
Abstract
The purpose of this paper is to describe verbal and nonverbal expressions of mutual regulation between patients and therapists through the analysis of relevant episodes of five psychotherapy processes. Microanalyses of discourse, vocal quality and facial expression of emotions were conducted on both patients and therapists in 67 Episodes of Change and 86 Episodes of Rupture of the Therapeutic Alliance. The analyses were carried out using hierarchical regression, showing that both Episodes of Change and Episodes of Rupture correspond to interactional scenarios where patients and therapists use different forms of speech, vocal qualities and facial expressions that account for specific regulation processes which are coherent with such scenarios.
Process-outcome research has focused on techniques and interventions that facilitate psychic change, producing a substantial body of knowledge about some of the ‘active ingredients’ of therapeutic effectiveness. One of the most consistent findings is that the quality of the therapeutic relationship explains much of the positive results of psychotherapy (Orlinsky, Ronnestad, & Willutzki, 2004).
Some authors have conceptualized the therapeutic relationship as a process of mutual regulation where both participants in the dyad negotiate the state of their relationship moment by moment, continually oscillating between states of coordination and lack of coordination (Bänninger-Huber & Widmer, 1999; Beebe & Lachmann, 2002). The members of the dyad display idiosyncratic affective and relational repertoires learned in the context of the significant bonds formed in early childhood and reorganized throughout life through subsequent meaningful relationships. These codes contain generalized procedures of mutual regulation and involve expectations about behaviours and roles that each participant should play during their relational exchange (Tronick & Cohn, 1989). Both participants’ explicit and implicit attempts to regulate the status of the relationship are influenced and affected by the other, in a circular, continuous and dynamic process (Beebe, 2006). This regulatory process is, in turn, expressed through multiple communication channels such as verbal speech, facial behaviour and movement, among others (Beebe & Lachmann, 1994). Despite their diversity and importance, research into mutual regulation and its various expressive channels has mostly focused on nonpsychotherapeutic contexts (mother-baby dyads, Beebe, Knoblauch, Rustin, & Sorter, 2005; nonverbal behaviour in everyday communication between adults, Nagaoka, Komorik, & Yoshikawa, 2007); while studies conducted in a psychotherapeutic context have examined each expression separately, (Ramseyer & Tschacher, 2014) and, in some cases, under experimental conditions (Nagaoka & Komori, 2008).
Verbal and nonverbal aspects of mutual regulation in the therapeutic interaction
According to Bucci (2007), there are two co-existing systems that mutually and continuously affect each other, and that process human experience: the symbolic and sub-symbolic. Symbolic processing is mainly manifested through verbal code through language; it is usually seen as intentional, explicit and conscious. On the other hand, the sub-symbolic system is manifested mostly non-verbally; it houses procedural knowledge that includes organizing principles of relational repertoires, which are implicit, automatic and nonvolitional, mainly operating at an unconscious level (Bucci, 1988). Despite the coexistence of both systems, much of the information exchanged during the therapeutic interaction is manifested tacitly, automatically and at a nonverbal level (Schore & Schore, 2008).
In psychotherapy, communication is formed at an explicit level by exchanging conscious contents, but also through implicit aspects of the subjectivity of the participants who model their forms of speech. Some authors (Hermans, 2001; Raggatt, 2007) have focused their investigations on different subjective states or positions expressed in the discourse of speakers, thus revealing the dialogic nature of the self. These positions are expressed by discursive voices that metaphorically talk to each other in each participant’s intramental space, and are in turn presented in the ‘real’ dialogue that occurs in the intermental space. The way in which the participants’ voices interact and regulate each other continuously shapes the meanings produced in the therapeutic process and regulates, in turn, the multiple interactions (Georgaca, 2014).
Notwithstanding the foregoing, the implicit dimension is mainly expressed nonverbally, made up of patient’s and therapist’s unconscious experiences and communication, which can be expressed through prosody, facial expressions and body movements. The available evidence shows that nonverbal coordination and communicative synchrony relate to aspects such as the ‘success’ of the interaction, rapport, and empathy, all of which are associated with regulatory processes (Cappella & Schreiber, 2006). In this regard, and in a psychotherapeutic context, the issues that have been mostly studied are body movements (Nagaoka & Komori, 2008; Ramseyer & Tschacher, 2014), facial expressions (Bänninger-Huber, 1992; Sharpley, Jeffrey, & Macmah, 2006), voice and vocal quality (Rice & Kerr, 1986; Tomicic, Martínez, Chacón, Guzmán, & Reinoso, 2011) and silences (Frankel & Levitt, 2008).
Considering the above, the purpose of this study was to describe the verbal and nonverbal characteristics of the mutual regulation processes between patient and therapist, in order to deepen knowledge on the aspects of the interaction involved in building a relationship that is favourable to therapeutic change.
If one considers that psychotherapy is a heterogeneous process that takes a nonlinear course, research into mutual regulation as an inherent process in the development and maintenance of the therapeutic relationship can be conducted by observing relevant episodes in therapy sessions (Elliott, 2010). Thus, this paper presents the results of a microanalysis conducted into verbal and nonverbal manifestations in the mutual regulation of Episodes of Change (EC; Krause et al., 2006) and Episodes of Rupture (ER; Safran & Muran, 2006) of the therapeutic alliance, considering them to be interactional scenarios (Martínez, Tomicic, & Medina, 2012) that are relevant to the development of the psychotherapeutic process.
Methodology
Participants
Description of the psychotherapy process and relevant episodes.
Notes: The diagnosis was reported by each therapist. E = Episode. Result: Therapeutic success was defined using the criteria from the Reliable Change Index (RCI = 17 or more) (von Bergen & de la Parra, 2002). aThe first 20 sessions in the psychotherapeutic process were analysed in this study; 45 episodes were identified during this psychotherapy process period. bThis psychotherapy was restarted after 4.5 months of suspension. The 31 coded sessions belong to the first period of treatment of care (RCI was evaluated in session 31).
The mean age of the patients was 34.7 years (SD = 12.1). On average, there were 32.8 (SD = 6.4) therapy sessions. The therapists, three men and two women, had between three and 15 years’ professional experience. All treatments were evaluated with the Outcome Questionnaire 45.2 (OQ-45.2, Lambert et al., 1996; von Bergen & de la Parra, 2002). The research was approved by the Bioethics Committee at the Universidad Diego Portales and each patient authorized their participation in the study by signing an informed consent form.
Procedures
All sessions were audio- and video-taped for their subsequent analysis. They were coded by trained raters using two sequential procedures: (a) Determination of relevant episodes and (b) Coding of the discourse, voice and facial expression of the therapist and the patient.
Determination of relevant episodes
Relevant episodes are defined as special segments in the therapy session (Elliott, 1984) that facilitate comprehension of the connection between the therapy exchange and its result. In this study, Episodes of Change (EC; Krause et al., 2006) and Episodes of Rupture (ER; Safran & Muran, 2006) were used.
An EC is an interaction segment where a moment of change occurs. In the coding process, this moment marks the end of an episode. The beginning of the episode is established by identifying the moment when participants begin to talk about the content of the change (Krause, 2005).
An ER is an interaction segment where communication markers are identified that show a breakdown of the therapeutic alliance generated by the patient, either because of withdrawal or confrontation (Eubanks-Carter, Muran, & Safran, 2009). Its onset is established with the first communicative signs of rupture and ends with the first signs of resolution or improvement.
To determine the episodes, five pairs of trained coders analysed the session videos and transcripts. Their codings were validated through intersubjective agreements (see Flick, 2009). Examples of relevant episodes of change and rupture coded in this study are shown in Appendix 1.
Coding of discursive positions (DP)
The Discursive Positioning Model (DPM, Martínez, Tomicic, Pérez, Altimir, & Krause, 2014) was used for the analysis of therapists and patients’ discourse. The purpose of this system is to identify discursive positions in participants’ speech. In the case of patients they are: (a) Reflexive, which is marked by emotional distance from situations, a balance between affects and perspectives and the ability to listen and critically look at their other positions; (b) Dependent, in which they position themselves subjectively as dependent, weak damaged and/or vulnerable; (c) Independent, associated with a self-sufficient discourse expressing that they do not require the help of others. In the case of therapists, discursive positions are: (a) Proposer, establishing themselves as able to show the patient what they observe, offering them a new perspective and creating a space to dialogue about their positions; (b) Professor, associated with a dominant and monologic dialogue, bearer of a truth or knowledge that is imposed and taught as the only alternative.
The coding was done by two judges who followed three microanalytical steps: (a) identification of ‘discursive voices’ associated with recurring enunciators in the therapist’s and the patient’s speech; (b) categorization of the discursive voices of each patient and therapist as idiosyncratic discursive positions; (c) classification of idiosyncratic discursive positions according to the DPM.
Inter-rater reliability was evaluated considering all episodes (n = 153, 6,575 segments), yielding a k = .762, p < .05 (Cohen, 1968).
Coding vocal quality patterns (VQP)
Two trained coders applied the VQP coding system (Tomicic et al., 2011), categorizing the patient’s and therapist’s speech into the following categories: (a) Report (speech conveys emotional distance, reporting content without emotional commitment); (b) Connected (speech transmits an elaborative quality and orientation towards the interlocutor); (c) Affirmative (speech transmits the quality of certainty and conviction, of instruction and commitment to what is being said); (d) Introspective (speech transmits the quality of introspection); and (e) Emotional (speech transmits an emotional quality, either expressive or contained).
Coding is performed following the four steps outlined in the VQP manual (Tomicic et al., 2009), adhering to standardized procedure. The Kappa value obtained for all episodes (n = 153, 4,553 segments) was k = .658, p < .05.
Coding facial expression categories (FEC)
The Facial Action Coding System (FACS; Ekman & Friesen, 1978), which identifies 44 facial action units, was used. Each episode was divided into segments of 25 video frames per second. In each frame, the presence and type of facial action for patient and therapist was coded.
The FEC are: (a) Basic Emotions: positive (joy) and negative (anger, sadness, fear, disgust and contempt); and (b) Unspecific Facial Behaviours: gaze (eye contact with the speaker), adapters (contact of one part of the body or face with another part of the face) and control processes (non-specific actions centred around the mouth).
The coding was carried out by three trained judges. The Interrater reliability between judge 1 and raters 2 and 3 in 25% of the sample (N = 14) was calculated. Reliability was adequate for gaze (k = .65, p < .01 for raters 1 and 2 and k = .73, p < .01 for raters 1 and 3) and for adapters (k = .86, p < .01 for raters 1 and 2 and k = .87, p < .01 for judges 1 and 3) was adequate, but it was insufficient in the case of basic emotions (values between k = .21 and k = .52).
Results
Patients’ and therapists’ discursive positions in episodes of change and rupture.
Patients and therapists’ vocal quality patterns in episodes of change and rupture.
Presence of regulatory facial behaviour in episodes of change and rupture in patients and therapists.
Note: aDifferences in total number of frames for Gaze, Control and Adapters are due to noncodable video sequences.
For the statistical evaluation of verbal (DP) and nonverbal (VQP and FEC) interaction modes, a model that considered the nested nature of the data was used. Each variable was dichotomized. For example, when the patient speaks from a Reflexive DP, the variable takes the value = 1 and when he/she speaks from an Independent and Dependent DP it acquires the value zero. Thus, the probability of occurrence of each dichotomized DP is compared according to the type of episode. For this a Logistic Hierarchical Regression Analysis (HLM 7.0) was conducted, using the PLQ estimation method, with a Bernoulli distribution (level 1). A three-level model was established: Level-1 (turn taking); Level-2 (episode); and Level-3 (complete psychotherapy for each patient).
The procedure considered: (a) the estimation of the non-conditional model to establish the presence of variability to be accounted for in the dependent variable; (b) the incorporation of level-1 predictor(s), modelling the evolution of variables throughout episode, that is, within the numerical ‘turn-taking’ sequence that begins at ‘Zero’ 1 and increases by one each time a turn elapses; (c) the incorporation of significant level-1 predictors (Intercept and/or gradient associated with the evolution within the episode) as ‘random effects’ at level-2, to determine variation according to type of episode. The variable Type of Episode (ER = 0, EC = 1) was modelled as a predictor of level-2 as it explained variability. Additionally, the variable Session, which accounts for the moment in the psychotherapy session where episodes occur (operationalized as session number) was incorporated only as a predictor of intercept (if it revealed significant variability). Finally, (d) the variable Patient’s Level of Functioning was added to level-3, distinguishing whether the patient was in the functional (1) or dysfunctional (0) population at the beginning of psychotherapy; it was considered as control variable of the intercept if it explained variance in the model. The intercept was modelled first (with level 2 and 3 predictors 2 ), followed by the slope associated with the course of the episode.
A similar procedure was used with dichotomized VQP, incorporating as level-1 predictors the variable that accounts for the evolution of the episode and the variable Actor, which identifies the speaker (1 = Patient 0 = Therapist), along with the interaction between both variables. Unspecific Facial Behaviours were dichotomized (Presence = 1, Absence = 0) in patients and therapists respectively. Basic Emotions were also dichotomized, but using as coding universe only those time frames when their presence was identified. In these models, the predictor ‘evolution throughout the episode’ (level-1) was operationalized as the time sequence of frames (25-second-long segments), assuming the value of zero in the initial frame and increasing by one point as each frame elapsed during the episode.
Model parameters (HLM): discourse, voice and facial expression according to type of episode.
Notes: aLevel-1 N = 1,917 (Patients) & N = 1,795 (Therapists), Level-2 N = 196, Level-3 N = 5. bLevel-1 N = 2,632 (Patients & Therapists), Level-2 N = 132, Level-3 N = 5; cLevel-1 N = 6,974 (Therapists) & N = 7,454 (Patients), Level-2 N = 54, Level-3 N = 5. Type of Episode 0 = Episode of Rupture compared with 1 = Episode of Change. Patient operating level = functional (1) or dysfunctional (0) Population. Actor: 1 = Patient 0 = Therapist. N/A = Not applicable. dCoefficients range (γ) and its errors (ES) are presented in brackets in the fixed effects; the Odds Ratios are presented below and their confidence interval (95% CI). eVariables centred with regard to the Grand Average. fEstimated Logit Model (y) = G000 + G010 *Session+ G020 *Type of Episode + G100 *Evolution (during episodes) + G110 *Type of Episode *Evolution + r0 + r1 (Evolution during episode) + u00. gEstimated Logit Model (y) = G000 + G010 *Type of Episode + G100 *Actor + r0 + u00. hEstimated Logit Model(y) = G000 + G100*Actor + G200* Evolution (during episodes) + G300* Evolution (during episodes)* Actor + r0 + u00. i Emotional VQP considered Expressive Emotional (73%) and Emotional Content (27%). jEstimated Logit Model (y) = G000 + G010 Episode Type + G100 * Evolution (during episodes) + r0 + r1 (Evolution during episode) + u°°. kEstimated Logit Model (y) = G000 + G010 *Episode Type + G100 *Evolution (during episodes) + G110 Episode Type * Evolution (during episodes) r0 + r1 (Evolution during episode) + u00. *p < .05; **p < 0.01; ***p < 0.001.
Discursive positions
The patient’s Reflexive DP is more likely at the start of EC, increasing as the episode elapses. As shown in Figure 1 (quadrant a), at the ‘moment of change’ (which happens at the end of the Episode of Change) the patient is most likely to interact from this position, in contrast to what occurs in the ER.
Probability of occurrence of discursive positions and categories of facial expression throughout the episodes.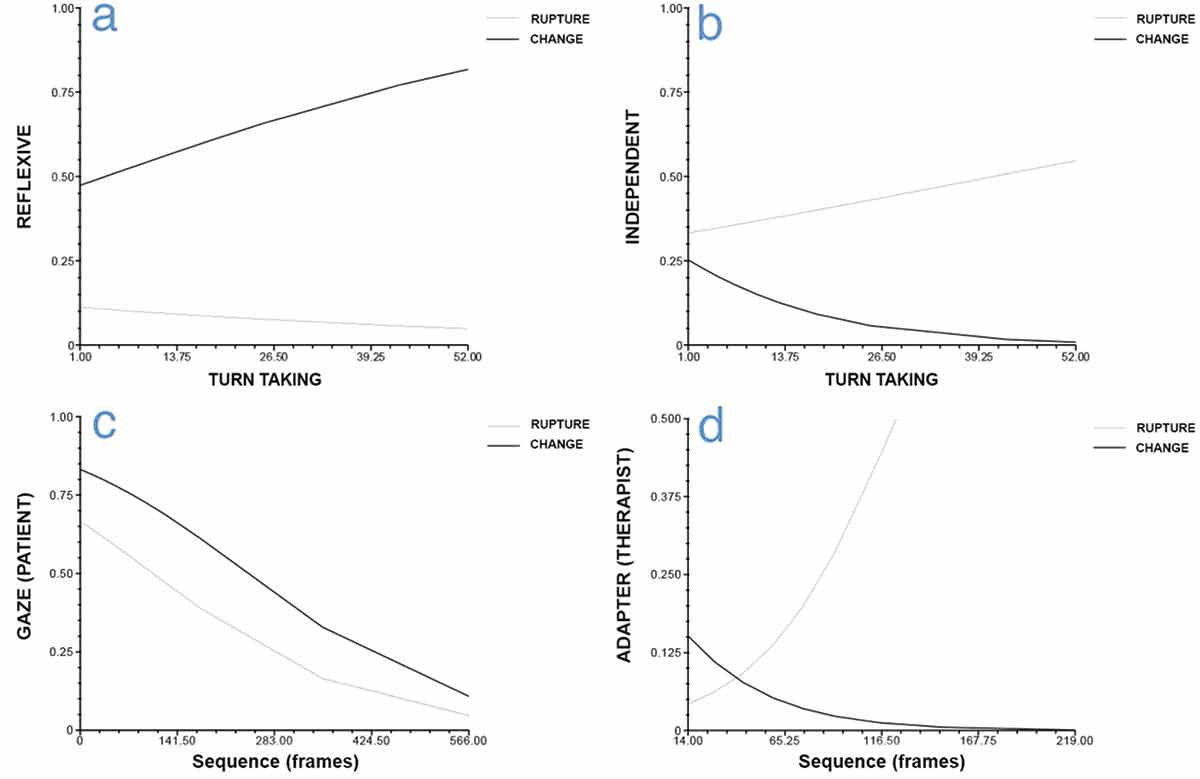
In the case of the Independent DP, although the likelihood for the patient to interact from this DP is similar at the start of both types of episodes, the probability increases as ER elapses and decreases as EC elapses (Figure 1 quadrant b).
No differences associated with episode type were observed regarding the likelihood for the patient to interact from the Dependent DP and for the therapist to do so from the Proposer and Professor DPs.
Vocal quality patterns
The results indicate that only the Report VQP varies depending on the type of episode once the variability associated with the speaker is controlled for. Thus, a higher probability of occurrence of the Report VQP in ER compared to EC (OR 0.65, 95% CI 0.43–0.98) is observed. Furthermore, it can be seen that as the episode elapses, the probability for the patient to use the Emotional VQP increases in both EC and ER, while the probability for the therapist to use the same VQP remains low throughout the whole episode.
Unspecific facial behaviours and basic emotions
The probability of gaze in patients and adapters in therapists depends on the type of episode. The patient is more likely to look at the therapist in EC. However, this probability decreases during both types of episodes (Figure 1, quadrant c). Meanwhile, the probability of adapters in the therapist decreases during in EC and, in contrast, increases during ER (Figure 1, quadrant d).
Discussion
This research describes the discursive, vocal and facial expression features that characterize the verbal and nonverbal forms of regulation between patient and therapist in two interactional scenarios that are relevant for the psychotherapeutic process. The results show that the use of micro-analytical techniques such as the Discursive Positioning Model, Vocal Quality Patterns and Facial Expression Categories facilitate discriminating and differentiating relevant aspects of the therapeutic interaction to understand the regulatory phenomena from a multidimensional approach. In particular, interactional change and rupture scenarios have allowed us to observe these regulatory phenomena, highlighting the different functions that speech, vocal quality and facial gesture play in the process.
In the case of episodes of change, it was observed that patients, as they move further forward in the episode and approach a verbalization that manifests a change in how they understand themselves and their problems, talk less from an independent discursive position, suggesting a subjective positioning of greater openness to dialogue. This occurs in conjunction with a type of speech that emerges from reflexive discourse (i.e., a reflexive discursive position), suggesting the emergence of a regulatory phenomenon among discursive positions, favouring the adoption of a position that listens and critically evaluates their own behaviour (Martínez et al., 2014).
In the case of the therapist, no predominance of one of the two discursive positions was observed. In this regard, it is possible to hypothesize that their speech is organized upon the basis of their role, adapting moment by moment to the relational offer made by the patient at that time, regardless of whether the interactional scenario is an episode of change or rupture (see Tomicic, Martínez, & Krause, 2014).
This coincides with what is pointed out by Stiles, Hill, and Elliott (2015), who propose that the therapist tends to assume a responsive role, designed to fit the needs of the patient.
Patients’ vocal expression during episodes of change was usually characterized by an emotional quality, however, this speech pattern was consistently less frequent for therapists during this kind of episode. This result is consistent with findings that reveal the implicit expressive differences between the roles of patient and therapist (Tomicic et al., 2014). Assuming that change is a moment of the therapeutic process that deeply impacts the patient's subjective theories (Krause, 2005), the emotional sound of their speech may reveal an attempt to self-regulate emotions associated with the emotional intensity that is characteristic of such episodes. As a consequence, it could be hypothesized that therapists hardly use this vocal quality pattern because they offer support by maintaining a speech that, at this level, neither becomes coupled with that of the patient nor is influenced by it.
Regarding facial expressions, patients tended to look more at therapists during these types of episodes, but as they approached the moment of change this behaviour decreased. While gaze has different communication and regulatory functions during the therapeutic interaction (Merten, 1997), it can be assumed that in the context of an episode of change, during which a transformation of meanings and thus a positive affective experience takes place, gaze serves to carry out complementary regulation functions (Bänninger-Huber & Widmer, 1999). So, initially looking at the therapist may serve to indicate that the emotion expressed is addressed to the interaction partner or the interaction itself, which is starting to shape a transformation of meanings. In other words, the patient appears to be emotionally involved in an interaction that is ‘producing’ something. For its part, the gradual withdrawal of the gaze as the moment of change is approached could indicate a shift in the patient’s emotional involvement and in the direction of his/her affection towards the content of the verbal narration (i.e. the content of the change) and towards the self, i.e., towards where the transformation of meanings takes place.
It was observed that as the episode of change occurs, therapists’ use of adapters diminishes, indicating less emotional stress (With & Kaiser, 2009). While more evidence is required to precisely interpret this finding as a regulatory phenomenon, it may fulfill a positive role in regard to change, to the extent that it would encourage the patient to perceive the therapist as someone who is adopting a more responsive and emotionally available role.
During episodes of rupture, patients tended to interact from the independent discursive position, which is associated with a subjective position of self-sufficiency and rejection of help from others, which would account not only for the relational distance in moments of therapeutic impasse, but, as described by Allen and Fonagy (2006), could demonstrate a patient’s regulatory strategy when faced with the recognition of an experience of misunderstanding or a feeling of distance from the other. As in episodes of change, no specific discursive position was found to predominate among therapists, thus reinforcing the hypothesis regarding the exercise of their role.
As in episodes of change, during episodes of rupture patients talked more frequently with the emotional pattern of vocal quality. However, in this interactional scenario, patient and therapist expressed themselves most frequently with the report vocal quality pattern. The use by patients of these two contrasting patterns of vocal quality, one disaffected and the other emotionally engaged, could be associated with an attempt to self-regulate their own negative affects in a scenario of rupture of the therapeutic alliance (Tomicic et al., 2014). Although this hypothesis requires further evidence, it is consistent with the sonority of the therapist’s voice, such that a disaffected vocal quality would serve a regulatory function whose purpose is to address the effects of the rupture in the relationship.
Consistent with what has been described so far, self-regulatory and mutual regulation efforts by patients and therapists in such episodes are also observed at a facial expression level. The former decrease eye contact, while the latter increase their use of adapters, which suggests that both participants are taking actions that help express, manage or relieve tension.
Despite their importance, the results of this study reflect only a sample of episodes nested in a small number of psychotherapies that, in turn, are heterogeneous in their approach, duration and diagnosis. Therefore, it is a task for future studies to answer questions concerning how the extension of the therapies or the severity and chronicity of the patients’ conditions may influence the regulatory processes between the participants and the verbal and nonverbal manifestations of such processes.
Manifestaciones verbales y no verbales de la regulación mutua en episodios relevantes de psicoterapia
La investigación de proceso-resultado se ha centrado en el estudio de las técnicas e intervenciones facilitadoras del cambio psíquico, produciendo un importante corpus de conocimiento sobre algunos de los ‘ingredientes activos’ de la efectividad terapéutica. Uno de los hallazgos más consistentes es que la calidad de la relación terapéutica explicaría una buena parte de los resultados positivos de la psicoterapia (Orlinsky, Ronnestad, & Willutzki, 2004).
Algunos autores han conceptualizado la relación terapéutica como un proceso de regulación mutua en el que ambos participantes de la díada negocian momento a momento el estado de la relación, oscilando continuamente entre estados de coordinación y descoordinación (Bänninger-Huber & Widmer, 1999; Beebe & Lachmann, 2002). Los miembros de la díada despliegan repertorios afectivos y relacionales idiosincrásicos aprendidos en el contexto de los vínculos significativos de la temprana infancia y reorganizados a lo largo de la vida a través de relaciones significativas posteriores. Estos repertorios contienen procedimientos generalizados de regulación mutua e involucran expectativas acerca de los comportamientos y roles que cada participante debiera adoptar en el intercambio relacional (Tronick & Cohn, 1989). Los intentos, explícitos e implícitos, de cada participante de la díada por regular el estado de la relación son influidos y afectados por los del otro, en un proceso circular, continuo y dinámico (Beebe, 2006). Este proceso de regulación a su vez se expresa a través de múltiples canales de comunicación tales como el discurso verbal, la conducta facial, el movimiento, entre otros (Beebe & Lachmann, 1994). No obstante su diversidad e importancia, la investigación en la regulación mutua y sus diversos canales expresivos se ha centrado en ámbitos no psicoterapéuticos (díadas madre-bebé, Beebe, Knoblauch, Rustin, & Sorter, 2005; conducta no verbal en la comunicación cotidiana entre adultos, Nagaoka, Komorik, & Yoshikawa, 2007) y, en las realizadas en el contexto psicoterapéutico se ha estudiado cada canal de expresión por separado (Ramseyer & Tschacher, 2014) y, en algunos casos, en condiciones experimentales (Nagaoka & Komori, 2008).
Aspectos verbales y no verbales de la regulación mutua en la interacción terapéutica
Según Bucci (2007), hay dos sistemas coexistentes que se afectan de manera mutua y continua, y que procesan la experiencia humana: el simbólico y el sub-simbólico. El procesamiento simbólico se manifiesta principalmente mediante el código verbal a través del lenguaje, que suele presentarse de manera intencional, explícita y consciente. Por otro lado, el sistema sub-simbólico se manifiesta mayoritariamente de forma no-verbal, alberga el conocimiento procedural que incluye principios organizadores de repertorios relacionales, los que son de carácter implícito, automático, y no volitivo, operando fundamentalmente a nivel no-consciente (Bucci, 1988). No obstante la coexistencia de ambos sistemas, gran parte de la información que se intercambia durante la interacción terapéutica se manifiesta de manera tácita, automática y a nivel no verbal (Schore & Schore, 2008).
En psicoterapia, la comunicación se conforma por el nivel explícito mediante el intercambio de contenidos conscientes, y también por aspectos implícitos de la subjetividad de sus participantes que modelan sus formas de habla. Algunos autores (Hermans, 2001; Raggatt, 2007) se han interesado por indagar los diferentes estados o posiciones subjetivas expresadas en el discurso de los hablantes y que revelan la naturaleza dialógica del self. Estas posiciones son manifestadas mediante voces discursivas que, metafóricamente, dialogan entre sí en el espacio intramental de cada participante y, a la vez, se presentan en el diálogo ‘real’ que ocurre en el espacio intermental. La forma en que las voces de los participantes interactúan y se regulan entre sí moldean continuamente los significados producidos en el proceso terapéutico y regulan, a su vez, las múltiples interacciones (Georgaca, 2014).
No obstante lo anterior, la dimensión implícita se expresa mayoritariamente de forma no verbal, comprendiendo experiencias y comunicaciones no conscientes de parte de paciente y terapeuta, que pueden ser expresarse mediante la prosodia, la expresividad facial y los movimientos corporales. La evidencia disponible muestra que la coordinación y sincronía comunicativa no verbal se relaciona con el ‘éxito’ de la interacción, el rapport y la empatía, aspectos asociados a los procesos regulatorios (Cappella & Schreiber, 2006). Al respecto, y en contexto psicoterapéutico, se han estudiado mayormente los movimientos corporales (Nagaoka & Komori, 2008; Ramseyer & Tschacher, 2014), expresiones faciales (Bänninger-Huber, 1992; Sharpley, Jeffrey, & Macmah, 2006), la voz y cualidad vocal (Rice & Kerr, 1986; Tomicic, Martínez, Chacón, Guzmán, & Reinoso, 2011) y los silencios (Frankel & Levitt, 2008).
Considerando lo planteado, el objetivo de este estudio fue describir las características verbales y no verbales de los procesos de regulación mutua entre paciente y terapeuta, con el fin de profundizar en el conocimiento sobre los aspectos de la interacción que participan de la construcción de una relación terapéutica favorecedora del cambio.
Si se considera que la psicoterapia es un proceso heterogéneo de curso no lineal, la indagación de la regulación mutua como proceso inherente al desarrollo y mantención de la relación terapéutica puede realizarse mediante la observación de episodios relevantes en las sesiones de terapia (Elliott, 2010). Así, el presente artículo presenta los resultados del microanálisis de manifestaciones verbales y no verbales de la regulación mutua en Episodios de Cambio (EC; Krause et al., 2006) y en Episodios de Ruptura de la alianza terapéutica (ER; Safran & Muran, 2006), considerándolos como escenarios interaccionales (Martínez, Tomicic, & Medina, 2012) relevantes en el desarrollo del proceso psicoterapéutico.
Método
Participantes
Descripción del proceso de psicoterapia y episodios relevantes.
Notas: El diagnóstico fue reportado por cada terapeuta. E = Episodio. Resultado: éxito terapéutico fue definido a partir del criterio de Índice de Cambio Confiable (ICC = 17 o más) (von Bergen & de la Parra, 2002). aLas primeras 20 sesiones del proceso psicoterapéutico completo fueron analizadas en este estudio; 45 Episodios fueron identificados en este periodo del proceso de psicoterapia. bEsta Psicoterapia fue reiniciada tras 4.5 meses de suspensión. Las 31 sesiones codificadas corresponden al primer periodo de atención (ICC fue evaluado en la sesión 31).
La media de la edad de los pacientes fue de 34.7 años (DS = 12.1). En promedio, las terapias fueron de 32.8 (DS = 6.4) sesiones. Los terapeutas, tres hombres y dos mujeres, tenían entre tres y 15 años de experiencia profesional. Todos los tratamientos fueron evaluados con el Outcome Questionnaire 45.2 (OQ-45.2, Lambert et al., 1996; von Bergen & de la Parra, 2002). La investigación contó con la aprobación del comité de bioética de la Universidad Diego Portales y cada paciente autorizó ser parte de este estudio mediante la firma de un consentimiento informado.
Procedimientos
Todas las sesiones fueron grabadas en audio y video para su análisis. Éstas fueron codificadas por jueces entrenados usando dos procedimientos secuenciales: (a) Determinación de episodios relevantes; y (b) Codificación del discurso, la voz y la expresión facial de terapeuta y paciente.
Determinación de episodios relevantes
Los episodios relevantes son segmentos especiales de la sesión terapéutica (Elliott, 1984) que hacen posible comprender la conexión entre el intercambio terapéutico y su resultado. En este estudio se utilizaron Episodios de Cambio (EC; Krause et al., 2006), y Episodios de Ruptura (ER; Safran & Muran, 2006).
Un EC es un segmento de interacción donde ocurre un momento de cambio. En el procedimiento de codificación, este momento marca el final de un episodio. El inicio del episodio se establece identificando el momento en que los participantes comienzan a hablar acerca del contenido del cambio (Krause, 2005).
Un ER es un segmento de interacción donde se identifican marcadores de comunicación que evidencian una ruptura de la alianza terapéutica por parte del paciente, ya sea por retirada o confrontación (Eubanks-Carter, Muran, & Safran, 2009). Su inicio se establece con los primeros indicios comunicativos de ruptura y su final con los primeros indicios de su resolución o superación.
Para determinar los episodios, cinco pares de codificadores entrenados analizaron videos y transcripciones de las sesiones. Sus codificaciones fueron validadas por medio de acuerdos intersubjetivos (ver Flick, 2009). En el Apéndice 1 se muestran ejemplos de episodios relevantes de cambio y ruptura codificados en este estudio.
Codificación de posiciones discursivas (PD)
Para el análisis de discurso de pacientes y terapeutas se utilizó el Modelo de Posicionamiento Discursivo (MPD, Martínez, Tomicic, Pérez, Altimir, & Krause, 2014). El sistema tiene por objeto identificar posiciones discursivas en el habla de los participantes. En el caso de los pacientes éstas son: (a) Reflexiva, asociada a un posicionamiento desde la toma de distancia emocional de las situaciones, equilibrando afectos con perspectivas, y siendo capaz de escuchar y mirar críticamente las otras posiciones de sí mismo; (b) Dependiente, posicionándose subjetivamente como alguien dependiente, débil, dañado y/o vulnerable; y (c) Independiente, asociada a un discurso de auto-suficiente, que no requiere de la ayuda de los otros. En el caso de terapeutas, las posiciones discursivas son: (a) Propositiva, instalándose éstos desde la capacidad para mostrar al paciente lo que observa, ofreciéndole una nueva perspectiva y generando un espacio dialógico para las posiciones del paciente; y (b) Profesor, asociado a un discurso dominante y monológico, portador de una verdad o conocimiento que se impone y enseña como una alternativa única.
La codificación se realizó por dos jueces siguiendo tres pasos microanalíticos: (a) identificación de ‘voces discursivas’ correspondientes a enunciadores recurrentes en el habla de paciente y terapeuta; (b) categorización de voces discursivas de cada paciente y terapeuta como posiciones discursivas idiosincráticas; y (c) clasificación de las posiciones discursivas idiosincráticas de acuerdo al MPD.
La confiabilidad inter-jueces fue evaluada considerando el total de episodios (n = 153, 6,575 segmentos) obteniéndose un k = .762, p < .05 (Cohen, 1968).
Codificación de Patrones de Cualidad Vocal (PCV)
Dos codificadores entrenados aplicaron el sistema de codificación de PCV (Tomicic et al., 2011), categorizando el habla de paciente y terapeuta en las siguientes categorías: (a) Reporte (imprime al habla la cualidad de distancia emocional, reportando un contenido sin compromiso afectivo); (b) Conectado (imprime al habla una cualidad elaborativa y de orientación hacia el interlocutor); (c) Afirmativo (imprime al habla la cualidad de certeza y convicción, de aleccionamiento y compromiso con lo dicho); (d) Reflexivo (imprime al habla la cualidad de introspección), y; (e) Emocional, (imprime al habla una cualidad emocional ya sea expresiva o contenida).
La codificación se realizó siguiendo los cuatro pasos señalados en el manual de PCV (Tomicic et al., 2009), ciñéndose al procedimiento estandarizado. El valor Kappa obtenido para el total de episodios (n = 153, 4,553 segmentos) fue k = .658, p < .05.
Codificación de Categorías de Expresión Facial (CEF)
Se utilizó el Sistema de Codificación de la Conducta Facial (FACS, Facial Action Coding System; Ekman & Friesen, 1978) que permite identificar 44 unidades de acción facial. Cada episodio fue dividido en segmentos de video de 25 cuadros por segundo. En cada cuadro se codificó la presencia y tipo de acción facial para paciente y terapeuta.
Las CEF fueron: (a) Emociones Básicas: positivas (alegría) y negativas (rabia, tristeza, miedo, asco y desprecio); y (b) Conductas Faciales Inespecíficas: mirada (contacto ocular con el interlocutor), adaptadores (contacto de una parte del cuerpo o del rostro con otra parte del rostro) y procesos de control (acciones inespecíficas centradas alrededor de la boca).
La codificación fue realizada por tres jueces entrenados. Se calculó la confiabilidad interjuez entre el juez 1 y los jueces 2 y 3 en el 25% de la muestra (N = 14). La confiabilidad para la mirada (k = .65, p < .01 para jueces 1 y 2 y k = .73, p < .01 para jueces 1 y 3) y adaptadores (k = .86, p < .01 para jueces 1 y 2 y k = .87, p < .01 para jueces 1 y 3) fue adecuada, mientras que en el caso de las emociones básicas fue insuficiente (valores entre k = .21 y k = .52).
Resultados
Posiciones discursivas, de pacientes y terapeutas en episodios de cambio y ruptura.
Patrones de cualidad vocal de pacientes y terapeutas en episodios de cambio y ruptura.
Presencia de conducta facial regulatoria en Episodios de Cambio y de Ruptura en pacientes y terapeutas.
Nota: aDiferencias en total de frames para Mirada, Control y Adaptadores se debe a secuencias de video no codificables.
Para la evaluación estadística de los modos de interacción verbal (PD) y no verbal (PCV y CEF) se utilizó un modelo que considerara el carácter anidado de los datos. Cada una de las variables fue dicotomizada. Por ejemplo cuando el paciente usa la PD Reflexiva, la variable adquiere el valor = 1 y cuando usa las PD Independiente y Dependiente adquiere el valor 0. Así, se compara la probabilidad de ocurrencia de cada PD dicotomizada según el tipo de episodio. Para ello se realizó un Logistic Hierarchical Regression Analysis (HLM 7.0), utilizando el método de estimación PLQ, con una distribución Bernoulli (nivel 1). Se estableció un modelo de tres niveles: Nivel-1 (turno de palabra); Nivel-2 (episodio), y el Nivel-3 (psicoterapia completa de cada paciente).
El procedimiento consideró (a) la estimación del modelo no-condicional, para determinar existencia de variabilidad a explicar de la variable dependiente; (b) la incorporación del (de los) predictor(es) del nivel-1, modelando la evolución de las variables a lo largo del episodio, es decir, en la secuencia numérica de ‘turnos de palabra’ que inicia en ‘Cero’ 1 y aumenta en una unidad cada vez que transcurre un turno; (c) la incorporación de aquellos predictores de nivel-1 significativos (Intercepto y/o pendiente asociada a la evolución dentro del episodio) como ‘efectos random’ en el nivel-2, para determinar variación según tipo de episodio. La variable Tipo de Episodio (ER = 0, EC = 1) fue modelada como predictor de nivel-2 en la medida que explicaba variabilidad. Adicionalmente, la variable Sesión, que da cuenta del momento de la psicoterapia en que acontecen los episodios (operacionalizada como número de sesión) fue incorporada como predictor sólo del intercepto (en caso de dar cuenta de variabilidad significativa). Finalmente, (d) A nivel-3, se incorporó la variable Nivel de Funcionamiento del Paciente, distinguiendo si éste se encontraba en la población funcional (1) o disfuncional (0) al inicio de la psicoterapia; ésta fue considerada como variable control del intercepto en el caso que explicara varianza en el modelo. Se modeló en primer lugar el intercepto (con los predictores de nivel 2 y 3 2 ) y posteriormente la pendiente asociada al transcurso de la terapia.
Similar procedimiento se utilizó con los PCV dicotomizados, incorporando como predictores del nivel-1, la variable que da cuenta de la evolución del episodio, y la variable Actor, que da cuenta de quién es el hablante (1 = Paciente, 0 = Terapeuta), y la interacción entre ambas variables. Las Conductas Inespecíficas Faciales fueron dicotomizadas (Presencia = 1, Ausencia = 0) en pacientes y terapeutas respectivamente. Las Emociones Básicas también fueron dicotomizadas, pero utilizando como universo de codificación solo aquellos marcos temporales (frames) en que se identificó su presencia. En estos modelos, el predictor ‘evolución a lo largo del episodio’ (nivel-1) fue operacionalizado como la secuencia temporal de frames (segmentos de 25 segundos), asumiendo el valor cero en el frame inicial, y aumentando en un punto en la medida que transcurría cada frame durante el episodio.
Parámetros de los Modelos (HLM): Discurso, voz y expresión facial según tipo de episodio.
Notas: a Nivel-1 N = 1,917 (Pacientes) & N = 1,795 (Terapeutas), Nivel-2 N = 196, Nivel-3 N = 5. b Nivel-1 N = 2632 (Pacientes & Terapeutas), Nivel-2 N = 132, Nivel-3 N = 5; c Nivel-1 N = 6974 (Terapeutas) & N = 7,454 (Pacientes), Nivel-2 N = 54, Nivel-3 N = 5. Tipo de Episodio: 0 = Episodio de Ruptura vs. 1 = Episodio de Cambio. Nivel de funcionamiento del Paciente = Población funcional (1) o disfuncional (0). Actor: 1 = Paciente, 0 = Terapeuta. N/C = No corresponde. dSe presentan los coeficientes Gama (γ) y sus errores (ES) entre paréntesis en los efectos fijos; abajo se presenta el Odds Ratio su el Intervalo de confianza (95% IC). eVariables centradas respecto del Gran Promedio. fModelo estimado Logit(y) = G000 + G010*Sesión+ G020*Tipo de Episodio + G100* Evolución (durante episodios) + G110*Tipo de Epsidio * Evolución + r0 + r1 (Evolución durante episodio)+ u00. gModelo estimado Logit(y) = G000 + G010*Tipo de Episodio + G100*Actor + r0 + u00. hModelo estimado Logit(y) = G000 + G100*Actor + G200* Evolución (durante los episodios) + G300* Evolución (durante los episodios)* Actor + r0 + u00. iPCV Emocional considera Emocional Expresivo (73%) y Emocional Contenido (27%). jModelo estimado Logit(y) = G000 + G010*Tipo de Episodio + G100* Evolución (durante episodios) + r0 + r1 (Evolución durante episodio)+ u°°. kModelo estimado Logit(y) = G000 + G010*Tipo de Episodio + G100* Evolución (durante episodios) + G110 Tipo de Episodio * Evolución (durante episodios) r0 + r1 (Evolución durante episodio)+ u00. *p < .05; **p < .01; ***p < .001.
Note 1: Carolina Altimir is not part of this article. Please exclude her from both the Spanish and English versión.
Note 2: Javier Morán is the first autor, and Claudio Martínez is the correspondence autor:
Claudio Martínez, Universidad Diego Portales. E-mail: claudio.martinez@mail.udp.cl
Posiciones discursivas
Al inicio de los EC es mayor la probabilidad la PD Reflexiva del paciente, aumentando esta en la medida que transcurre el episodio. Tal como lo muestra la Figura 1 (cuadrante a), en el ‘momento de cambio’ (que acontece al final del episodio) el paciente presenta la mayor probabilidad de interactuar desde esta posición, contrastando con lo que acontece en los ER.
Probabilidad de ocurrencia de Posiciones Discursivas y Categorías de Expresión Facial a lo largo de los episodios.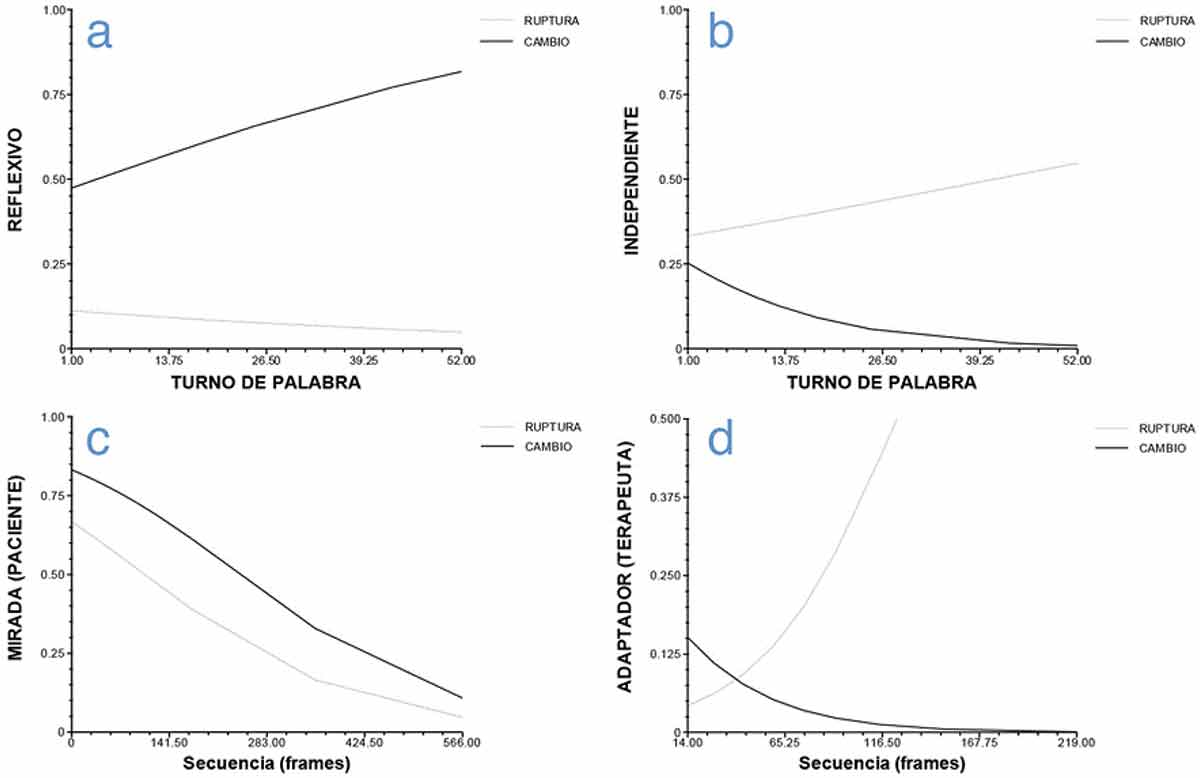
En el caso de la PD Independiente, si bien la probabilidad de que el paciente interactúe desde esta PD es similar en el inicio de ambos tipos de episodios, su probabilidad aumenta en la medida que transcurre el ER y disminuye en el transcurso del EC (Figura 1, cuadrante b).
No se observaron diferencias en la probabilidad de que el paciente interactúe desde la PD Dependiente y la probabilidad que el terapeuta lo haga desde las PDs Propositivo y Profesor según el tipo de episodio.
Patrones de cualidad vocal
Los resultados indican que sólo el PCV Reporte varía en función del tipo de episodio una vez que se controlan la variabilidad asociada al emisor del lenguaje. Así, se observa una mayor probabilidad de ocurrencia del PCV Reporte en ER en comparación con los EC (OR 0.65, 95%IC 0.43–0.98). Además, tanto en los EC como en los ER se aprecia que en la medida que el episodio transcurre aumenta la probabilidad de uso del PCV Emocional por parte del paciente, mientras que la probabilidad de uso del mismo PCV por parte del terapeuta se mantiene baja durante todo el episodio.
Conductas Inespecíficas Faciales y Emociones Básicas
La probabilidad de mirada en pacientes y de adaptadores en terapeutas depende del tipo de episodio. Es más probable que el paciente dirija su mirada al terapeuta en EC. Sin embargo esta probabilidad disminuye en el transcurso de ambos tipos de episodios (Figura 1, cuadrante c). Por su parte, la probabilidad de adaptadores en el terapeuta disminuye a lo largo del EC y, en contraste, aumenta en el transcurso del ER (Figura 1, cuadrante d).
Discusión
Esta investigación permitió describir las características discursivas, vocales y de expresión facial que dan cuenta de las manifestaciones verbal y no verbal de la regulación entre paciente y terapeuta en dos escenarios interaccionales relevantes para el proceso psicoterapéutico. Los resultados muestran que la utilización de técnicas microanalíticas como el Modelo de Posicionamiento Subjetivo, los Patrones de Cualidad Vocal o las Categorías de Expresión Facial permiten discriminar y diferenciar aspectos relevantes de la interacción terapéutica para comprender los fenómenos regulatorios que la conforman, desde un acercamiento multidimensional. Particularmente, los escenarios interaccionales de cambio y ruptura han permitido observar estos fenómenos regulatorios, destacando las diferentes funciones que el discurso, la cualidad vocal y el gesto facial cumplen en dicho proceso.
Para el caso de los episodios de cambio, se observó que los pacientes, a medida que avanza el episodio y se acercan a una verbalización que manifiesta un cambio en la manera de entenderse a sí mismos y sus problemas, hablan menos desde la posición discursiva independiente, sugiriendo así un posicionamiento subjetivo de mayor apertura al diálogo. Lo anterior ocurre en conjunto con un habla articulada desde un discurso reflexivo (i.e., posición discursiva reflexiva), sugiriendo la emergencia de un fenómeno regulatorio entre posiciones discursivas, favoreciendo la adopción de una postura que escucha y evalúa críticamente su propio actuar (Martínez et al., 2014).
En el caso del terapeuta, no se observó predominio de una de sus dos posiciones discursivas. Al respecto, es posible hipotetizar que su habla se halla organizada desde su rol y, adecuándose momento a momento a la oferta relacional del paciente, con independencia de si el escenario interaccional es un episodio de cambio o de ruptura (véase Tomicic, Martinez, & Krause, 2014).
Lo anterior coincide con lo señalado por Stiles, Hill, & Elliott (2015) quienes proponen que el terapeuta tiende a asumir un rol responsivo, orientado a ajustarse a las necesidades del paciente.
La expresión vocal característica de los pacientes durante los episodios de cambio fue la cualidad emocional, en cambio, en los terapeutas este patrón vocal fue constantemente menor durante este tipo de episodio. Este resultado es coincidente con hallazgos que muestran las diferencias expresivas implícitas de los roles diferenciados de paciente y terapeuta (Tomicic et al., 2014). Considerando que el cambio correspondería a un momento del proceso terapéutico que impactaría profundamente las teorías subjetivas del paciente (Krause, 2005), es posible que la sonoridad emocional en el habla de éstos podría evidenciar un intento por autorregular afectos asociados a la intensidad afectiva característica de este tipo de episodios. Consecuentemente, podría ser hipotetizado que los terapeutas prácticamente no hablan con este patrón de cualidad vocal debido a que ofrecen soporte, en términos de mantener un habla que, en este nivel, no se acopla o contagia con el del paciente.
Respecto a la expresión facial, los pacientes tendieron a mirar más a los terapeutas durante este tipo de episodios, pero a medida que se acercaron al momento de cambio este comportamiento disminuyó. Si bien la mirada posee distintas funciones comunicativas y regulatorias durante la interacción terapéutica (Merten, 1997), puede asumirse que en el contexto de un episodio de cambio, en el que se evidencia un proceso de transformación de significados y por tanto una experiencia de carácter afectivamente positiva, la mirada cumple funciones de regulación complementarias (Bänninger-Huber & Widmer, 1999). Así, dirigir inicialmente la mirada hacia el terapeuta, puede tener una función de indicar que el afecto expresado está dirigido al compañero de interacción o bien a la interacción misma, que está comenzando a gestar una transformación de significados. En otras palabras, el paciente se muestra afectivamente involucrado en una interacción que está ‘produciendo’ algo. Por su parte, la progresiva retirada de la mirada a medida que se avanza hacia el momento de cambio, puede indicar un giro del involucramiento afectivo y de la dirección del afecto hacia el contenido de la narración verbal (i.e., el contenido del cambio) y hacia sí mismo, es decir, hacia el depositario de la transformación de significados.
En los terapeutas se observó que a medida que transcurre el episodio de cambio disminuye el uso de adaptadores, indicando una menor tensión emocional (With & Kaiser, 2009). Si bien se requiere más evidencia para interpretar precisamente este hallazgo como un fenómeno regulatorio, es posible que cumpla un papel positivo en relación al cambio, en la medida que favorecería que el paciente perciba al terapeuta asumiendo un rol más receptivo y emocionalmente disponible.
Durante los episodios de ruptura los pacientes tendieron a interactuar desde la posición discursiva independiente, asociada a un posicionamiento subjetivo de autosuficiencia y de rechazo de la ayuda de otros, lo que daría cuenta no sólo del distanciamiento relacional en momentos de impasse terapéutico, sino que, tal como describen Allen y Fonagy (2006), podría evidenciar una estrategia regulatoria del paciente ante el reconocimiento de una experiencia de desencuentro o distancia con el otro. En el caso del terapeuta, al igual que en episodios de cambio, no se observó un uso predominante de alguna posición discursiva, reforzando así la hipótesis en la línea del ejercicio de su rol.
Igualmente que en los episodios de cambio, en episodios de ruptura los pacientes hablaron más frecuentemente con el patrón emocional de cualidad vocal. Sin embargo, en este escenario interaccional, paciente y terapeuta se expresaron más frecuentemente con el patrón de cualidad vocal reporte. El uso por parte del paciente de estos dos patrones contrapuestos de cualidad vocal, uno desafectado y otro emocionalmente cargado, podría asociarse a un intento por autorregular los afectos negativos propios de un escenario de ruptura de la alianza terapéutica (Tomicic et al., 2014). Aunque esta hipótesis requiere de mayor evidencia, es coherente con la sonoridad de la voz del terapeuta, de manera que una cualidad vocal desafectada cumpliría una función reguladora orientada a afrontar los efectos del quiebre en la relación.
Consistente con lo descrito hasta ahora, a nivel de expresión facial también se observan esfuerzos de autorregulación y regulación mutua desplegados por pacientes y terapeutas en este tipo de episodios. Los primeros disminuyen el contacto visual y los segundos aumentan el uso de adaptadores, sugiriendo que ambos se hallan realizando acciones que contribuyen a expresar, gestionar o aliviar la tensión.
No obstante su relevancia, los resultados de este estudio corresponden a una muestra de episodios anidados en un número pequeño de psicoterapias que, a su vez, son heterogéneas con respecto a su enfoque, duración y diagnóstico de sus pacientes. Por tanto, quedan pendientes para futuras investigaciones preguntas relativas a las maneras en que la extensión de las terapias, o la severidad y cronicidad de las afecciones de los pacientes, puedan determinar variaciones en los procesos regulatorios entre estos y sus terapeutas, como también en las manifestaciones verbales y no verbales de dichos procesos.
Footnotes
This research study was carried out within the Fondecyt Project, Nos. 1110361 and 1150639, Postdoctoral Fondecyt Project N° 3150029, and has been partially funded by the Ministry of Economy, Development and the Tourism Innovation Fund for Competitiveness (FIC), through the Millennium Science Initiative Project IS130005. / Esta investigación se ha realizado dentro del proyecto Fondecyt N°s 1110361 y 1150639, y recibió apoyo del Fondo de Innovación para la Competitividad (FIC) del Ministerio de Economía, Fomento y Turismo, a través de la Iniciativa Científica Milenio, Proyecto IS130005.
Disclosure statement
No potential conflict of interest was reported by the authors. / Los autores no han referido ningún potencial conflicto de interés en relación con este artículo.
1.
This allows the intercept to account for the probability of occurrence of the DP at the start of episodes.
2.
Predictors of level 1, 2 and 3 that did not account for significant variability in the models were removed.
1.
Esto permite que el intercepto dé cuenta de la probabilidad de ocurrencia de la PD al inicio de los episodios.
2.
Predictores de nivel 1, 2 y 3 que no daban cuenta de variabilidad significativa en los modelos fueron eliminados de éstos.