
Abstract
The therapeutic relationship is organized triadically between children, therapists and parents, yet little research focuses on its evolution as a change mechanism integrating these perspectives. Develop a comprehensive model of the therapeutic relationship as a change mechanism in different phases of psychotherapy, from the perspective of children, parents and therapists. A grounded theory analysis integrated findings from a retrospective and a qualitative longitudinal study of the therapeutic relationship with children and parents as change factors based on semi-structured interviews and children’s drawings. Initially, therapists’ close, flexible attitude improved children’s and parents’ motivation for psychotherapy. Later, a child-centred, playful relationship fostered children’s affection and trust in the therapists, promoting emotional and socio-affective changes. Lastly, as a greater bond developed, children internalized the therapist as a significant figure, and deeper changes emerged. Parents’ changes were eased by further trust and collaboration in the relationship with the therapist, and changes in the child-parent relationship emerged. Constructing positive therapeutic relationships requires participants’ evolving dispositions. These relationships shape progressive changes in children and their parents.
Although child psychotherapy research has made critical progress in recent years (Schmidt & Schimmelmann, 2015), it still represents a rather new field. Childhood is an intense developmental period characterized by constant change, and this — together with the involvement of parents — means that it is quite different from therapy with adults (Midgley et al., 2018). Therefore, child psychotherapy requires its own body of evidence regarding the psychotherapy process (Target, 2018).
In child psychotherapy, the therapeutic relationship has been conceived as central for therapeutic change (Shirk & Karver, 2011). This relationship can be broadly defined as the feelings and attitudes that therapists and patients experience for each other and the way they are expressed (Gelso & Carter, 1994). This definition includes the working alliance, the real relationship and transferential and countertransferential components (Gelso, 2019). Scarce research has focused on child therapy relationships (Shirk & Karver, 2011), and when done the tendency has been to use instruments based on Bordin’s (1979) therapeutic alliance model (Shirk & Karver, 2011). This model was conceived for adults’ psychotherapy and emphasizes the patients’ collaborative role (Horvath, 1994). Collaboration in child psychotherapy may express in a different way, primarily because children rarely refer themselves to treatment (Halfon, 2021) and may be less motivated to engage in an activity that was not initiated by themselves (Shirk & Karver, 2011). Nevertheless, a positive alliance is associated with positive outcomes, symptom reduction in children and greater motivation to address their problems (Hawley & Weisz, 2005; Karver et al., 2018; Liber et al., 2010; Shirk & Karver, 2011).
It is important to note that the child-parent-therapist connection operates as a triadic relationship (Gvion & Bar, 2014). Yet, few studies have addressed jointly these relationships and their mutual effect on change processes. The quality of the parent-therapist relationship is associated with parents’ commitment to treatment (Hawley & Weisz, 2005) and session support, affecting the treatment outcome (Kazdin et al., 2006; Marker et al., 2013). Positive parental alliance relates to better parenting skills and improved family interactions; when combined with a firm commitment to therapy, it supports the quality of the alliance with the child (Kazdin et al., 2006).
The therapeutic relationship may express differently according to the length of the process (Gelso, 2019). From the perspective of patients and therapists, the therapeutic relationship builds first as a technical dimension, which provides a stable structure for the helping relationship. Within this structure an affective dimension grows, characterized by the genuine feelings between patient and therapist that foster the building of trust in the therapist, a key element for a successful process. This second dimension strengthens and gains prominence as the therapy advances (Altimir et al., 2017).
The development of child psychotherapy research that incorporates the perspectives of children, parents and therapists is recent (Alamo, 2019; Núñez et al., 2021). Particularly children have been left out, with the false belief that they are unable to give valid comments about their experiences (Gibson & Cartwright, 2014). When consulted, children generally have a positive appreciation of their therapy (Carroll, 2002), but some may not recall why they participated in it (Areas et al., 2020; Carroll, 2002). Children identify changes due to psychotherapy, describing an improvement in different areas, such as their emotional well-being and interpersonal relationships, among others (Alamo, 2019; Areas et al., 2020; Capella et al., 2018, 2015; Carlberg et al., 2009; Núñez et al., 2022). They also note a more caring and less hostile attitude in their mothers towards them (Capella et al., 2018). Parents recall they further understand the child’s problems, achieving a better management of their child’s difficulties (Alamo, 2019; Núñez et al., 2022).
Children underscore the therapeutic relationship as a central aspect of their psychotherapy. They report a positive appreciation of their therapists and view them as someone who can help them, highlighting the trust and affection to their therapist, having fun and playing (Areas et al., 2020; Capella et al., 2018; Núñez et al., 2021). These interpersonal elements improve children’s and parents’ attitudes towards therapy (Alamo, 2019; Areas et al., 2020; Capella et al., 2018; Núñez et al., 2022).
However, the evolution of our understanding of the therapeutic relationship in child psychotherapy to a triadic view, and its contributions as a change mechanism through the therapeutic process, has only rarely been explored from the combined perspectives of children, parents and therapists. The central question in this paper is how the therapeutic relationship with children and parents evolves as a change mechanism in child psychotherapy, from the perspectives of children, parents and therapists.
Methods
Design
This qualitative study entailed three phases: (1) a retrospective study of the therapeutic relationship in child therapy to identify the core elements highlighted by children, parents and therapists; (2) a longitudinal study focused on the therapeutic relationship as a change factor in the beginning and middle phases of psychotherapy according to children, parents and therapists; and (3) the integration of the key findings of phases 1 and 2 to create a comprehensive model of the evolution of the therapeutic relationship as a change mechanism in different moments of child psychotherapy.
The core findings of phases 1 and 2 were already published (Núñez et al., 2022, 2021), so the focus of the present paper is phase 3.
Participants
Participants’ characteristics.
The sampling strategy for both phases was purposive (Flick, 2018) and intended the maximum variation regarding children’s sex and age, consulting reason and therapists’ theoretical framework. Participating children were referred to a mental health service for different reasons. Therapists entailed varied levels of experience but were relatively inexperienced in phase two. Therapies involved directive and nondirective play, art and narrative techniques in individual and family sessions. In phase, 1 all therapies terminated with an agreed ending except for one dropout and were defined as long term when continued for over six months. In phase 2, therapies were open-ended and on-going processes.
Procedure
Ethical approval was granted from the Scientific Ethics Committee in Social Sciences, Arts and Humanities of the Pontificia Universidad Católica de Chile, and collaboration agreements were established with mental health centres of public, private and university settings in Santiago, Chile.
In phase 1, participants were contacted at the beginning of psychotherapy; the informed consent of parents and therapists and assent of children were completed. Once the psychotherapy concluded, the research team conducted interviews, complemented with children’s drawings.
In phase 2, the same recruitment procedure used in phase one was developed; however, participants were interviewed after the first or second individual session of psychotherapy with the children and after four months of intervention (M = 16.4 sessions).
In phase 3, results from phases 1 and 2 were merged in a comprehensive model of the different moments of therapy: the beginning (1 or 2 sessions), the middle-advanced (by four months) and the final phase of psychotherapy (when ended).
Data collection
Semi-structured interviews
Semi-structured individual interviews with participants comprised 66 units of analysis. Interview schedules were developed by the research team and started with an open question regarding the psychotherapy experience; the therapeutic expectations, relationship, change processes and contents were addressed next. Interviews were transcribed following the Mergenthaler Norms (Mergenthaler & Gril, 1996).
Drawings
To complement verbal expression, children were asked for two specific drawings during the interviews. The first was ‘My psychologist and me’ (Núñez et al., 2021) and addressed the experience of the therapeutic relationship. The second focused on expected or perceived change and varied depending on the moment of the interview. Children were asked to draw ‘How am I before/after therapy’ (Capella et al., 2015) in the follow-up interview, ‘How am I at the beginning of therapy/How I want to be at the end of therapy’ (Núñez et al., 2022) in the initial moment and ‘How was I before therapy/How am I now’ (Capella et al., 2018) after four months of psychotherapy. In these second drawings, the paper had a vertical line in the middle, creating side-by-side sketches. Researchers followed children’s spontaneous expressions and asked open questions to promote their narratives. These verbalizations formed part of the interview transcript.
Data analysis
Data were analysed through open, axial and selective coding processes of grounded theory methods (Corbin & Strauss, 2008). In phases 1 and 2, first, interviews followed open coding by identifying and then contrasting categories. Children’s, parents’ and therapists’ perspectives were treated separately in open coding, supported by ATLAS.TI v8 software. Drawings were analysed as part of the interview transcript with children and through qualitative analysis guidelines for therapeutic drawings (Alamo, 2019; Núñez et al., 2021). Then axial coding was developed and focused on mapping the relationships among concepts and categories in an explanatory scheme. Open and axial results were reported in two papers (Núñez et al., 2022, 2021), where vignettes and drawings supported the findings.
In phase 3, selective coding was developed (Corbin & Strauss, 2008), following the prior axial coding of phases 1 and 2. Findings from the different time points were described and compared, involving a procedural analysis (Corbin & Strauss, 2008). A higher level of abstraction and relations within categories was developed (Flick, 2018), to propose a comprehensive model through an integrative diagram and its explanation. In all phases, agreement was pursued though an intersubjective triangulation strategy; several views were considered to reduce researcher bias (Altimir et al., 2017).
Results
The integration of findings of phases 1 and 2 enabled the formulation of a comprehensive model of the evolution of the therapeutic relationship as a change mechanism. This model identifies the change factors that stem from the children’s, therapists’ and parents’ attitudes and roles in different phases of psychotherapy and from the evolution of the child-therapist and parent-therapist relationship (Figure 1). In this way, interrelated levels of changes are described: roles and attitudes interconnect and shape the therapeutic relationship, and this relationship favours changes in children and parents.
Evolution of the therapeutic relationship as a change mechanism in child psychotherapy.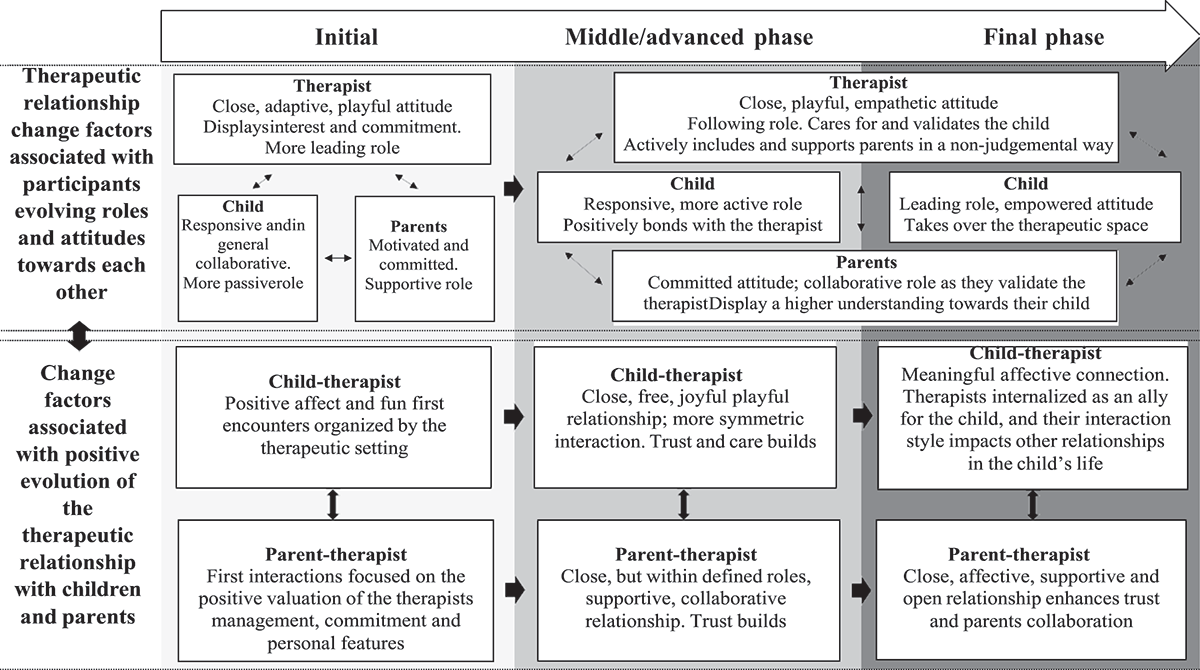
Evolution of the attitudes and roles between child psychotherapy participants
The attitudes and roles of children, therapists and parents changed through psychotherapy. In the beginning, the therapists displayed a central lead in generating a positive encounter with the child. The therapist’s initial role was crucial; their genuine interest, affectionate and kind attitude towards children and parents constituted therapist-offered conditions for psychotherapy to advance.
The child’s collaborative attitude was also essential for the development of the therapeutic relationship. However, at the beginning of psychotherapy, children presented a more passive role, sometimes with a rejecting attitude when they had negative expectations towards the therapist or the utility of psychotherapy. As the therapist’s initial attitude was positively experienced by children in a responsive manner, their motivation and attitude towards the therapist and psychotherapy improved.
As parents pursued psychotherapy for their children, they generally had a supportive role: they explained the importance of psychotherapy and encouraged their child to participate. However, some parents presented a degree of initial scepticism towards the therapist’s capacity to help, especially when therapists were very young. This initial distrust was overcome by the therapists’ high commitment and their capacity to make meaningful and accurate interventions with the parents. Parents contributed to this change through a positive disposition. Once this reticence was overcome, parents reported a better valuation of the therapist and higher compliance towards the interventions.
In a more advanced phase of psychotherapy, therapists generally stepped back in their leading role and followed the child’s needs and contents. Therapists’ friendly, playful and nice attitude and high level of commitment and availability were valued by children and parents and were not role-expected. The high commitment of therapists was appreciated by children and parents beyond their young age. The counterpart experience of young therapists was a tendency to self-criticize their high involvement as they feared it may be unprofessional or non-therapeutic.
In response to the therapists’ relational offer, children mostly displayed a more participatory role and a caring attitude towards the therapist. This positive attitude was considered by parents and therapists to be a change factor for building a stronger therapeutic relationship. In parallel, the therapist generally promoted the participation of parents in their child’s process and supported parents in improving their relationship with the child. Parents highly valued the therapist’s committed, supportive, receptive and non-judgemental attitude, plus the therapist’s professional ability to provide helpful orientations.
In more long-term processes, the elements displayed in the middle phase advanced further. Children took over the leading role and showed a more empowered attitude towards their therapist. More positive traits in the child were underscored within the child-therapist relationship. The focus on the child’s positive relational offer was very important for children to experience a positive version of themselves, aiding an improved self-concept.
As parents evidenced positive changes in their child and the relationship with them, and felt supported by the therapist, their commitment towards the process grew, as well as their responsive and collaborative attitude.
Change factors associated with the positive evolution of the therapeutic relationship with children and parents in different moments of psychotherapy
Therapists were expected by parents to generate a positive emotional interaction with children, to help develop their willingness to participate in psychotherapy. However, to succeed in this path required a high amount of flexibility and focus from the therapist on the child’s interests. When achieved, a positive child-therapist relationship was experienced, giving place to a collaborative, role-related relationship.
Additionally, the first comfortable, free and playful encounters with the therapist generated immediate changes in children, as they felt more animated and less troubled. These changes positioned the child-therapist relationship as therapeutic, as it alleviated the child’s initial unease. In parallel, parents appreciated the therapist’s ability to manage and connect with the child, their dedication and guidance, improving their confidence towards the child psychotherapist and the validation of the therapist’s interventions.
As the therapeutic relationship evolved, affection grew between child and therapist. The therapeutic relationship configuration moved towards a more symmetric encounter in terms of affection. In this configurational change, play and playful joint activities engaging both the child and the therapist represented the core of the therapeutic relationship. The joint involvement in play promoted positive interpersonal feelings in children and therapists and empowered children through a child-centred encounter.
As the affective connection between child and therapist grew, trust emerged. Trust was not present at the beginning of the relationship and was considered essential for therapeutic change. Children came to like their therapists and felt good and comfortable with them. Once this happened, they shared more conflicted personal contents in psychotherapy. Addressing these matters with the therapists was considered a significant change factor. Children also felt important to their therapist. Children’s self-concepts became more positive and less burdened by difficulties than before psychotherapy, and for children and parents, these changes were eased by the therapist’s help and genuine care.
The parent-therapist relationship evolved in terms of trust and validation of the therapists, but within defined roles. Parents viewed psychotherapy as teamwork between the therapist, the child and themselves. A positive parent-therapist relationship promoted the receptivity of parents to the therapist’s interventions and enabled changes in their parental role, as they expanded their understanding of their child’s problems and how to deal with them. This made parents feel calmer and more reassured in their parenting skills. An expanded comprehension in parents of their child’s problem improved the parent-child relationship.
A more meaningful therapeutic relationship with the child developed in longer-term psychotherapies. Therapists were remembered and named outside psychotherapy by children; they were described as allies when the child needed to get support in relation to their parents’ conduct. And when therapy ended, children wanted to be remembered by the therapist. These aspects reflected the internalization of the therapist in the child’s interpersonal repertory.
In longer-term therapies, a deeper level of involvement and openness in parents emerged, facilitated by the further development in the parents of trust and feeling supported by the therapist. Parents appreciated not being alone in their concern for their child’s well-being and felt helped by the therapist in some of their personal issues. Handling the parent’s personal issues strengthened the parent-therapist relationship through an improved attitude in parents.
Discussion
This study aimed to develop a comprehensive model of the child-therapist-parent relationship in the context of a range of child therapies. In this model, the importance of a leading initial role among therapists to generate an inviting environment is a key finding and has been previously described in psychotherapy with adults and children (Altimir et al., 2017).
However, in the studied therapies, the child’s responsive attitude and the support of parents was also required to shape their motivation and improve their feelings and attitude towards the therapist. Motivation is a core element for psychotherapy to work (Krause et al., 2011), but it may require extra support from parents and the therapist in the case of children.
In this study, collaboration was expressed in terms of ‘participation’, as described previously (Shirk & Karver, 2011), but also as ‘responsiveness’ in the child towards the therapist. This description expands the notion of therapeutic collaboration in children, as it is not always expressed in an active manner.
An initial passive or reticent attitude was described among several children. It is interesting to discuss that child psychotherapy may start from an early ‘rupture’ state of the relationship (Safran & Muran, 2006). Child psychotherapists’ first relational task may be to repair this onset ‘rupture’ in the child’s willingness to participate in psychotherapy.
It is important for child psychotherapists to keep in mind that psychotherapy itself is a challenging context for many children and parents. In this path, a therapist’s committed and supportive attitude towards parents was very important to move forward in their relationship. Similar findings have been reported in adult psychotherapy (Krause et al., 2011) and relate to a positive adult-adult interaction. This element has relevant clinical implications when working with parents in child psychotherapy. Parents may experience self-criticism of their parenting competence or feeling guilty for their child’s problems and can locate in a defensive position towards the therapist. A non-judgemental and empathetic stance in the child’s therapist towards parents seems key for them to start to trust and get involved in the therapeutic process. As parents expand their understanding and management of the child’s issues, as reported by Alamo (2019), a better disposition towards the child emerges and improves the parent-child relationship. These changes make parents feel reassured in their parenting skills.
As psychotherapy progresses, children and therapists fully engaged in play and activities representing the ‘affective-motor’ component of a positive therapeutic relationship. The relevance of joint play for children in psychotherapy has been reported previously (Areas et al., 2020; Capella et al., 2018), as it supports a meaningful therapeutic relationship (Núñez et al., 2021). As the child-therapist relationship grew in terms of an affective connection between them, trust emerged. The importance of trust-based therapeutic relationships for change in child psychotherapy has been underlined elsewhere (Areas et al., 2020; Capella et al., 2018), but the importance of both child and therapist genuinely having fun together has been less emphasized. This finding recalls Carlberg’s (1997) ‘turning points’ in child psychotherapy, as the emotional meeting between two mutually influencing subjects prepares the way for change to emerge.
In the later phase of longer-term treatments, it is interesting to discuss the therapist’s internalization in terms of mentalization, as children evoked their therapists in extra-therapeutic situations. This issue may suggest that the child is keeping the therapist’s ‘mind in mind’, and this favours the child to ponder difficult social interactions with others in a self-caring way, as they have been cared for by their therapists within a secure relationship.
This study shed light on the understanding of the therapeutic relationship in child psychotherapy. The different trajectories observed in the child-therapist and parent-therapist relationships should be further explored to advance our understanding of their dynamics, as well as the overall triadic relationship between child, parent and therapist.
A strength of this study was the multiple-perspective approach towards the therapeutic relationship, as it represents the triadic nature of this relationship. Moreover, the inclusion of children significantly enriched the findings, supporting the use of age-appropriate methods in psychotherapy research. However, a clear limitation of the developed model is that it was drawn only from positive therapeutic relationships and did not explore negative trajectories, despite that in child therapy there is a considerable number of less satisfactory therapy experiences. A second limitation is that many participating therapists were inexperienced ones. Future studies may use a larger and more diverse sample, especially with respect to the therapists.
La relación terapéutica como un mecanismo de cambio en la psicoterapia infantil: un estudio cualitativo de las perspectivas de niño/as, padres, y terapeutas en diferentes momentos del proceso
La investigación sobre psicoterapia infantil ha experimentado un progreso notable en los últimos años (Schmidt & Schimmelmann, 2015) sin embargo, todavía representa un campo relativamente nuevo. La infancia es un periodo de desarrollo intenso caracterizado por cambios constantes, y esto — junto con la implicación de los padres — significa que es bastante diferente de la terapia con adultos (Midgley et al., 2018). Por tanto, la psicoterapia infantil requiere de su propio conjunto de evidencia en relación con el proceso psicoterapéutico (Target, 2018).
En psicoterapia infantil, la relación terapéutica se ha concebido como un factor central para el cambio terapéutico (Shirk & Karver, 2011). Esta relación puede ser ampliamente definida como los sentimientos y actitudes que los terapeutas y los pacientes experimentan mutuamente, y la forma en que se expresan (Gelso & Carter, 1994). Esta definición incluye la alianza terapéutica, la relación real, y los componentes transferenciales y contratransferenciales (Gelso, 2019). Pocas investigaciones se han centrado en las relaciones de la terapia infantil (Shirk & Karver, 2011), y cuando lo han hecho la tendencia ha sido utilizar instrumentos basados en el modelo de alianza terapéutica de Bordin (1979; Shirk & Karver, 2011). Este modelo fue concebido para la psicoterapia de adultos y pone el énfasis en el rol colaborador de los pacientes (Horvath, 1994). La colaboración en la psicoterapia infantil se puede expresar de forma diferente, esencialmente porque los niño/as rara vez se auto refieren al tratamiento (Halfon, 2021) y pueden estar menos motivados a participar en una actividad que no ha sido iniciada por ellos mismos (Shirk & Karver, 2011). No obstante, una alianza positiva está asociada con resultados positivos, reducción de los síntomas de los niño/as, y una mayor motivación para abordar sus problemas (Hawley & Weisz, 2005; Karver et al., 2018; Liber et al., 2010; Shirk & Karver, 2011).
Es importante destacar que la conexión entre niño/a-padres-terapeuta funciona como una relación triádica (Gvion & Bar, 2014). Sin embargo, pocos estudios han abordado conjuntamente estas relaciones y su efecto mutuo sobre los procesos de cambio. La calidad de la relación padres-terapeuta está asociada con el compromiso de los padres con el tratamiento (Hawley & Weisz, 2005) y el apoyo a las sesiones, lo que afecta al resultado del tratamiento (Kazdin et al., 2006; Marker et al., 2013). Las alianzas parentales positivas se relacionan con mejores habilidades parentales e interacciones familiares; y cuando se combinan con un compromiso firme con la terapia, esto respalda la calidad de la alianza con el niño/a (Kazdin et al., 2006).
La relación terapéutica puede expresarse de manera diferente según la duración del proceso (Gelso, 2019). Desde la perspectiva de los pacientes y los terapeutas, la relación terapéutica se construye primero como una dimensión técnica que ofrece una estructura estable para la relación de ayuda. Dentro de esta estructura se desarrolla una dimensión afectiva, caracterizada por los sentimientos reales entre paciente y terapeuta, que fomenta el desarrollo de la confianza en el terapeuta, un elemento clave para el éxito del proceso. Esta segunda dimensión se fortalece y adquiere más importancia a medida que la terapia progresa (Altimir et al., 2017).
El desarrollo de las investigaciones sobre psicoterapia infantil que incorpora las perspectivas de los niño/as, los padres y los terapeutas es reciente (Alamo, 2019; Núñez et al., 2021). Particularmente, los niño/as han sido excluidos debido a la falsa creencia de que son incapaces de ofrecer comentarios válidos sobre sus experiencias (Gibson & Cartwright, 2014). Al ser consultados, los niño/as generalmente tienen una apreciación positiva de su terapia (Carroll, 2002), pero algunos pueden no recordar por qué la están haciendo (Areas et al., 2020; Carroll, 2002). Los niño/as identifican los cambios derivados de la psicoterapia, describiendo una mejoría en diferentes áreas, como pueden ser el bienestar emocional y las relaciones interpersonales, entre otras (Alamo, 2019; Areas et al., 2020; Capella et al., 2018, 2015; Carlberg et al., 2009; Núñez et al., 2022). También advierten que sus madres tienen actitudes más cariñosas y menos hostiles con ellos (Capella et al., 2018). Los padres manifiestan que comprenden más los problemas del niño/a, y consiguen gestionar mejor sus dificultades (Alamo, 2019; Núñez et al., 2022).
Los niño/as destacan la relación terapéutica como un aspecto central de su psicoterapia. Reportan una apreciación positiva de sus terapeutas, a quienes consideran como alguien que puede ayudarlos, subrayando la confianza y el afecto que sienten por su terapeuta, que lo pasan bien y juegan con él/ella (Areas et al., 2020; Capella et al., 2018; Núñez et al., 2021). Estos elementos interpersonales mejoran la actitud de los niño/as y los padres respecto de la terapia (Alamo, 2019; Areas et al., 2020; Capella et al., 2018; Núñez et al., 2022).
No obstante, la evolución de nuestra comprensión de la relación terapéutica en la psicoterapia infantil como una triada y de sus contribuciones como mecanismo de cambio a través del proceso terapéutico, ha sido raramente analizada desde las perspectivas combinadas de niño/as, padres, y terapeutas. La cuestión central en este artículo es de qué forma la relación terapéutica con los niño/as y los padres evoluciona como mecanismo de cambio en la psicoterapia infantil, desde las perspectivas de los niño/as, los padres, y los terapeutas.
Método
Diseño
Este estudio cualitativo implicó tres fases: (1) Un estudio retrospectivo de la relación terapéutica en la terapia infantil para identificar los elementos esenciales destacados por los niño/as, los padres y los terapeutas. (2) Un estudio longitudinal enfocado en la relación terapéutica como factor de cambio en las fases inicial y media de la psicoterapia de acuerdo con los niño/as, los padres y los terapeutas. (3) La integración de los hallazgos centrales en las fases 1 y 2, para crear un modelo exhaustivo de la evolución de la relación terapéutica como mecanismo de cambio en diferentes momentos de la psicoterapia infantil.
Los hallazgos esenciales de las fases 1 y 2 ya se han publicado (Núñez et al., 2022, 2021), de manera que el presente artículo se centra en la fase 3.
Participantes
Características de los participantes.
La estrategia para ambas fases fue un muestreo intencional (Flick, 2018) y se pretendió contar con la máxima variación en relación con el sexo y la edad de los niño/as, los motivos de consulta, y el marco teórico de los terapeutas. Los niño/as que participaron habían sido derivados a un servicio de salud mental por diferentes razones. Los terapeutas tenían diferentes niveles de experiencia, pero eran relativamente poco experimentados en la fase 2. Las terapias implicaron técnicas lúdicas, de arte y narrativas directivas y no directivas en sesiones individuales y familiares. En la fase 1 todas las terapias terminaron de común acuerdo entre los participantes, excepto un caso de deserción, y fueron definidas como terapias a largo plazo cuando se mantenían durante más de seis meses. En la fase 2 las terapias se encontraban en proceso y eran de extensión abierta.
Procedimiento
Se obtuvo la aprobación del Comité Científico de Ética en Ciencias Sociales, Artes y Humanidades de la Pontificia Universidad Católica de Chile, y se establecieron acuerdos de colaboración con centros de salud mental, públicos, privados y universitarios en Santiago, Chile.
En la fase 1 se contactó con los participantes al comienzo de la psicoterapia; se completó el consentimiento informado de padres y terapeutas, y el asentimiento de los niño/as. Una vez concluida la psicoterapia, el equipo de investigación realizó entrevistas complementadas con dibujos en el caso de los niño/as.
En la fase 2, se desarrolló el mismo procedimiento de reclutamiento utilizado en la fase 1; no obstante, se entrevistó a los participantes después de la primera o segunda sesión individual de psicoterapia con los niño/as, y luego de cuatro meses de intervención (sesiones M = 16.4).
En la fase 3, se combinaron los resultados de las fases 1 y 2 en un modelo comprensivo de los diferentes momentos de la terapia: la fase inicial (una o dos sesiones), la fase media-avanzada (a los cuatro meses), y la fase final de la psicoterapia (tras terminar).
Recolección de datos
Entrevistas semi-estructuradas
Las entrevistas individuales semi-estructuradas con los participantes comprendieron 66 unidades de análisis. El equipo de investigación creó los guiones de entrevista, que iniciaban con una pregunta abierta respecto de la experiencia psicoterapéutica; a continuación, se abordaron las expectativas, la relación, los procesos de cambio y los contenidos de la psicoterapia. Las entrevistas se transcribieron considerando las Normas de Mergenthaler (Mergenthaler & Gril, 1996).
Dibujos
Se solicitó a los niño/as que hicieran dos dibujos específicos durante las entrevistas para complementar la expresión verbal. El primer dibujo fue ‘Mi psicólogo y yo’ (Núñez et al., 2021) y se refería a la experiencia de la relación terapéutica. El segundo se centró en el cambio esperado o percibido, y varió dependiendo del momento de la entrevista. Se pidió a los niño/as que dibujaran ‘Cómo me siento antes/después de la terapia (Capella et al., 2015) en la entrevista de seguimiento; ‘Cómo me encuentro al comienzo de la terapia/Cómo quiero encontrarme al concluir la terapia’ (Núñez et al., 2022) en el momento inicial; y ‘Cómo me encontraba antes de la terapia/Cómo me encuentro ahora (Capella et al., 2018) después de cuatro meses de psicoterapia. En estos segundos dibujos, el papel tenía una línea vertical en el medio, creando bocetos uno al lado del otro. Los investigadores siguieron las expresiones espontáneas de los niño/as, y formularon preguntas abiertas para promover sus narrativas. Estas verbalizaciones formaron parte de la transcripción de la entrevista.
Análisis de datos
Los datos se analizaron a través de los procesos de codificación axial, abierta y selectiva de la teoría fundamentada (Corbin & Strauss, 2008). En las fases 1 y 2 en primer lugar las entrevistas siguieron una codificación abierta centrada en identificar y luego contrastar categorías. Las perspectivas de los niño/as, los padres y los terapeutas se trataron de forma separada en la codificación abierta, Este proceso fue desarrollado en el software ATLAS.TI v8. Los dibujos se analizaron como parte de la transcripción de la entrevista con los niño/as, y a través de directrices de análisis cualitativos para los dibujos terapéuticos (Alamo, 2019; Núñez et al., 2021). La codificación axial se desarrolló y enfocó en el mapeo de las relaciones entre conceptos y categorías en un esquema explicativo. Los resultados abiertos y axiales reportaron en de dos artículos previos (Núñez et al., 2022, 2021), en los cuales las viñetas y los dibujos apoyaban los hallazgos.
En la fase 3, se desarrolló una codificación selectiva (Corbin & Strauss, 2008), después de la codificación axial previa de las fases 1 y 2. Los hallazgos de los diferentes momentos se describieron y compararon, a partir de un análisis procedural (Corbin & Strauss, 2008). Se creó un nivel superior de abstracción y relaciones dentro de las categorías (Flick, 2018) para proponer un modelo comprensivo a través de un esquema integrativo y su explicación. En todas las fases se buscó un acuerdo a través de una estrategia de triangulación intersubjetiva; se consideraron varias perspectivas para reducir el sesgo del investigador (Altimir et al., 2017).
Resultados
La integración de los hallazgos de las fases 1 y 2 permitieron la formulación de un modelo comprensivo de la evolución de la relación terapéutica como mecanismo de cambio. Este modelo identifica los factores de cambio que surgen de las actitudes y roles de los niño/as, terapeutas, y padres en las diferentes fases de la psicoterapia, y de la evolución de la relación niño/a-terapeuta y padre/madre-terapeuta (Figura 1). Por tanto, se describen los niveles de cambios interrelacionados: los roles y las actitudes interconectan y modelan la relación terapéutica, y esta relación favorece los cambios en los niño/as y los padres.
Evolución de la relación terapéutica como mecanismo de cambio en la psicoterapia infantil.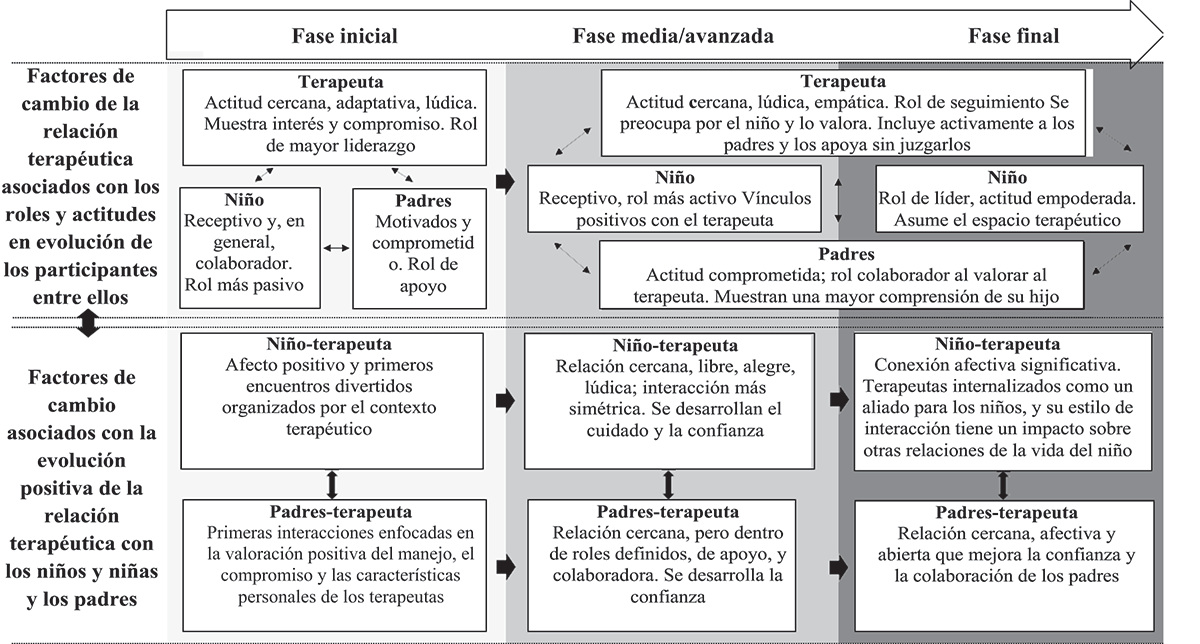
Evolución de las actitudes y roles entre los participantes de la psicoterapia infantil
Las actitudes y roles de los niño/as, terapeutas y padres cambiaron a lo largo de la psicoterapia. Al comienzo, los terapeutas asumieron un rol protagónico a la hora de generar un encuentro positivo con los niño/as. El rol inicial del terapeuta fue crucial; su genuino interés y su actitud afectuosa y amable con los niño/as y los padres constituyeron las condiciones ofrecidas por los terapeutas para el progreso de la psicoterapia.
La actitud colaboradora de los niño/as también fue esencial para el desarrollo de la relación terapéutica. No obstante, al comienzo de la psicoterapia, los niño/as manifestaron un rol más pasivo, en ocasiones con una actitud de rechazo cuando tenían expectativas negativas en relación con el terapeuta o la utilidad de la psicoterapia. El hecho de que los niño/as experimentaran positivamente la actitud inicial del terapeuta mostrándose receptivos, mejoró su motivación y su actitud respecto del terapeuta.
Por ser los padres quienes solicitaron la psicoterapia para sus hijos, en general tuvieron un rol de apoyo: explicaron a su hijo/a la importancia de la psicoterapia y lo motivaron para que participara en ella. Sin embargo, algunos padres presentaron un cierto grado inicial de escepticismo respecto de la capacidad del terapeuta para ayudarlos, especialmente si era muy joven. Esta desconfianza inicial fue superada gracias al gran compromiso del terapeuta, y a su capacidad para hacer intervenciones significativas y certeras con los padres. Los padres contribuyeron a este cambio a través de una disposición positiva. Una vez superada esta reticencia, los padres manifestaron una mejor valoración del terapeuta y una mayor conformidad con sus intervenciones.
En una fase más avanzada de la psicoterapia, los terapeutas generalmente abandonaron el rol más protagónico para seguir las necesidades y contenidos manifestados por los niño/as. La actitud cordial, amistosa y lúdica de los terapeutas, y el alto nivel de compromiso y disponibilidad fueron valorados por niño/as y padres, y no se esperaba de su rol. El gran compromiso de los terapeutas fue apreciado por niño/as y padres independientemente de su juventud. La experiencia equivalente de los terapeutas jóvenes fue una tendencia a la autocrítica por su gran implicación, debido al temor de que pudiera ser una actitud no profesional o no terapéutica.
En respuesta a la oferta relacional de los terapeutas, los niño/as mostraron mayoritariamente un rol participativo y una actitud afectiva hacia el terapeuta. Esta actitud positiva fue considerada por padres y terapeutas como un factor de cambio para construir una relación terapéutica más fuerte. Paralelamente, por lo general el terapeuta promovió la participación de los padres en el proceso de su hijo/a, y los apoyó a la hora de mejorar su relación con él/ella. Los padres valoraron muy positivamente la actitud comprometida, receptiva, de apoyo, y no crítica del terapeuta, además de su capacidad profesional para brindar una orientación útil.
En procesos de más largo plazo, los elementos presentados en la fase intermedia avanzaron aún más. Los niño/as asumieron el rol de liderazgo, y mostraron una actitud más empoderada hacia el terapeuta. Se destacaron los rasgos más positivos de los niño/as en la relación niño/a-terapeuta. El foco en la oferta relacional positiva del niño/a fue muy importante para que los niño/as experimentaran una versión positiva de sí mismos, lo que ayudó a que tuvieran un mejor concepto de sí mismos.
A medida que los padres observaron cambios positivos en su hijo/a y en la relación que mantenía con ellos, y se sintieron apoyados por el terapeuta, su compromiso con el proceso fue cada vez mayor, lo mismo que su actitud receptiva y colaboradora.
Factores de cambio asociados con la evolución positiva de la relación terapéutica con niño/as y padres en diferentes momentos de la psicoterapia
Los padres esperaban que los terapeutas generaran una interacción emocional positiva con los niño/as, para ayudar a desarrollar su disposición a participar en la psicoterapia. No obstante, tener éxito en este recorrido requería mucha flexibilidad por parte del terapeuta y que éste se centrara en los intereses del niño/a. Cuando esto se consiguió, se desarrolló una relación niño/a-terapeuta positiva, lo que dio lugar a una relación colaboradora de acuerdo con los roles.
Por otra parte, los primeros encuentros cómodos, libres y lúdicos con el terapeuta generaron cambios inmediatos en los niño/as, puesto que se sintieron más animados y menos preocupados. Estos cambios posicionaron la relación niño/a-terapeuta como una relación terapéutica en sí misma ya que aliviaba el malestar inicial del niño/a. Paralelamente, los padres apreciaron la capacidad del terapeuta para manejar. Paralelamente, los padres apreciaron la capacidad del terapeuta para manejar y conectar con su hijo/a, su dedicación, y orientación, y esto mejoró su confianza en el psicoterapeuta del niño/a, y la valoración de las intervenciones del terapeuta.
A medida que la relación terapéutica evolucionó, progresó el afecto entre el niño y el terapeuta. La configuración de la relación terapéutica tendió a un encuentro más simétrico en términos de afecto. En este cambio configuracional, el juego y las actividades lúdicas conjuntas en las que participaron tanto el niño/a como el terapeuta representaron el núcleo de la relación terapéutica. La participación conjunta en los juegos promovió sentimientos interpersonales positivos en los niño/as y terapeutas, y empoderó a los niño/as a través de un encuentro centrado en el niño/a.
A medida que la conexión afectiva entre el niño/a y el terapeuta fue progresando, emergió la confianza. La confianza no estuvo presente en el inicio de la relación, y se la consideró esencial para el cambio terapéutico. Los niño/as llegaron a sentir afecto por sus terapeutas y a encontrarse a gusto y cómodos en su presencia. En cuanto esto ocurrió, compartieron más contenidos personales conflictivos en la psicoterapia. El hecho de que hablaran de estos problemas con los terapeutas se consideró un factor de cambio significativo. Los niño/as también sintieron que eran importantes para su terapeuta. El auto-concepto de los niño/as fue entonces más positivo y menos cargado de dificultades que antes de la psicoterapia, y para los niño/as y los padres estos cambios fueron facilitados por la ayuda y el cuidado genuino del terapeuta.
La relación padres-terapeuta evolucionó en términos de confianza y valoración de los terapeutas, pero dentro de roles definidos. Los padres consideraron la psicoterapia como un trabajo en equipo entre el psicoterapeuta, el niño/a, y ellos mismos. Una relación padres-terapeuta positiva promovió la receptividad de los padres a las intervenciones del terapeuta y posibilitó cambios en su rol parental, a medida que comprendían más los problemas de su hijo/a, y la forma adecuada de gestionarlos. Esto provocó que los padres se sintieran más relajados y más seguros de sus habilidades parentales. Esa mayor comprensión de los padres del problema de su hijo/a mejoró la relación padres-niño/a.
Una relación terapéutica más significativa con el niño/a dio lugar a psicoterapias a más largo plazo. Los niño/as recordaron y nombraron a los terapeutas fuera de la psicoterapia; se los describió como aliados cuando el niño/a necesitó apoyo en relación con regular la conducta de sus padres. Y al concluir la terapia, los niño/as manifestaron su deseo de que el terapeuta los recordara. Estos aspectos reflejaron la internalización del terapeuta en el repertorio interpersonal del niño/a.
En terapias a más largo plazo, surgió un nivel más profundo de participación y apertura de los padres, facilitada por el posterior desarrollo de la confianza de los padres y su sensación de ser apoyados por el terapeuta. Los padres apreciaron no estar solos en su preocupación por el bienestar de sus hijos, y se sintieron ayudados por el psicoterapeuta en algunos de sus problemas personales. Abordar los problemas personales de los padres en las sesiones con éstos fortaleció la relación padres-terapeuta a través de una mejor actitud de los padres.
Discusión
El objetivo de este estudio fue desarrollar un modelo comprensivo de la relación niño/a-terapeuta-padres en el contexto de una variedad de psicoterapias infantiles. En este modelo, la importancia de un rol de liderazgo inicial en los terapeutas para generar un ambiente receptivo es un hallazgo clave, y ha sido descrita previamente en psicoterapia de adultos y niño/as (Altimir et al., 2017).
No obstante, en las terapias estudiadas la actitud receptiva del niño/a y el apoyo de los padres también fueron necesarios para moldear su motivación y mejorar sus sentimientos y actitudes hacia los terapeutas. La motivación es un elemento clave para que la psicoterapia sea efectiva (Krause et al., 2011), pero puede requerir un respaldo adicional de los padres y del terapeuta en el caso de los niño/as.
En este estudio la colaboración se expresó en términos de ‘participación’, tal como se ha descrito previamente (Shirk & Karver, 2011), pero también como la ‘receptividad’ del niño/a en relación con el terapeuta. Esta descripción amplía la idea de la colaboración terapéutica en los niño/as, ya que no siempre se expresa de manera activa.
En varios niño/as se observó una actitud inicial pasiva o reticente. Es interesante afirmar que la psicoterapia infantil puede iniciarse a partir de un estado de ‘ruptura’ temprana de la relación (Safran & Muran, 2006). La primera tarea relacional de los psicoterapeutas infantiles puede ser reparar esta ‘ruptura’ inicial en la disposición del niño/a a participar en la psicoterapia.
Es importante para los niño/as que los psicoterapeutas tengan en cuenta que la psicoterapia por sí misma es un contexto desafiante para muchos niño/as y padres. En este camino, la actitud comprometida y el apoyo del terapeuta a los padres fue muy importante para avanzar en su relación. Se han reportado hallazgos similares en psicoterapia de adultos (Krause et al., 2011) y se relacionan con una interacción positiva adulto-adulto. Este elemento tiene implicaciones clínicas relevantes cuando se trabaja con los padres en psicoterapia infantil. Los padres pueden criticar y cuestionar sus propias habilidades parentales, o sentirse culpables por los problemas de su hijo/a, y pueden asumir una postura defensiva frente al terapeuta. La actitud empática y no crítica del terapeuta hacia los padres parece esencial para que ellos comiencen a confiar en él y se involucren en el proceso terapéutico. A medida que los padres aumentan su comprensión y mejoran el manejo de los problemas de su hijo/a, tal como lo ha afirmado Alamo (2019), surge una mejor disposición en relación con el niño y mejora la relación padres-hijo. Estos cambios hacen que los padres se sientan tranquilos en lo que se refiere a sus habilidades parentales.
A medida que la psicoterapia progresa, el involucramiento pleno de los niños/as y los terapeutas en el juego y las actividades representan el ‘motor-afectivo’ de una relación terapéutica positiva. La importancia del juego conjunto para los niño/as en psicoterapia ha sido previamente abordada (Areas et al., 2020; Capella et al., 2018), ya que respalda una relación terapéutica significativa (Núñez et al., 2021). Cuando la relación niño/a-terapeuta progresó en términos de una conexión afectiva entre ellos, surgió la confianza. La importancia de las relaciones terapéuticas basadas en la confianza para que se produzcan cambios en la psicoterapia infantil ha sido subrayada en otros estudios (Areas et al., 2020; Capella et al., 2018), pero la importancia de que tanto el niño/a como el terapeuta disfruten realmente juntos ha sido menos enfatizada. Este hallazgo recuerda los ‘puntos de inflexión’ de Carlberg (1997) en psicoterapia infantil, porque el encuentro emocional entre dos sujetos que se influyen mutuamente allana el camino para que surja el cambio.
En la fase más avanzada de tratamientos a más largo plazo, es interesante comentar la internalización del terapeuta en términos de mentalización, ya que los niño/as recordaron a sus terapeutas en situaciones extra-terapéuticas. Ello puede sugerir que el niño/a sigue mantiene la ‘mente del terapeuta en mente’, y esto favorece que el niño/a reflexione sobre las interacciones sociales difíciles que mantiene con otras personas cuidando de sí mismo, tal como ha sido cuidado por su terapeuta en una relación segura.
Este estudio arrojó luz sobre la comprensión de la relación terapéutica en la psicoterapia infantil. Las diferentes trayectorias observadas en la relación niño/a-terapeuta y padres-terapeuta deberían analizarse más en profundidad para avanzar en la comprensión de su dinámica, así como también de la relación tríadica entre el niño/a, los padres y el terapeuta.
Un punto fuerte de este estudio fue el abordaje de la relación terapéutica desde múltiples perspectivas, ya que representa la naturaleza tríadica de esta relación. Más aún, la inclusión de los niño/as enriqueció significativamente los hallazgos, apoyando el uso de métodos evolutivamente sensibles a la edad en las investigaciones sobre la psicoterapia. No obstante, una clara limitación del modelo desarrollado es que se basa únicamente en relaciones terapéuticas positivas y no se analizaron trayectorias negativas; a pesar de que en terapia infantil hay un considerable número de experiencias terapéuticas menos satisfactorias. Una segunda limitación es que muchos de los terapeutas que participaron en el estudio no eran experimentados. Estudios futuros podrían utilizar una muestra más amplia y diversa, especialmente con respecto a los terapeutas.
Footnotes
This work was funded by the National Agency for Research and Development (ANID) / Scholarship Program / DOCTORADO NACIONAL /2016 – 21160244, and the Millennium Institute for Research on Depression and Personality-MIDAP ICS13_005. The authors thank the Center for Applied Psychology of the Faculty of Social Sciences of the University of Chile (CAPs) and the Mental Health Unit, San Joaquín Medical Center of the UC CHRISTUS Health Network, and the children, parents and therapists who participated. / Este trabajo fue financiado por la Agencia Nacional para la Investigación y el Desarrollo (National Agency for Research and Development, ANID)/Programa de Becas/DOCTORADO NACIONAL /2016 – 21160244, y el Instituto Millenium para la Investigación en Depresión y Personalidad-MIDAP ICS13_005. Los autores agradecen al Centro para la Psicología Aplicada de la Facultad de Ciencias Sociales de la Universidad de Chile (CAPs) y la Unidad de Salud Mental, Centro Médico San Joaquín de la Red de Salud UC CHRISTUS, y a los niños/las niñas, los padres, y los terapeutas que participaron en los estudios.
No potential conflict of interest was reported by the authors. / Los autores no han referido ningún potencial conflicto de interés en relación con este artículo.