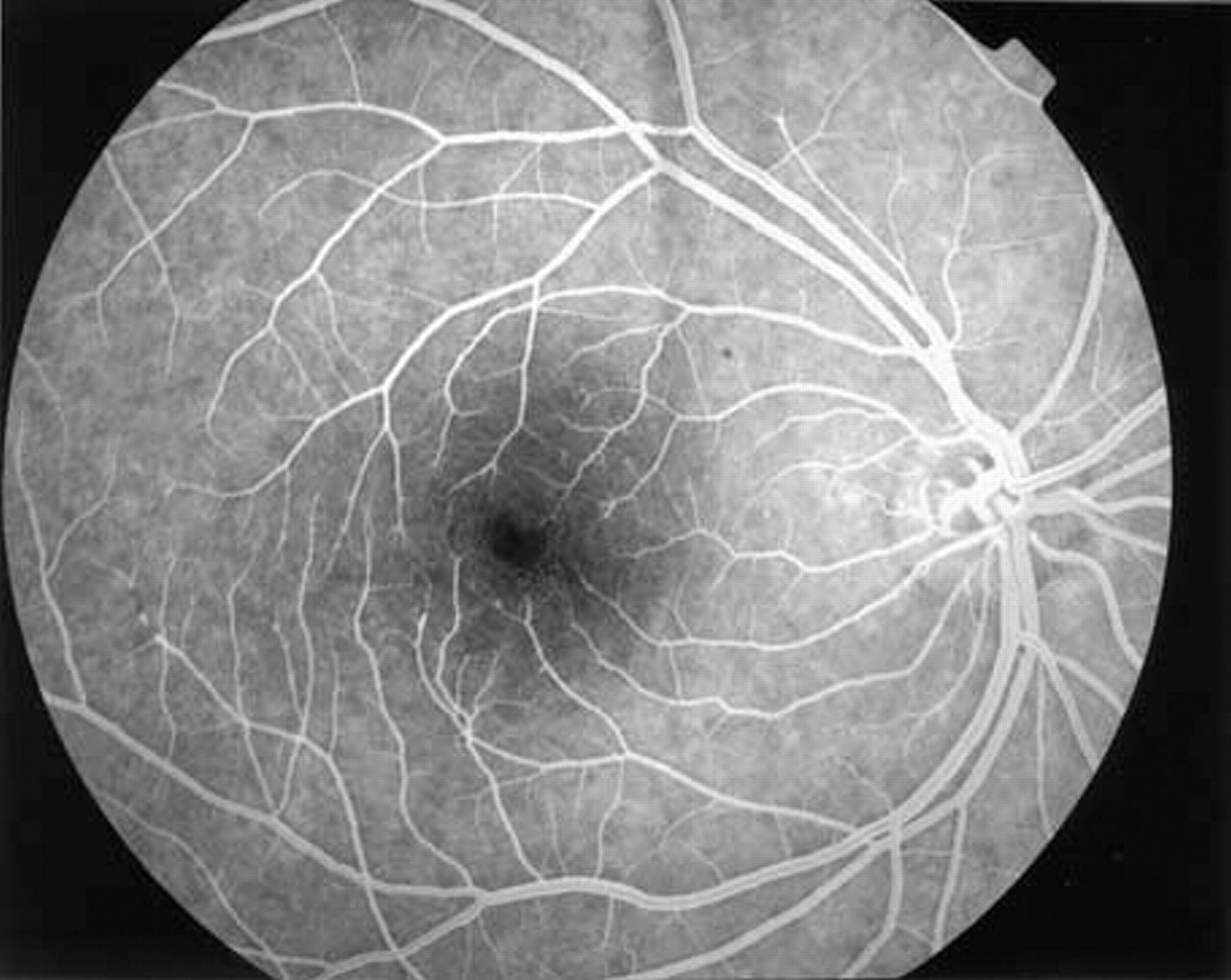
Flourescene angiogram of right retina shows multiple filling defects about macula. Note large filling defect in periphery opposite optic nerve.
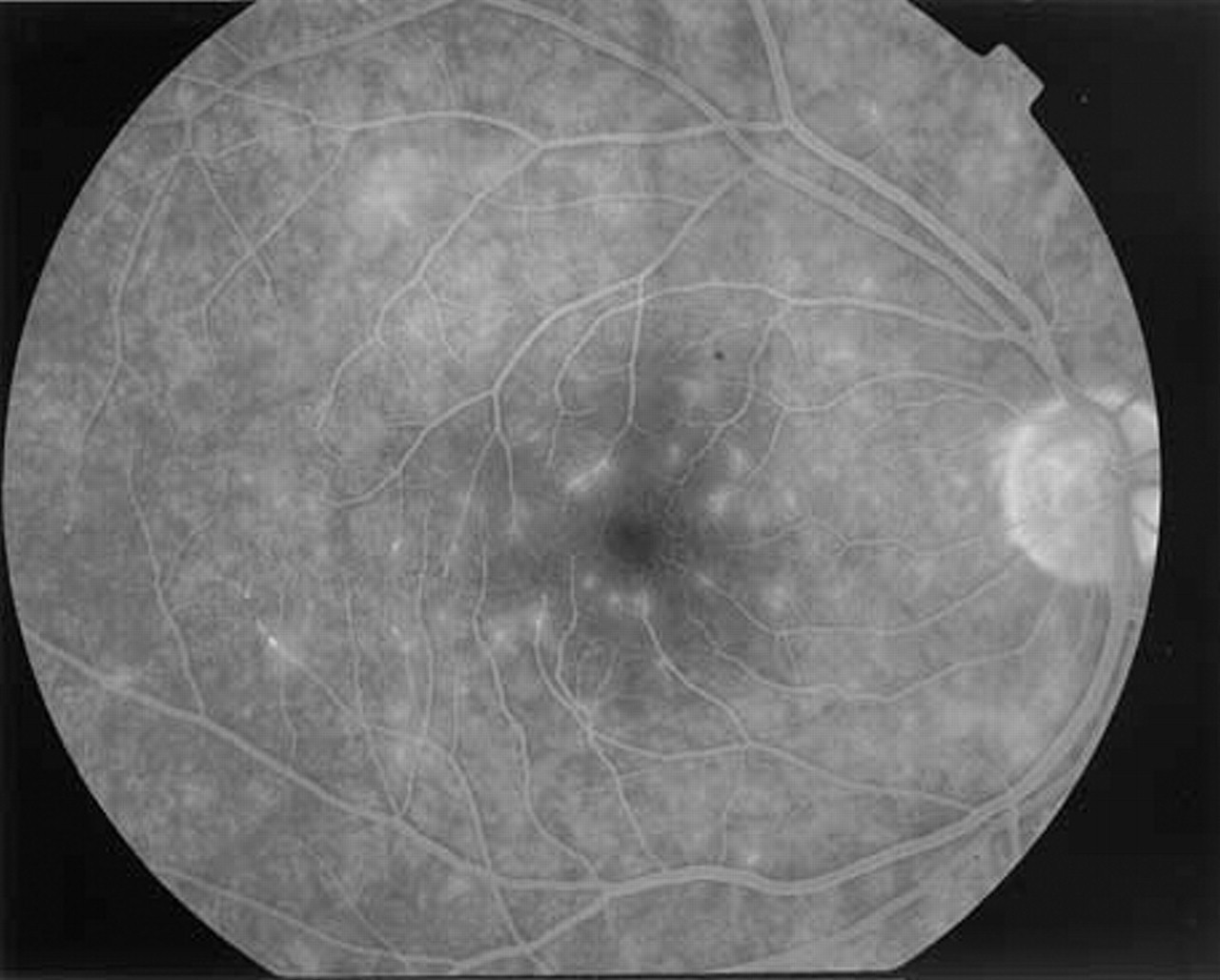
Flourescene angiogram shows multiple emboli as lucent objects in end arterial circulation about macula.