
Abstract
The goal of the present study was to measure COVID-19 social representation and to characterize attitudes and knowledge about the virus SARS-CoV-2. With an exploratory nature, it used a non-probabilistic sample of 297 Portuguese adults. To measure COVID-19 social representation, we used a free evocation task; attitudes were assessed by 20-item questionnaires divided into cognitive, affective and behavioural dimensions; knowledge was assessed by a true or false test based upon general information made available by DGS [Portuguese health general directorate]. Results suggest participants have little belief that they could be infected, have the disease or even be preoccupied about it. Concerning social representation, results suggest the existence of two different groups of participants, one with a more favourable attitude towards COVID-19 and another with a less favourable attitude. The study raises questions to be developed in future research.
The novel coronavirus (2019-nCoV) or SARS-CoV-2 is a new, widely spreading virus, which causes COVID-19 or coronavirus disease. The COVID-19 pandemic beginning in 2020 has changed individual, social and socio-economic life at a global level. An infectious disease presents a real risk to humanity that implies adjustments at the individual and group levels, even in the face of a vaccine, as we are starting to see.
To deal with a new phenomenon such as the COVID-19 pandemic, social representations arise spontaneously to cope with and organize this novel, unpredictable, changing reality (Colì et al., 2020). Therefore, social representations can be conceived as forms of collective symbolic coping (Páez & Pérez, 2020).
Thus, the theory of social representations (SRT) seeks to explain how we appropriate and represent new concepts, with implications for group and individual behaviour (Jodelet, 1989; Moscovici, 1976). Through social representations, individuals create shared cognitive conceptions which represent a filter for groups to interpret the new phenomena and to act upon them (Vala & Castro, 2017). SRT can be helpful to understand how this new risk to social health is transformed and appropriated by the group. This framework has been extensively studied in other epidemics or infectious diseases (Eicher & Bangerter, 2015) such as SARS (Washer, 2004), Ebola (Idoiaga et al., 2017; Joffe & Haarhoff, 2002), tuberculosis (Ascuntar et al., 2010) and AIDS (Rodrigues et al., 2014), explaining human conduct in the face of threat.
This analytic process begins with studying the formal and informal speech around the subject (Pérez, 2004). Moscovici defined two concurrent processes with regard to social representation formation: objectification and anchoring. Objectification is the process that allows new and abstract concepts to become concrete, using a selective strategy to decontextualize information and organize it in a figurative representation (Abric, 1996).
Social speech around COVID-19 is focused on metaphors such as combat, fight and defeat (Jaspal & Nerlich, 2020). In Portugal, since confinement measures in response to COVID-19 were first enacted, communication has been based on counting the number of infections and deaths; the president of the republic, following the communication paradigm used by other governmental elements such as those of France and Italy, referred to public-health responses to COVID-19 as being ‘at war with an invisible and insidious enemy’. This metaphoric language appeals to the nation’s fear and unification against an enemy.
The anchoring process, in social representations, enables the classification of the new and unknown, using existing shared categories. It will also establish a link between the new pandemic and similar previous events, helping to understand the latest phenomenon in continuity with the past ones (Camargo & Bousfield, 2009; Camargo et al., 2011). Concerning COVID-19’s social representation, it is known to have been anchored to HIV in the media (Yong, 2020, as cited in Jaspal & Nerlich, 2020). In Portugal, this anchoring was made with the flu. Despite the importance of knowing how these processes socially develop, it is also relevant to understand how they get cognitively organized (Abric, 1996). The structure of social representation may be valuable to explain how it functions and how it applies to human action. Abric (1993) proposed that social representations are organized into two interdependent systems, the central core and the peripheral system.
The central core contains impressions of the collective memory. It should be common, consensual to a group of individuals and collectively shared. It is stable, resistant to change and has the function of organizing all the elements that constitute the social representation.
The peripheral system would be an interconnection between reality and the central core, contextualizing social representation. It provides flexibility and an individualized expression — it concretizes, regulates and defends the central core. It will also ensure the concretization of the central system in terms of assuming a position and behaviours (Abric, 1996). Knowing a social representation, therefore, requires knowing its structure (Wachelke, 2009).
Vergès (1992) and Vergès et al. (1994) developed a methodology using a technique of free evocations to assess the structure of social representations. The analysis that emerges from this technique, prototypical evocations analysis, allows us to identify the beliefs, ideas and values central to a representation. It uses the frequency and order in which they are evoked, based only on the presentation of the concept whose social representation we intend to measure. The criteria for this analysis are the absolute frequency of evocations and the average order in which each word is evoked, allowing us to distinguish the central core from the peripheral system (Gomes & Nunes, 2015; Wachelke & Wolter, 2011). The core is expected to be related to our beliefs and attitudes and to determine representational behaviours (Vala & Castro, 2017). The peripherical system implicates values and beliefs that allow us to normalize and respond to change, maintaining the core intact. It may allow us to contextualize our own experience, despite the similarity of values and beliefs among the group (Gomes & Nunes, 2015).
Several studies have started from this point of reasoning and tried to clarify COVID-19 social representation. Colì et al. (2020), using Vergès’s (1992) prototypical analysis, found a social representation structured on fear, a shared emotion that revolves around the risk of contagion and the current pandemic state. Personal experience has been found to affect the structure of peripherical elements. Fasanelli et al. (2020), comparing humanities and life sciences students, observed a 65% overlap in the central core in both groups. The overlapping elements included quarantine, anxiety, pandemic, personal protection equipment, fear, death, virus, lockdown and loneliness. Bú et al. (2020) applied ALCESTE analysis to evocations about COVID-19. They observed the emergence of two themes subdivided into four classes. The social representation focused on concerns related to dissemination, and psychosocial and emotional implications. Fear, panic, danger and empathy are words significantly associated with the psychosocial and affective implications of the virus (constituting a single thematic class with the highest percentage of the corpus). These concerns are associated with being a woman, being from the south and earning between three and four minimum wages.
The emotional concerns are not exclusive to adults, as Idoiaga et al. (2020) observed exploring children’s social and emotional representations of the COVID-19 pandemic. Children expressed fear of the pandemic, especially focusing on concerns with the elderly (grandparents).
We expect the Portuguese COVID-19 social representation to replicate this process of formation and, therefore, to present a similar pattern in functioning, presenting a central core focused on affective implications and dissemination concerns.
As noted earlier, social representations are built upon information available, by formal and informal social communicators. Differently from other pandemics, COVID-19 is described to be infodemic as well; in that characterization, a great amount of information is disseminated, not always true or verifiable, which seems to influence individual behaviour (Cinelli et al., 2020).
Knowledge has effects on beliefs and behaviours. The misinformation around COVID-19 has been associated with poorer knowledge, less engagement in protective behaviour and misinformed beliefs about this subject (Lee et al., 2020). Knowledge about COVID-19 has been observed to be high in health care practitioners and health students (Khader et al., 2020; Maheshwari et al., 2020; Shi et al., 2020), although with less consistent results in other studies. US college students appear to have inconsistent knowledge about COVID-19 (Chesser et al., 2020), while the Saudi Arabian general population is described as having high literacy, associated with optimistic attitudes, despite less knowledge, less optimistic attitudes and worse health practices in men rather than in women (Al-Hanawi et al., 2020). Nigeria’s population has also been described as having good COVID-19 literacy derived from formal health information (Olapegba et al., 2020, under review). In Portugal, a study was conducted concerning knowledge, attitudes and behaviours of adolescents (Alves et al., 2021). Participants reported high knowledge but were less engaged in protective behaviours. To the extent of our knowledge, knowledge about COVID-19 in adults is yet to be studied. Considering the previous studies, however, it is expected to be high, especially in educated female participants.
Social representation organizes the cognitive information regarding the new social subject (Abric, 1996), and in the case of COVID-19, the values and beliefs that we appropriate during this process might influence attitudes towards it. Attitudes are described as a psychological tendency, relative to a specific entity, expressed through a degree of favourability or unfavourability (Eagly & Chaiken, 1993). This tendency has an evaluative purpose, and it is usually classified as having three different types of responses from which it could be inferred (Ajzen, 1989): cognitive responses, affective responses and conative (behavioural) responses.
While cognitive responses relate to beliefs towards an attitudinal object, the affective responses have more to do with feelings towards that object. The conative responses show behavioural inclinations, intentions or actions towards the object. Ajzen (1989) considered the possibility of collecting both verbal and nonverbal responses, from the three types. If social representations concern more of a dynamic composition of beliefs shared and built by a group, attitudes represent an individual appropriation of a social object (Marková, 2017). The expectation is to see a relation between the cognitive content of the social representation and the attitude towards COVID-19, since the ‘attitude about an object of representation is based on the evaluative components in its representation’ (Moliner & Tafani, 1997, p. 698). Therefore, in this study we expected to find an attitude that relates to the social representation of COVID-19.
Given the impact of COVID-19 and the behavioural modification it implied in our life, it seems pertinent to investigate the functioning of social representation, the originating attitude and the degree of knowledge about this infectious disease. This measurement may help us to understand how to adopt healthier and protective behaviours that are expected to be required in the next 12 to 24 months until group immunity or a full working vaccine for the disease is achieved (e.g., social distancing, prophylactic isolation, respiratory etiquette, hand hygiene and disinfection of surfaces).
Thus, the objective of this study was to measure the structure of the social representation of COVID-19 and to describe the attitudes and the level of knowledge about the disease in a heterogeneous sample of the Portuguese population, and to establish questions for further investigations, which will facilitate the introduction of health protection behaviours against SARS-CoV-2 or other infectious pandemics.
Method
Participants
The sample of this study was selected from the Portuguese literate adult population (aged > 18 years), using a non-probabilistic (i.e., ‘snowball’) sampling technique.
Two hundred and ninety-four participants were selected, all of Portuguese nationality, with an average age of 42 years (M = 42.54, SD = 12.32, Median = 40.0, Max. = 78 years). Of this cohort, 85% were women. In their geographic characterization, 23.5% were from Algarve, 37.8% were from the Lisbon region and 10% were from the greater Porto region, with the remaining participants originating from Alentejo, Minho, Trás-os-Montes, Madeira and the Azores (percentages below 5%). About 66% of the participants were married, and 60% reported dependents (M dependents = 1.6, SD = 0.497). Regarding education, 36.1% were post-Bologna graduates/masters, and 18.8% had completed high school/secondary education; education ranged between the second cycle of basic education (six years in school, 2.4%) and the PhD degree (2.4%). The sample could be defined generally as middle-aged, female, educated, married and with dependents.
The participants were also asked if they knew someone infected with COVID-19, to which 98% of the participants answered that they did not. We assessed risk perception by asking participants, ‘What is the estimated probability of being infected with COVID-19?’ They answered on a scale of 1 (‘not at all likely’) to 5 (‘very likely’); 6.8% responded that it was very likely (5), 10.9% likely, 35.4% uncertain, 24.8% unlikely and 22.1% not at all likely (1). Generally speaking, participants do not believe in the possibility of becoming infected with COVID-19.
Measures
COVID-19 social representation
A free evocation technique was used, considering the expression coronavirus/COVID-19 as a stimulus to the task. Participants were asked to write up to five words or expressions (not phrases) that the presented concept/words suggested to them, always in the order that they remembered them. Five visual spaces were provided for this purpose, where they could enter their responses.
Attitude towards COVID-19
Using the website of the DGS [Portuguese general health directorate] for official and updated information on scientific advances on COVID-19, several items were constructed referring to three attitudinal components about the disease: cognitive component, affective/emotional component and behavioural component (see Appendix A).
The component related to cognition concerns personal beliefs about the plausibility of infection with COVID-19, personal affect, understanding or perception of personal risk (a total of six items).
The affective component concerns emotions and feelings caused by this plausibility of infection and personal affect (total of six items).
Finally, the behavioural dimension concerns the behaviours adopted (or oral behavioural change) since the appearance of COVID-19 (a total of eight items).
Adjustment of the three-factor model of attitude towards COVID-10
Note: CFI — Comparative Fit Index; TLI — Tucker-Lewis Index; RMSEA — Root Mean Square Error of Approximation; SRMR — Standardized Root Mean Square Residual.
After calculating the final reliability measures, the cognitive dimension has a Cronbach’s alpha of .650, the affective dimension of .888 and the behavioural dimension of .926, all values considered favourable to the construction of composite measures.
Higher scores in the cognitive dimension show a greater tendency to believe in COVID-19 as a personal and social risk. Higher scores in the affective dimension suggest greater feelings of anxiety, fear about COVID-19, preoccupation towards individual risk and possible infection outcomes. Finally, a higher score in the behavioural dimension shows a greater tendency to change or monitor one’s behaviour or health status in the face of the COVID-19 pandemic situation.
Knowledge about COVID-19
Using the most frequent questions and information available on the DGS website, 10 sentences were constructed regarding the viral agent responsible for COVID-19, the known means of transmission and knowledge of the vaccine, cure and prevention. The possible response options were ‘true’, ‘false’ or ‘don’t know’. One point was assigned for each correct answer, with a degree of correct answers varying between 0 and 10. A negative point was also assigned to each incorrect answer. No point was assigned for ‘don’t know’, but the percentage of uncertainty was determined for each question. The total degree of knowledge was determined mathematically, subtracting incorrect scores from correct scores. The higher the total value, the greater the degree of knowledge of the participant.
Risk perception
Two questions were included to measure risk perception. Participants were asked to classify the probability of being infected with COVID-19, from 1 (‘totally unlikely’) to 7 (‘completely likely’), and to answer positively if they know someone infected with COVID-19 (dichotomous question, ‘yes’/‘no’).
Data collection procedure
Participants were contacted through social networks, and data were collected using an online survey. All participants were informed of the purpose of the study. To respond they had to consent to participate voluntarily in the study, recognizing that they would never be asked for personal data that would identify them or that would imply further contacts.
All data collected were generic and did not identify participants, with anonymity and confidentiality of responses guaranteed. There were no rewards or risks for participating in the study. At any time, participants reserved the right to withdraw from the study by closing the browser window where they were responding to the questionnaire.
All data were collected after the determination of social isolation measures, between March 11 and 26 March 2020.
Data analysis procedure
We defined the structure of a social representation using Vergès’s (1992) prototypical analysis. It assumes the use of both raw and categorized words. We opted to use raw forms. The frequency and order of evocation are considered in the analysis.
The criteria for analysing the evocations are determined as follows: minimum frequency — the minimum absolute frequency for words to be considered in the analysis; intermediate frequency — the absolute frequency that distinguishes high-count words from low-count words; the average evocation order (OME) — which classifies the average evocation of each word; and the average of the average orders of all evocations, a criterion that allows distinguishing the words evoked more primarily from those evoked secondarily.
The words most frequently observed and whose average order of evocation is lower than the average of all OMEs will probably constitute the central core of social representation. In contrast, the least evoked words, with an average of evocation higher than the average of all OMEs, will probably constitute the peripheral system.
IRaMuTeQ software was used to conduct the prototypical analysis and the similitude analysis (frequency of co-occurrences and Chi-square association test).
For the analysis of data that allows establishing the relationship between social representation, attitude towards COVID-19 and knowledge, bivariate correlations were used between the frequency of evocations, knowledge and the scores obtained between cognitive, affective and behavioural dimensions of attitude towards COVID-19.
All analyses were considered statistically significant at a 95% significance level.
Results
Social representation of COVID-19/coronavirus
The 294 participants performed 1,362 evocations, using 231 distinct words. Words evoked by at least 5% of the sample were considered as minimum frequency, which resulted in thresholds of 15 occurrences. This criterion reduced the corpus to 25 distinct words, which corresponds to a retention rate of 11%. These 25 words also correspond to 67% of all evocations performed.
The intermediate frequency was performed through the average frequency of all evocations (M = 39.36).
Average evocation orders are a weighted average of the frequency of words in the order in which they are evoked. The average of the average evocation orders is found through the OME of the words retained. Figure 1 shows the social representation of COVID-19. This analysis was conducted according to the technique of prototypical analysis (or evocation analysis) by Vergès (1992) and considering the suggestions provided by Wachelke and Wolter (2011) and Gomes and Nunes (2015). Social representation of COVID-19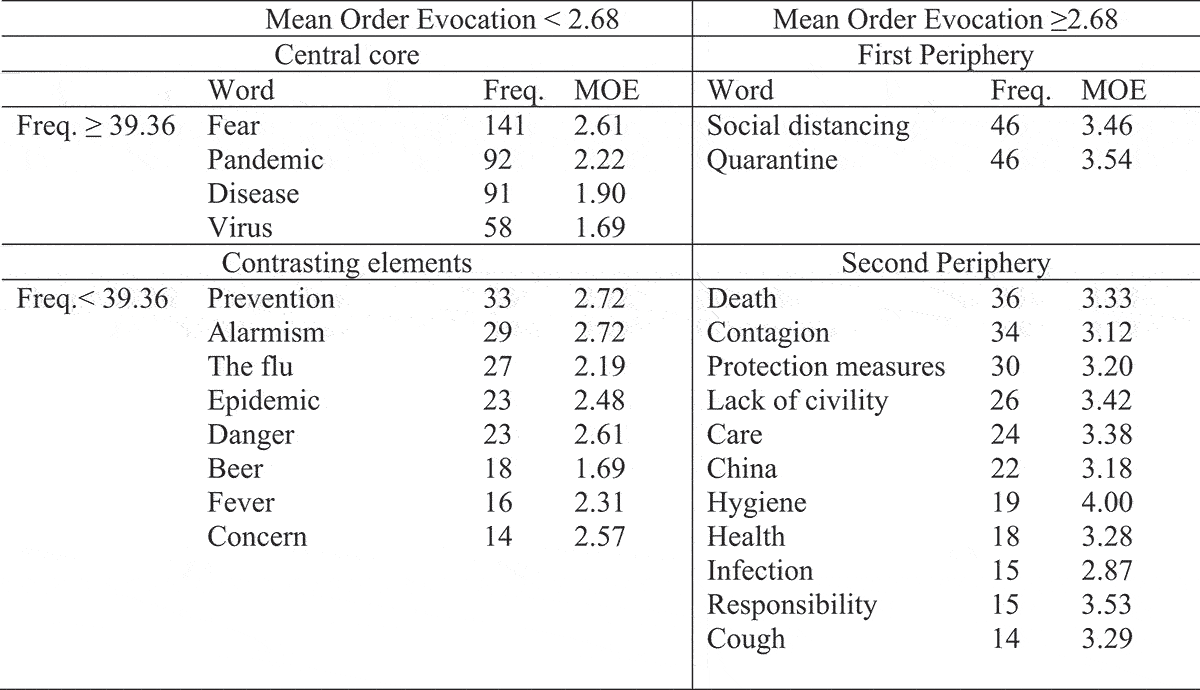
The central core zone includes fear, pandemic, disease and virus. Fear is the most frequent word. It describes an emotion about COVID-19. The rest of the central core words imply a description of the situation: pandemic, disease and virus. The first periphery includes two possible situations that involve isolation: quarantine and social distancing. In the contrasting elements, we found previous concepts used for anchoring: the flu, beer (a reference to Corona beer) and words related to the characterization of this disease: danger, epidemic and fever. Finally, the second and more external periphery presents several perspectives or positions about COVID-19.
The similitude analysis (Figure 2) allows establishing the concurrences between the words evoked. Results of the lexical similarity (co-occurrence) analysis produced by the free association task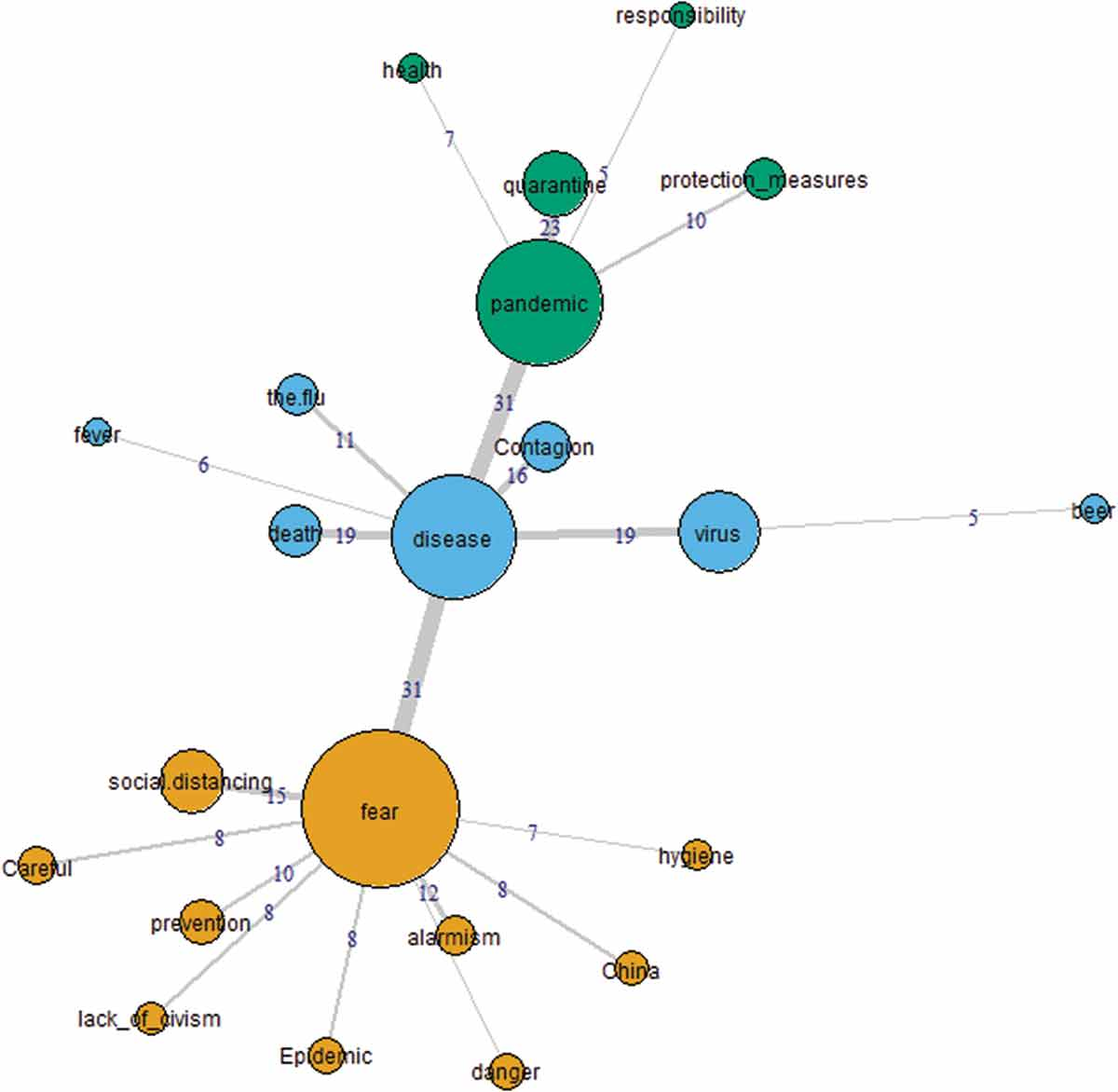
Fear, pandemic and disease — all concepts from the central core — seem to organize the evocations in three branches or communities. Fear co-occurs mainly with social distancing, but also with alarmism and prevention. Fear is linked with disease but not with pandemic.
Disease presents its highest co-occurrence with virus and death, followed by contagion and the flu. It also establishes a high co-occurrence with pandemic.
Pandemic showed higher proximity with quarantine, follow by protection measures. These associations were also tested for association with the Chi-square test (Figure 3). Results of the association (Chi-square test) between evocations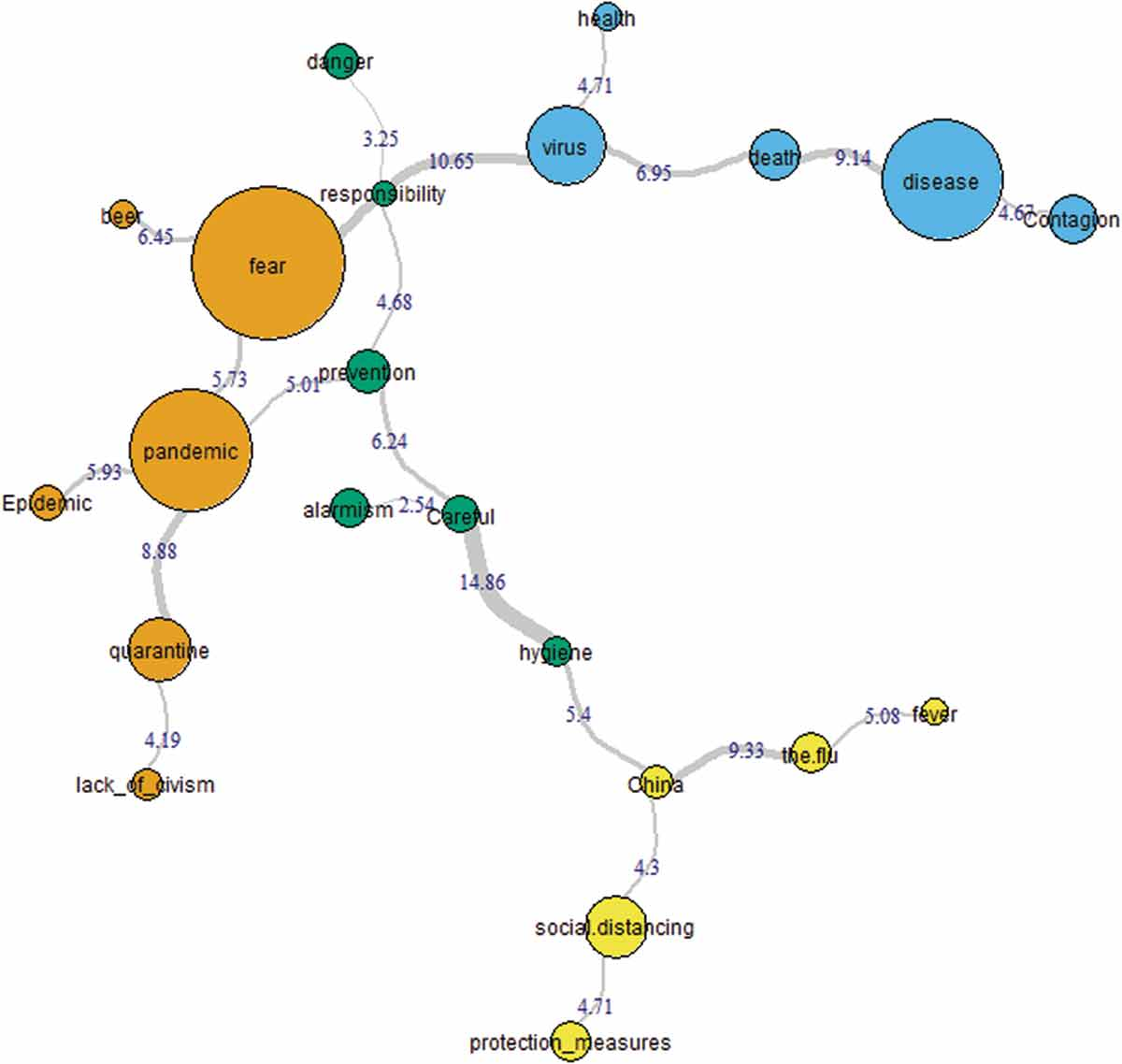
All values were considered statistically significant for Chi-square values above 3.841 (confidence level 95%; n/F = 1).
The strongest associations were established between careful and hygiene, fear and virus, disease and death, China and the flu, and between pandemic and quarantine. Evocations seem to be significantly associated between them, except for danger and responsibility, and alarmism and careful.
Attitudinal components towards COVID-19
Pearson’s correlations between cognitive, affective and behavioural dimensions of attitude towards COVID-19
Knowledge in the face of COVID-19
Rate of correct answers and lack of knowledge about COVID-19
We assessed the accuracy of knowledge by the differential between correct and incorrect answers. With a minimum of −2.00 to a maximum of 10.00, the average of knowledge is 5.53 (SD = 2.528). Knowledge is not affected by the participant’s age (p = .466) or education (p = .333).
Relationship between social representation, knowledge and attitude towards COVID-19
Pearson’s correlations between knowledge and attitude towards COVID-19
Note: *p < .05, **p < .01, ***p < .001.
There is a strong, positive correlation between the correct and incorrect answers, showing that getting the answers right also implies more incorrect answers.
However, there is a strong negative correlation between correct answers and lack of knowledge. This result suggests that greater accuracy is seen among those who are least likely to report not knowing the information questioned. In contrast, errors and uncertainty are positively correlated, but the correlation is weak. So, it is possible to assume that greater accuracy is not necessarily conditioned on being well informed.
Pearson’s correlations between COVID-19 social representation, knowledge and attitude
Note: *p < .05, **p < .01, ***p < .001.
The results show a positive relationship between the affective dimension of the attitude towards COVID-19 and pointing out fear and danger in social representation, with fear being one of the concepts that are part of the central core. A higher score in the affective and behavioural dimension of the attitude towards COVID-19 seems to be correlated with not indicating flu and beer.
About knowledge, the individuals who had more incorrect answers were the ones who least showed concern and incivility in the social representation of COVID-19; those who have more correct answers seem to evoke more social distance.
Discussion
Our objective was to measure the social representation of COVID-19, to characterize the attitude and knowledge about the SARS-CoV-2 virus and its infectious disease that is responsible for the current pandemic, which has physical, mental, social and economic consequences, at a global scale.
Social representation was described based on Abric’s central core theory (1993) using the prototypical analysis of Vergès (1992). A social representation was found that retained 67% of all evocations carried out, with a total of 25 words in the analysis. There was no categorization of the evocations; instead we opted for a more conservative analysis. However, the proximity between some words suggests that a more parsimonious representation could have been achieved if we had grouped the words by lexical similarity.
A general observation of the social representation of COVID-19 shows, unsurprisingly, a negative characterization of the phenomenon. This is a new threat, demanding and with high implications for people, and they may be experiencing negative feelings about it. It is precisely an emotion — fear — that is the most evoked word, which represents a shared and common emotion concerning the possibility of contagion. The central core also includes concepts concerning the core of this situation: pandemic, disease and virus. The construction of the social representation seems to rely on its characteristics: it is a disease promoted by a virus, that resulted in a pandemic.
Previous studies about infectious diseases have showed similar social representations, with fear presenting as a central aspect. The social representation of Ebola in Spain (Idoiaga et al., 2017) and the UK (Joffe & Haarhoff, 2002) showed the presence of fear, however without a sense of personal threat. Washer (2004) showed fear as a trace in the social representation of SARS, although it contained a mechanism that differentiated those who are at risk (others) from those who are not (I, us). Colì et al. (2020) conducted a similar study to this, using a free association task in the Italian adult population. Social representation presented contagion, fear and pandemic in the central core system. In the study we also observe the similarity with other viral infection epidemics. However, there was no ‘othering’ mechanism in the representation. The personal risk or personal threat seems to be implied in this representation. Also, our results show a replication of media discourse about COVID-19, which has an impact on the formation of social representation, and in preventive behaviour and management of fear.
The social representation observed in this study presents values such as responsibility, protection measures, prevention, social distancing and hygiene, which suggests a sense of personal threat and individual responsibility.
Nevertheless, we should consider that China is present in the evocations, and associated with fear. There is also an association with the flu. De Rosa and Mannarini (2020) argued that the global impact of COVID-19 increased the consciousness of human vulnerability and pictured humankind as the in-group. This might increase the awareness that we are all at risk. Thus, the previous association (China and fear) can be interpreted as a reliance on the origin of the virus, rather than on an ‘othering’ mechanism.
However, the association established with the flu seems to be a spillover from the media discourse of COVID-19 being the ‘Chinese flu’, which supports the idea that the ‘others’ (Chinese) are responsible for this situation. Páez and Pérez (2020) reflected on this matter, showing that anchoring the disease to an out-group is a common process in representing epidemics. As they argued, these out-groups are considered anti-hygienic or having anti-hygienic practices. This seems to have been applied to COVID-19 in a xenophobic but broadly reported media representation, as US President Donald Trump labelled it as the ‘Chinese flu/Chinese virus’. This media representation might have been sufficient for the general public to associate anti-hygienic practices with the Chinese people, increasing stigmatization and differentiation from Western societies. In fact, in our study, China is also associated with hygiene, showing a possible villainization of the Chinese in this situation. Portuguese people may be blaming China or Chinese people for the pandemic, due to cultural phenomena such as widespread sales of non-domesticated animals (so-called ‘wet markets’) and hygiene practices.
In Portugal, the media discourse was less focused on the stigmatization of an out-group and relied more on a ‘state of war’, which was continuously used to address the virus. ‘Insidious enemy’ and a ‘battle to be fought by each and every single one of us’ were expressions used by governmental ministers and the president. This increased the personal sense of risk and behavioural implications to contain the COVID-19 pandemic.
In response to COVID-19, Portugal, like other countries, relied on compulsory confinement, social distancing, appeal to personal hygiene and the use of masks to control the number of contagious transmissions in the population. The first periphery words seem to reflect this. The category includes only two words: quarantine and social distancing. Also, one of the requisites of air-transmitted virus is isolation, for those who are ill (quarantine), and social distancing to prevent infections. However, while quarantine co-occurs with pandemic, social distance co-occurs with fear, suggesting that people might have a negative affective impression of these measures. Fear is also associated with alarmism, which seems an attempt to diminish the risk perception of the situation. This type of communication towards an enemy, with references to war, has been discussed in the literature as posing difficulties to cognitive and emotional features of cooperation and care for others (Sabucedo et al., 2020).
Although it seems intuitive that the reaction to fear is to look for behaviours that prevent the risk, studies on health preventive behaviours do not show this association in an obvious way. Ruiter et al. (2001) suggested that fear is less motivating than the perception of the effectiveness of the action and the self-efficacy of individuals in dealing with threats. The perceived personal relevance may also be critical to the emotional and perceived impact of the available information about the threat. Lench and Levine (2005) suggested that fear may diminish unrealistic, optimistic beliefs; however, the more fear the participants reported, the less control they believed they had in the result, and less memory of the risk itself, which results in a decrease in preventive behaviours. Kok et al. (2018) pointed out that the role of fear may be more harmful than beneficial in adopting healthy behaviours or avoiding threats, with individuals being dependent on the perceived self-efficacy to deal with this threat.
Joffe (2003) suggested that texts and images are processed through pre-existing representations. The anchoring with the flu may be constraining how we are processing the information available about the disease, diminishing risk perception. In fact, most of our sample expressed unlikelihood at becoming infected with the virus, despite the increasing number of infections. Also, the dynamics are expected to shift, and fear as an emotional reaction is expected to decline (Mayor et al., 2012), which might give people an illusional perspective of being safe and lead them to abandon the preventive measures, or at least feel that they might collide with the democratic values of liberty of expression and action.
Nevertheless, this representation seems to serve its sense of collective symbolic coping (Páez & Pérez, 2020). It includes information regarding methods to control the infection (hygiene, social distancing, protective measures), clear information on symptoms (fever), but also an anchoring to the known flu and a link to China (first known outbreak of the disease). Anchoring this unknown life-threatening disease to known concepts, such as the flu, serves the representational purpose of normalizing and making the situation familiar
Moscovici, 1976), while it provides useful information on how to deal with it and to make behavioural adjustments in terms of protection. Nevertheless, the information surrounding the virus’s manifestation and behaviour is still changing, and it is expected that a transformation of this social representation might occur.
Participants seem to be well informed concerning protective measures and identification of symptoms of the infection. Of the respondents, 93.5% know that this virus does not affect solely elderly people, 89.1% know they should not go to health primary centres if they have symptoms of infection, and they know that coughing and fever are the symptoms to mind. However, almost half of the sample believes COVID-19 is identical to the flu virus, and more than 60% believe the origin of the virus is well established. Our participants seem to have inconsistent knowledge.
Our results seem to support those of Chesser et al. (2020), who found inconsistent knowledge about COVID-19 among college students. Available studies on knowledge and attitudes about COVID-19 (Gupta et al., 2020; Khader et al., 2020; Shi et al., 2020) have showed that the samples involved — schooled, linked to the health area — had a high level of knowledge, although they may have some deficits in advanced preventive measures (Khader et al., 2020). From a functional point of view, the sample under study has a high level of knowledge in hygiene measures, symptoms and procedures in case of infection. However, there seems to be a set of mistaken beliefs about the infection, namely over the origin of the virus (at the time of measurement), similarity or dissimilarity with the flu, disease treatment and means of transmission. The level of knowledge seems, therefore, to be lower than the groups linked to the health groups. However, it seems to be high in the most relevant dimensions for personal protection.
This inconsistency, although expected, reinforces the use of social representation to manage the risk information available. Contrary to other pandemics, COVID-19 has been characterized by a continuous flux of information, on several media platforms. Information is available and was widely disseminated. More than considering people to be misinterpreting information or having erroneous information processing, we should be considering the hypothesis that social representation is shaping how individuals are reacting to COVID-19 and constructing their representation of not being at risk. As Joffe (2003) concluded in a review, social representation theory contributes to risk theory by ‘positioning how the “we” enters into and constructs the representation of the “I”’ (p. 68).
There also seems to be a relation between the knowledge presented and the individual evocation profile. Individuals who more frequently answer ‘don’t know’ tend to also more frequently evoke the word alarmism; those who have more incorrect answers tend to less frequently evoke the words concern and lack of civility; those with higher rates of correct answers tend to more frequently evoke social distance. These results suggest that an inferior degree of literacy concerning COVID-19 may result in an appropriation of the social representation that relies on peripheral elements to adjust personal experience and increasing risk. All of this is particularly interesting if we consider this pandemic as being an infodemic (Cinelli et al., 2020). Misinformation around COVID-19 has been associated with poorer knowledge, less engagement in protective behaviour and misinformed beliefs about this subject (Lee et al., 2020).
Regarding attitudes, the results suggest that the participants do not seem to believe in the possibility of being infected with the virus or even being concerned about this possibility. There was a slightly higher concern in changing behaviour.
We expected to observe a relation between the content of COVID-19’s social representation and the attitude measured. Nevertheless, this relation is not clear or well established. The correlations are weak, barely indicative of possible associations between the evocations and the evaluation of COVID-19.
Individuals with higher scores in the affective dimension of the attitude seem to more frequently evoke fear and danger, and less so flu and beer. Those who evoke danger seem to be more likely to change their behaviour to protect themselves. Evoking the flu is associated with a less anxious/worried position and with a lower propensity to change behaviours (e.g., more frequent hand hygiene). The evocation of beer — in an allusion to the Corona beer brand — is inversely related to the affective and behavioural dimensions, and a more permeable attitude to COVID-19 is expected.
It should also be noted that the rate of ‘I don’t know’ answers is inversely associated with the behavioural dimension. Those who most frequently report ‘I don’t know’ seem to change their behaviour less. These are also the individuals who most evoke the word alarmism.
The expected relation between social representation and attitude is not present. We expected social representations to be feeding the attitude towards COVID-19, as attitudes of an object are based upon social representation components (Moliner & Tafani, 1997). However, we must consider that the great contribution of social representations is based, precisely, on the dynamic process of their formation. Understanding the social representation from the static point of view of the cognitive organization is taking away from it the information wealth about the way the world is apprehended and the process of deconstruction of the object, for the creation of common sense (Joffe, 2003).
Even if it is not linear, the social representation of COVID-19 may be showing the emergence of two groups. They are collectively forming different representations that serve their self-identity. There is a group that has a less favourable attitude towards COVID-19, which has a more considerable preoccupation/anxiety concerning the disease and has a greater behavioural intention to maintain behaviours compatible with individual protection (hand hygiene, respiratory etiquette and social distancing). This group seems to have a representation about fear, protection, social distancing and civic behaviour. On the other hand, there seems to be another group with a more favourable attitude towards COVID-19, with less anxiety/concern and less intention to change behaviour. This second group is more oriented towards alarmism, beer and the flu, presenting higher levels of ‘don’t know’ answers (regarding their knowledge).
Further studies
The study was conducted early in the COVID-19 pandemic, while the social representation was formed. Mayor et al. (2012) showed how patterns in social representation change along with the pandemic situation. The social representation found in this study has several elements from the first contact with the risk threat (a responsible out-group, classification of symptoms, ways to diminish risk infection). With the spread of the infection, it is presumable that more persons will be infected, or will know people who had the infection, or will even feel the consequences of the pandemic. Knowledge about COVID-19 is increasing rapidly and continues to be disseminated to laypeople. Therefore, an evolution in social representation is expected, and it should be studied, since it seems to contribute to explaining the complexity of individual behaviour towards COVID-19.
La representación social, las actitudes y los conocimientos de la población adulta portuguesa sobre la COVID-19
El nuevo coronavirus (2019-nCoV) o SARS-CoV-2 es un virus de gran propagación que causa la enfermedad COVID-19. La pandemia de COVID-19 que se inició a principios de 2020 ha cambiado la vida de las personas a nivel individual, social y socioeconómico. Una enfermedad infecciosa representa un riesgo real para la humanidad que requiere ciertos ajustes a nivel individual y grupal, incluso con una posible vacuna, como ya se ha podido comprobar.
Para poder afrontar un fenómeno como la pandemia de COVID-19, las representaciones sociales surgen espontáneamente para gestionar y organizar esta nueva realidad, imprevisible y cambiante (Colì et al., 2020). Por tanto, las representaciones sociales pueden concebirse como formas de afrontamiento simbólico colectivo (Páez & Pérez, 2020).
Por tanto, la Teoría de las representaciones sociales (TRS) trata de explicar cómo las personas nos apropiamos y representamos nuevos conceptos, con sus correspondientes implicaciones en los comportamientos grupales e individuales (Jodelet, 1989; Moscovici, 1976). A través de las representaciones sociales, las personas crean conceptos cognitivos compartidos que actúan a modo de filtro en la interpretación que los miembros del grupo hacen del nuevo fenómeno y en su comportamiento respecto a este (Vala & Castro, 2017). La TRS puede ser útil para comprender cómo el grupo transforma y se apropia de esta nueva amenaza para la salud social. Se trata de un escenario que ha sido ampliamente estudiado en otras epidemias y enfermedades infecciosas (Eicher & Bangerter, 2015) como el SARS (Washer, 2004), el ébola (Idoiaga et al., 2017; Joffe & Haarhoff, 2002), la tuberculosis (Ascuntar et al., 2010) o el SIDA (Rodrigues et al., 2014), y que explica el comportamiento humano frente a una amenaza.
El proceso analítico comienza con el estudio del discurso formal e informal sobre el tema en cuestión (Pérez, 2004). Moscovici define dos procesos simultáneos relativos a la formación de la representación social: objetivación y anclaje. La objetivación es el proceso que permite concretizar nuevos conceptos abstractos aplicando una estrategia selectiva para descontextualizar la información y organizarla en una representación figurativa (Abric, 1996).
El discurso social sobre la COVID-19 se centra en metáforas en las que se utilizan términos como combate, lucha y derrota (Jaspal & Nerlich, 2020). En Portugal, desde la introducción de las medidas de confinamiento en respuesta a la enfermedad, la comunicación ha consistido básicamente en contar el número de personas infectadas y fallecidas. El presidente de la República, siguiendo el mismo patrón de comunicación utilizado por otros gobiernos como el francés o el italiano, se refería a la respuesta de la sanidad pública frente a COVID-19 como ‘una guerra contra un enemigo invisible e insidioso’. Este tipo de lenguaje metafórico apela al miedo y a la unidad de la nación frente al enemigo.
El proceso de anclaje de las representaciones sociales facilita la clasificación de lo nuevo y lo desconocido, utilizando categorías existentes compartidas. También permite establecer un vínculo entre la nueva pandemia y acontecimientos previos similares que nos ayuda a comprender el fenómeno reciente en continuidad con los anteriores (Camargo & Bousfield, 2009; Camargo et al., 2011). Por lo que respecta a la representación social de la COVID-19, sabemos que en los medios de comunicación se ha vinculado esta enfermedad con el SIDA (Yong, 2020, citado en Jaspal & Nerlich, 2020). En Portugal, el anclaje se ha vinculado con la gripe. Si bien es clave conocer cómo se desarrollan socialmente estos procesos, también es relevante comprender cómo se organizan cognitivamente (Abric, 1996). La estructura de la representación podría ser de ayuda para explicar su funcionamiento y su impacto en la acción humana. Abric (1993) propuso que las representaciones sociales se organizan en dos sistemas interdependientes, el núcleo central y el sistema periférico.
El núcleo central contiene impresiones de la memoria colectiva y debe ser común y consensuado por un grupo de personas que lo comparten colectivamente. Es estable, resistente al cambio y tiene la función de organizar todos los elementos que constituyen la representación social.
El sistema periférico podría ser una interconexión entre la realidad y el núcleo central que contextualiza la representación social. Le facilita flexibilidad y una expresión individualizada; concretiza, regula y defiende el núcleo central. También garantiza la concretización del sistema central en términos de asumir una posición y ciertos comportamientos (Abric, 1996). Conocer una representación social, por tanto, requiere conocer su estructura (Wachelke, 2009).
Vergès (1992) y Vergès et al. (1994) desarrollaron una metodología utilizando la técnica de la evocación libre para evaluar la estructura de la representación social. El análisis que emerge de esta técnica de análisis prototípico de evocaciones, nos permite identificar las creencias, las ideas y los valores centrales de una representación. Hace uso de la frecuencia y el orden en el que se evocan las palabras, basándose únicamente en la presentación del concepto cuya representación social se pretende medir. Los criterios para este análisis son la frecuencia absoluta de las evocaciones y el orden promedio en el que se evoca cada palabra, lo que nos permite distinguir el núcleo central del sistema periférico (Gomes & Nunes, 2015; Wachelke & Wolter, 2011). Anticipamos que el núcleo estará relacionado con nuestras creencias y actitudes, y determinará los comportamientos representacionales (Vala & Castro, 2017). El sistema periférico implica ciertos valores y creencias que nos permiten normalizar y responder al cambio, manteniendo intacto el núcleo central. Nos puede permitir contextualizar nuestra propia experiencia, a pesar de la semejanza de valores y creencias dentro del grupo (Gomes & Nunes, 2015).
Diversos estudios han adoptado este razonamiento como punto de partida y han tratado de esclarecer la representación social de la COVID-19. Colì et al. (2020), utilizando el análisis prototípico de Vergès (1992), identifica una representación social estructurada en torno al miedo, una emoción compartida que gira en torno al riesgo de contacto y el estado actual de la pandemia. Se ha observado que la experiencia personal influye en la estructura de los elementos periféricos. Comparando estudiantes de humanidades y de ciencias de la vida, Fasanelli et al. (2020) observaron un solapamiento de 65% en el núcleo central de ambos grupos. Entre los elementos que se solapaban, se identificaron: cuarentena, ansiedad, pandémica, equipos de protección personal, miedo, muerte, virus, confinamiento y soledad. Bú et al. (2020) aplicaron un análisis ALCESTE a las evocaciones sobre la COVID-19. Observaron la emergencia de dos temas subdivididos en cuatro clases. La representación social se centraba en cuestiones relacionadas con la propagación del virus y con las implicaciones psicológicas y emocionales. Miedo, pánico, peligro y empatía son palabras que se asocian significativamente con las implicaciones psicológicas y afectivas del virus (y que constituyen una única clase temática con el porcentaje más elevado del corpus). Estas cuestiones están relacionadas con el ser mujer, del sur, y tener unos ingresos equivalentes a tres o cuatro veces el salario mínimo.
Las preocupaciones emocionales no son exclusivas de los adultos, como ya mostraron Idoiaga et al. (2020), observando las representaciones sociales y emocionales de la pandemia de COVID-19 en los niños. Los niños expresaron miedo por la pandemia, centrado especialmente en los mayores (abuelos).
Esperábamos que la representación social de la COVID-19 en la población portuguesa reprodujese este proceso de formación y, por tanto, presentase un patrón similar de funcionamiento, con un núcleo central enfocado en las implicaciones afectivas y la preocupación por la propagación del virus.
Como ya hemos comentado, las representaciones sociales se construyen sobre la información disponible a través de comunicadores formales e informales. A diferencia de otras pandemias, la causada por la COVID-19 se describe también como infodémica; con esta descripción se hace referencia a una enorme cantidad de información, no siempre verdadera o verificable, que parece influir en el comportamiento individual (Cinelli et al., 2020).
El conocimiento influye en las creencias y en los comportamientos. La desinformación en torno a la COVID-19 se ha relacionado con un conocimiento deficiente, con la falta de compromiso con las medidas de prevención y con creencias erróneas sobre el tema (Lee et al., 2020). Se ha observado un nivel alto de conocimiento sobre la enfermedad en los sanitarios y estudiantes de medicina y otras ciencias relacionadas con la salud (Khader et al., 2020; Maheshwari et al., 2020; Shi et al., 2020), aunque con resultados menos cohe-rentes que en otros estudios. Un grupo de estudiantes estadounidenses de secundaria mostraron conocimientos contradictorios sobre la enfermedad (Chesser et al., 2020), mientras que se describe a la población general en Arabia Saudí como poseedora de un alto nivel de alfabetización sobre la pandemia, asociado con actitudes optimistas, aunque los hombres mostraron un nivel menor de conocimientos y actitudes menos optimistas, así como unas prácticas menos beneficiosas para la salud que las mujeres (Al-Hanawi et al., 2020). También se ha descrito a la población de Nigeria como poseedora de un buen nivel de información sobre la COVID-19 derivado de fuentes formales de información sanitaria (Olapegba et al., 2020, en revisión). En Portugal se llevó a cabo un estudio sobre los conocimientos, las actitudes y los comportamientos de los adolescentes (Alves et al., 2021) sobre esta enfermedad. Los participantes exhibieron un nivel elevado de conocimientos pero se mostraron menos comprometidos con las medidas de prevención. Hasta donde sabemos, todavía no se han analizado los conocimientos de los adultos portugueses sobre la COVID-19. Sin embargo, teniendo en cuenta estudios anteriores, se espera que estos sean elevados, especialmente en el caso de las participantes mujeres con estudios.
La representación social organiza la información cognitiva sobre el nuevo asunto social (Abric, 1996) y, en el caso de la COVID-19, los valores y las creencias que interiorizamos durante este proceso podrían influir en nuestras actitudes frente a la enfermedad. Las actitudes se describen como una tendencia psicológica relativa a una entidad concreta, expresada a través de cierta disposición a favor o en contra (Eagly & Chaiken, 1993). Esta tendencia tiene una finalidad evaluativa y suele clasificarse en función de los tres tipos distintos de respuesta de las que se puede inferir (Ajzen, 1989): respuestas cognitivas, afectivas y conativas (conductuales).
Mientras que las respuestas cognitivas hacen referencia a las creencias sobre un objeto inanimado, las afectivas están más relacionadas con los sentimientos hacia dicho objeto. Las respuestas conativas muestran predisposiciones conductuales, intenciones o acciones respecto al objeto. Ajzen (1989) consideró la posibilidad de recabar respuestas tanto verbales como no verbales de los tres tipos. Si las representaciones sociales están más relacionadas con una composición dinámica de las creencias compartidas y construidas por un grupo, las actitudes representan la apropiación individual de un objeto social (Marková, 2017). Lo que se espera es observar una relación entre el contenido cognitivo de la representación social y las actitudes relativas a la COVID-19, puesto que ‘las actitudes relativas a un objeto de representación se basan en los componentes evaluativos de esa representación’ (Moliner & Tafani, 1997, p. 698). Por tanto, en este estudio esperamos identificar una actitud relacionada con la representación social de la COVID-19.
Dado el impacto de la pandemia de COVID-19 y los cambios en los comportamientos que esta ha causado en nuestras vidas, parece pertinente investigar el funcionamiento de la representación social, la actitud de la que surge esta representación y el grado de conocimiento sobre esta enfermedad infecciosa. Esta medida nos podría ayudar a entender cómo podemos adoptar comportamientos más saludables y de prevención, que probablemente serán necesarios en los próximos 12 a 24 meses hasta que se alcance la inmunidad de grupo o se consiga una vacuna totalmente eficaz (e.g., distanciamiento social, confinamientos profilácticos, etiqueta respiratoria, higiene de manos y desinfección de superficies).
Por tanto, el objetivo de este estudio era medir la estructura de la representación social de la COVID-19 y describir las actitudes y el nivel de conocimientos sobre la enfermedad de una muestra heterogénea de la población portuguesa, y formular nuevas preguntas para investigaciones posteriores que facilitarán la introducción de comportamientos preventivos frente al SARS-CoV-2 y a otras enfermedades infecciosas.
Método
Participantes
La muestra utilizada en este estudio fue reclutada entre la población portuguesa adulta con cierto nivel de estudios (mayores de 18 años), aplicando una técnica de muestreo no probabilístico (efecto ‘bola de nieve’).
En total se reclutaron 294 participantes, todos ellos de nacionalidad portuguesa, con una media de edad de 42 años (M = 42.54, DT = 12.32, Mediana = 40.0, Máx. = 78 años). El 85% de los participantes eran mujeres. Su distribución geográfica era: 23.5% del Algarve, 37.8% de la región de Lisboa y 10% de la región de Oporto. El resto de los participantes procedían del Alentejo y las regiones de Minho, Tras-os-Montes y las Azores (en porcentaje inferiores a 5%). Alrededor de un 66% de los participantes estaban casados y 60% declararon tener dependientes (M dependientes = 1.6, DT = 0.497). Por lo que respecta al nivel de estudios, 36.1% eran graduados o máster pos-Bolonia y 18.8% habían completado los estudios secundarios; el nivel de estudios, pues, oscilaba entre el segundo ciclo de enseñanza obligatoria (seis años de escolarización, 2.4%) y el doctorado (2.4%). La muestra podría definirse como de mediana edad, mujeres, con estudios, casadas y con dependientes.
Los participantes también tenían que indicar si conocían a alguien que se hubiese infectado de COVID-19, a lo que el 98% de los participantes respondieron negativamente. Se evaluó su percepción del riesgo de infección mediante las preguntas ‘¿Cuál estima que es la probabilidad de resultar infectado/a de COVID-19?’, a lo que respondieron sobre una escala de 1 (‘nada probable’) a 5 (‘muy probable’). Un 6.8% respondieron que era muy probable (5), 10.9% probable, 35.4% indecisos, 24.8% poco probable y 22.1 nada probable (1). Por lo general, los participantes no creían en la posibilidad de infectarse con COVID-19.
Medidas
La representación social de la COVID-19
Se aplicó la técnica de la evocación libre de palabras, considerando la expresión coronavirus/COVID-19 como el estímulo para la tarea. Los participantes tenían que escribir hasta cinco palabras o expresiones (no frases completas) que les sugiriese el concepto o la palabra presentada, siempre en el orden en que las evocaban. Para esta tarea se facilitaron cinco espacios visuales en los que podían introducir sus respuestas.
Actitud respecto a la COVID-19
A partir de la información facilitada por la DGS con datos oficiales actualizados sobre los avances científicos relacionados con la COVID-19, se elaboraron diversos ítems referidos a los componentes actitudinales sobre la enfermedad: componente cognitivo, componente afectivo/emocional y componente conductual (véase Apéndice A).
El componente relacionado con la cognición hace referencia a las creencias personales sobre la probabilidad de contraer COVID-19, el afecto personal, el conocimiento o comprensión sobre la enfermedad y la percepción personal sobre el riesgo de infección (un total de seis ítems).
El componente afectivo está relacionado con las emociones y los sentimientos causados por esta probabilidad de infección y por el afecto personal (seis ítems).
Por último, la dimensión conductual se ocupa de los comportamientos adoptados (o el cambio conductual discursivo) desde la aparición de la COVID-19 (ocho ítems en total).
Ajuste del modelo trifactorial de las actitudes respecto a la COVID-19
Nota: CFI — Índice de ajuste comparativo, TLI — Índice de Tucker-Lewis, RMSEA — Raíz del error cuadrático de aproximación; SRMR — Residuo cuadrático medio estandarizado.
Tras calcular la medidas de fiabilidad finales, la dimensión cognitiva presentó un alfa de Cronbach de .650, la dimensión afectiva de .888 y la conductual de .926, todos ellos valores considerados favorables a la elaboración de medidas compuestas.
Los valores más elevados en la dimensión cognitiva indican una mayor tendencia a creer que la COVID-19 representa un riesgo personal y social. Los valores más elevados en la dimensión afectiva sugieren un mayor sentimiento de ansiedad y miedo sobre la enfermedad, la preocupación sobre el riesgo individual y las posibles consecuencias de la infección. Por último, los valores elevados de la dimensión conductual indican mayor tendencia a cambiar o vigilar el propio comportamiento o estado de salud frente a la situación de pandemia.
Conocimientos sobre la COVID-19
Utilizando la información y las preguntas más frecuentes de la página web de la DGS, se elaboraron 10 enunciados sobre el agente viral responsable de la COVID-19, los medios de transmisión conocidos y el conocimiento de la vacuna, el tratamiento de la enfermedad y su prevención. Las posibles respuestas eran ‘verdadero’, ‘falso’ o ‘no lo sé’. A cada respuesta correcta se le asignó un punto, con una variación de repuestas correctas de 0 a 10. También se asignó un punto negativo a cada respuesta incorrecta, mientras que la respuesta ‘no lo sé’ no acarreaba ninguna puntuación, aunque se calculó el porcentaje de incertidumbre para cada pregunta. La puntuación global correspondiente al grado de conocimiento se determinó matemáticamente, sustrayendo las respuestas incorrectas de las correctas. Cuanto mayor era la puntuación global, mayor era el grado de conocimientos del participante.
Percepción del riesgo
Se incluyeron dos preguntas para medir la percepción del riesgo. Los participantes tenían que indicar la probabilidad de infectarse de COVID-19 de 1 (‘totalmente improbable’) a 7 (‘totalmente probable’) y responder si conocían a alguien infectado de COVID-19 (‘Sí’/‘No’).
Procedimiento de recolección de datos
Se contactó con los participantes a través de las redes sociales y se recabaron los datos mediante un cuestionario en línea. Se informó a todos los participantes sobre la finalidad del estudio. Para responder tenían que confirmar su consentimiento de participar voluntariamente en el estudio y se les aseguraba que no se les pediría información personal que les pudiese identificar o que produjese un nuevo contacto posterior.
Todos los datos recabados eran genéricos y no identificaban a los participantes, a quienes se garantizó total anonimidad y confidencialidad de las respuestas facilitadas. No se ofreció retribución alguna por su participación en el estudio, ni esta suponía riesgo alguno. Los participantes podían abandonar el estudio en cualquier momento cerrando la ventana del navegador en la que respondían al cuestionario.
Todos los datos fueron recabados después de que se introdujeran las medidas de confinamiento social, entre el 11 y el 26 de marzo de 2020.
Procedimiento de análisis de datos
Para definir la estructura de la representación social utilizamos el análisis prototípico de Vergès (1992), que asume el uso de palabras tanto ‘crudas’ o sin procesar, como categorizadas. Optamos por utilizar las formas sin procesar. En el análisis se tuvieron en cuenta la frecuencia y el orden de las evocaciones.
Los criterios para los análisis de las evocaciones fueron los siguientes: frecuencia mínima (la frecuencia mínima absoluta de las palabras que se incluyen en el análisis), frecuencia intermedia (la frecuencia absoluta que distingue a las palabras de alto nivel de ocurrencia de las de bajo nivel de ocurrencia), orden promedio de evocación (OME) mediante el cual se clasifica la evocación media de cada palabra y la media de los promedios de todas las evocaciones, un criterio que permite distinguir entre palabras de evocación primaria y palabras de evocación secundaria.
Es muy probable que las palabras de mayor frecuencia cuyo orden promedio de evocación es inferior a la media de todos los OME constituyan el núcleo central de la representación social. Por el contrario, las palabras menos evocadas, con una evocación media superior a la media de todos los OME probablemente constituyan el sistema periférico.
Los análisis prototípico y de semejanza (frecuencia de coocurrencias y prueba de asociación Chi cuadrado) se realizaron con el programa IRaMuTeQ.
Para el análisis de datos que nos permitiese establecer las relaciones entre representación social, actitudes frente a la COVID-19 y conocimientos, se recurrió a las correlaciones bivariadas entre la frecuencia de evocación, el conocimiento y las puntuaciones obtenidas en las dimensiones cognitiva, afectiva y conductuales de las actitudes frente a la enfermedad.
Todos los análisis se consideraron estadísticamente significativos, con un nivel de significatividad de 95%.
Resultados
Representación social COVID-19/coronavirus
Los 294 participantes efectuaron 1,362 evocaciones en las que utilizaron 231 palabras distintas. Las palabras evocadas por al menos 5% de la muestra se consideraron de frecuencia mínima, con un umbral de 15 ocurrencias. Este criterio redujo el corpus a 25 palabras distintas, es decir, una tasa de retención del 11%. Estas 25 palabras se correspondían con el 67% de todas las evocaciones efectuadas.
La frecuencia intermedia se estableció como la frecuencia media de todas las evocaciones (M = 39.36).
Los respectivos OEM se corresponden a la media ponderada de la frecuencia de las palabras en el orden en las que se han evocado. La media de los OEM se calculó a través de los OME de las palabras retenidas. En la Figura 1 se muestra la representación social de la COVID-19. Para este análisis se utilizó la técnica del análisis prototípico (o análisis de evocación) de Vergès (1992), incorporando también las sugerencias de Wachelke y Wolter (2011) y de Gomes y Nunes (2015). Representación social de la COVID-19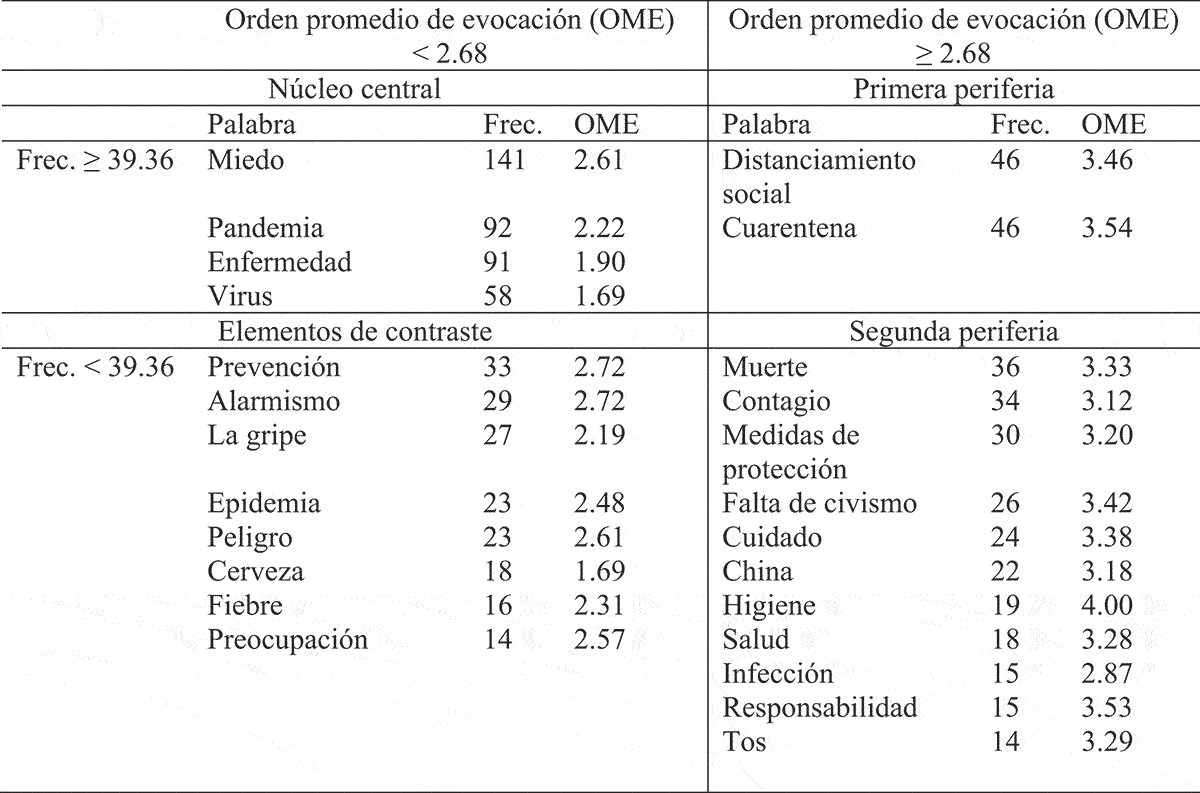
El área que ocupa el núcleo central incluye los términos miedo, pandemia, enfermedad y virus. Miedo es la palabra más frecuente. Describe una emoción vinculada a la COVID-19. El resto de las palabras del núcleo central contiene una descripción de la situación: pandemia, enfermedad y virus. La primera periferia incluye dos situaciones posibles que implican aislamiento: cuarentena y distanciamiento social. Entre los elementos de contraste observamos conceptos utilizados para el anclaje: gripe, cerveza (en referencia a la marca de cerveza Corona) y palabras relacionadas con la caracterización de la enfermedad: peligro, epidemia y fiebre. Por último, en la segunda periferia, más externa, se identifican diversas perspectivas o posiciones sobre la COVID-19.
El análisis de semejanza (Figura 2) permite establecer las concurrencias entre las palabras evocadas. Resultados del análisis de proximidad léxica (coocurrencia) realizado mediante la tarea de asociación libre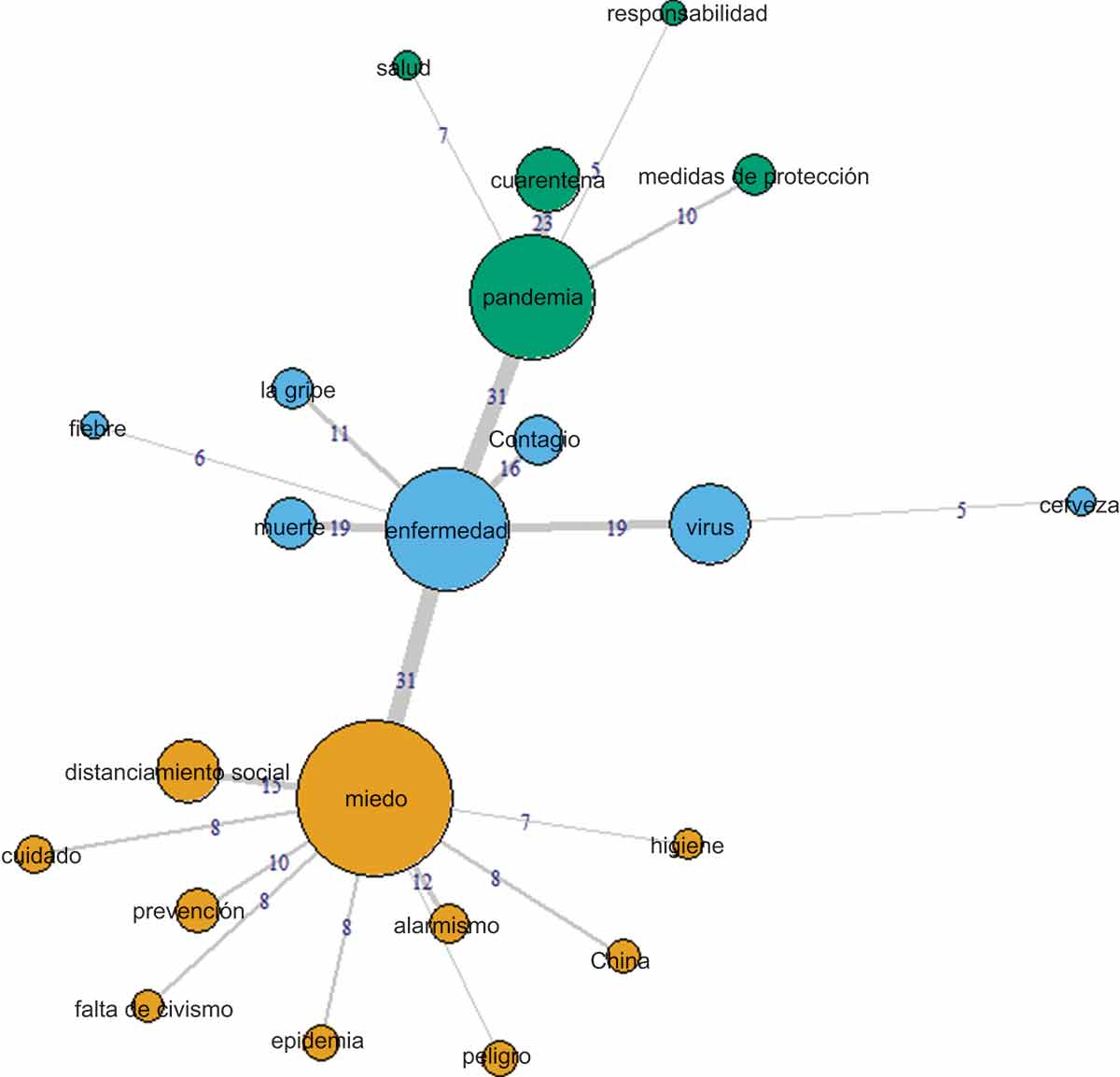
Las palabras miedo, pandemia y enfermedad — todos ellos conceptos del núcleo central — parecen organizar las evocaciones en tres ramificaciones o comunidades. Miedo coocurre principalmente con el distanciamiento social, pero también lo hace con el alarmismo y la prevención. Miedo se vincula con enfermedad pero no con pandemia.
Enfermedad presenta la coocurrencia más alta con virus y muerte, seguida de contagio y gripe. También presenta una coocurrencia elevada con pandemia.
Pandemia presenta mayor proximidad con cuarentena, seguida de las medidas de protección. Estas asociaciones también fueron sometidas a la prueba de Chi cuadrado (Figura 3). Resultados de las relaciones entre evocaciones (test de Chi cuadrado)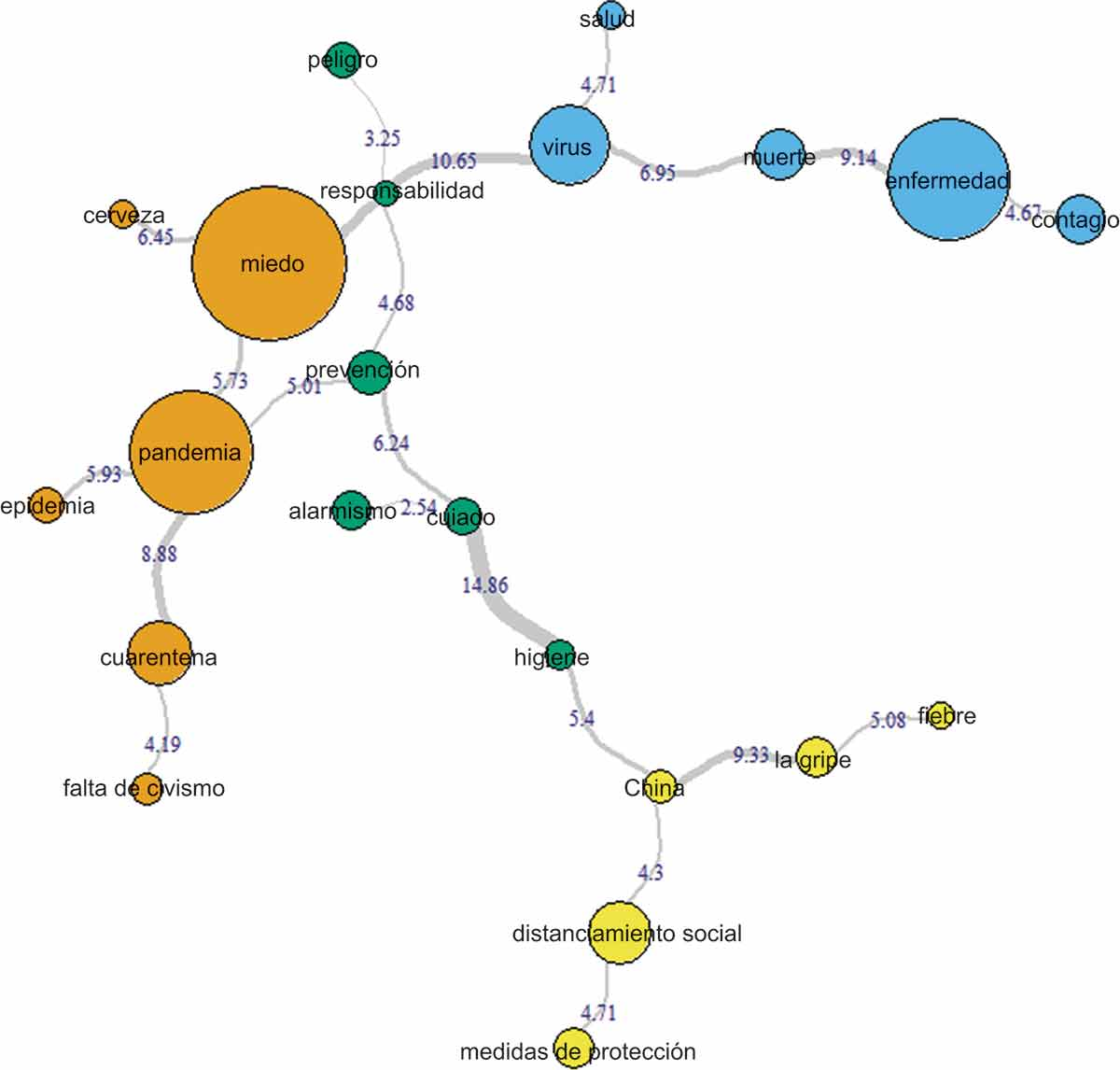
Todos los valores se consideraron estadísticamente significativos para valores de Chi cuadrado superiores a 3.841 (nivel de confianza de 95%; n/F = 1).
Las asociaciones más fuertes observadas eran: cuidado e higiene, miedo y virus, enfermedad y muerte, China y gripe y entre pandemia y cuarentena. Todas las evocaciones parecen estar asociadas significativamente entre ellas, excepto peligro y responsabilidad y alarmismo y cuidado.
Componentes actitudinales frente a la COVID-19
Correlaciones de Pearson entre las dimensiones actitudinales cognitiva, afectiva y conductual frente a la COVID-19
El nivel de conocimientos frente a la COVID-19
Índice de respuestas correctas y falta de conocimientos sobre la COVID-19
Evaluamos la exactitud de los conocimientos de los participantes mediante el diferencial entre las respuestas correctas y las incorrectas. Con un mínimo de −2.00 y un máximo de 10, la media del nivel de conocimientos era de 5.53 (DT = 2.528). El conocimiento no se veía afectado por la edad del participante (p = .466) o su nivel de estudios (p = .333).
Relaciones entre representación social, nivel de conocimientos y actitudes frente a la COVID-19
Correlaciones de Pearson entre conocimientos y actitudes frente a la COVID-19
Nota: *p < .05, **p < .01, ***p < .001.
Se observó una fuerte correlación positiva entre las respuestas correctas y las incorrectas, lo que muestra que responder de manera correcta a las preguntas también implica dar más respuestas incorrectas.
No obstante, también se observó una correlación negativa entre las respuestas correctas y la falta de conocimientos. Este resultado sugiere mayor exactitud de conocimientos entre los participantes menos predispuestos a indicar su desconocimiento de la información sobre la que se les preguntaba. Por el contrario, se observó una correlación entre los errores y la incertidumbre, aunque bastante débil. Por tanto, podemos afirmar que la exactitud no depende necesariamente del nivel de conocimientos.
Correlaciones de Pearson entre la representación de la COVID-19, los conocimientos y las actitudes frente a la enfermedad
Nota: *p < .05, **p < .01, ***p < .001.
Los resultados revelan también una relación positiva entre la dimensión afectiva frente a la COVID-19 y la prevalencia del miedo y el peligro en la representación social. El miedo, en particular, era uno de los conceptos integrantes del núcleo central. Las puntuaciones altas en las dimensiones afectiva y conductual de las actitudes frente a la COVID-19 parecían estar relacionadas con la ausencia de referencias a la gripe y la cerveza.
Por lo que respecta a los conocimientos, los participantes con más respuestas incorrectas mostraron los niveles más bajos de preocupación y descortesía en sus representaciones sociales de la COVID-19; los que anotaron más respuestas correctas parecían evocar mayor distancia social.
Discusión
El objetivo del estudio era medir la representación social de la COVID-19, caracterizar las actitudes y el conocimiento sobre el virus SARS-CoV-2 y la enfermedad infecciosa responsable de la actual pandemia con importantes consecuencias físicas, mentales, sociales y económicas a escala global.
Se describe la representación social desde la perspectiva de la Teoría del núcleo central de Abric (1993) y se aplica el análisis prototípico de Vergès (1992). Los resultados revelan que la representación social retiene el 67% del total de evocaciones efectuadas, con un total de 25 palabras en los análisis. No se efectuó una categorización de las evocaciones, sino que optamos por un análisis más conservador. No obstante, la proximidad entre algunas palabras sugiere que se podría haber obtenido una representación más parsimoniosa si se hubiesen agrupado las palabras en función de su semejanza léxica.
Como cabía esperar, la observación general de la representación social de la COVID-19 revela una caracterización negativa del fenómeno. Se trata de una nueva amenaza que impone ciertas exigencias y grandes implicaciones para las personas y los participantes podrían albergar sentimientos negativos hacia ella. Y la palabra más evocada es precisamente una emoción — el miedo — que representa un sentimiento común y compartido sobre la posibilidad de contagio. El núcleo central también incluye conceptos relativos a los elementos centrales de la situación: pandemia, enfermedad y virus. La construcción de la representación social parece depender de sus características: se trata de una enfermedad producida por un virus que ha provocado una pandemia.
Estudios previos sobre las enfermedades infecciosas revelan representaciones sociales similares, con el miedo como un aspecto central. La representación social del ébola en España (Idoiaga et al., 2017) y en el Reino Unido (Joffe & Haarhoff, 2002) mostró la presencia del miedo, aunque sin el sentimiento de amenaza personal. Washer (2004) mostró también el miedo como un vestigio en la representación social del SARS, aunque contenía un mecanismo por el que se diferenciaba a quienes estaban en situación de riesgo (otros) de quienes no lo estaban (yo, nosotros). Colì et al. (2020) realizaron estudio similar en el que una muestra de población adulta italiana completó una tarea de asociación libre. La representación social incluía contagio, miedo y pandemia en el sistema del núcleo central. En este estudio se identificó también cierta semejanza con otras epidemias infecciosas causadas por virus. Sin embargo, no se identificó un mecanismo de alterización en la representación. El riesgo o la amenaza personal parece estar implícito en esta representación. Asimismo, nuestros resultados revelan una reproducción del discurso mediático sobre la COVID-19 que influye en la formación de la representación social, en el comportamiento preventivo y en la gestión del miedo.
La representación social observada en este estudio presenta valores como responsabilidad, medidas de protección, prevención, distanciamiento social e higiene, que sugieren un sentimiento de amenaza personal y de responsabilidad individual.
Y aun así, deberíamos tener en cuenta que China está presente en las evocaciones, asociada al miedo. Existe también un vínculo con la gripe. De Rosa y Mannarini (2020) sostenían que el impacto global de la COVID-19 incrementa la conciencia de la vulnerabilidad humana y dibuja a la humanidad como el endogrupo. Esto podría incrementar la concienciación de que todos nos encontramos en una situación de riesgo. Por tanto, la asociación anterior (China y miedo) podría interpretarse como la confianza en el origen del virus y no en un mecanismo de alterización.
No obstante, el vínculo establecido con la gripe podría ser un efecto del discurso mediático sobre la COVID-19 como ‘gripe china’, que respalda la idea de que ‘otros’ (China) son responsables de la situación. Páez y Pérez (2020) reflexionaron sobre este tema y demostraron que el anclaje de la enfermedad a un exogrupo es un proceso habitual en la representación de una epidemia. Como afirman los autores, estos exogrupos se consideran antihigiénicos o autores de prácticas antihigiénicas. Este razonamiento parece haberse aplicado al caso de la COVID-19 en una representación mediática xenófoba pero ampliamente difundida, como indica la etiqueta conferida por el Presidente estadounidense Donal Trump en sus referencias al ‘virus chino’ o ‘gripe china’. Esta representación mediática podría haber bastado para que el público general asociase prácticas antihigiénicas con la población china, incrementando así su estigmatización y su diferenciación respecto a las sociedades occidentales. De hecho, en nuestro estudio, China también se asocia con el concepto de higiene, mostrando una posible denigración de los ciudadanos chinos en esta situación. La población portuguesa podría culpar a China o a la población china por la pandemia debido a fenómenos culturales como la venta generalizada de animales silvestres (en los llamados ‘mercados húmedos’ o de animales vivos) y las prácticas de higiene.
En Portugal, el discurso mediático se ha centrado menos en la estigmatización de un exogrupo para enfocarse en el ‘estado de guerra’, utilizado constantemente para hacer alusión al virus. El ‘insidioso enemigo’ y la ‘batalla que todos y cada uno de nosotros tenemos que librar’ son expresiones utilizadas por ministros del Gobierno y por el Presidente. Estos aspectos han incrementado el sentimiento personal de riesgo y las implicaciones conductuales para detener o limitar la pandemia de COVID-19.
En respuesta a la COVID-19, Portugal, como otros países, recurrió al confinamiento obligatorio, el distanciamiento social, la higiene personal y el uso de mascarillas para controlar la transmisión de la infección entre la población. Las palabras de la primera periferia parecen reflejar esta situación. Esta categoría incluye únicamente dos palabras: cuarentena y distanciamiento social. Asimismo, uno de los requisitos de los virus de transmisión aérea es el aislamiento de los infectados (cuarentena) y el distanciamiento social para prevenir la infección. Sin embargo, mientas que la cuarentena ocurre de un modo simultáneo a la pandemia, el distanciamiento social es concurrente con el miedo, lo que sugiere que las personas podrían tener una impresión afectiva negativa de estas medidas. El miedo también está asociado al alarmismo, que podría interpretarse como un intento de disminuir la percepción de riesgo de la situación. Este tipo de comunicación hacia un enemigo, con referencias bélicas, se ha debatido en la literatura como un obstáculo que dificulta los aspectos cognitivos y emocionales de la cooperación y el cuidado de los demás (Sabucedo et al., 2020).
Aunque la búsqueda de comportamientos de prevención del riesgo como reacción al miedo podría interpretarse como intuitiva, diversos estudios sobre los comportamientos preventivos no identifican esta asociación de manera obvia. Ruiter et al. (2001) sugirieron que el miedo es menos motivador que la percepción de la efectividad de la acción y la autoeficacia de los individuos en su gestión ante las amenazas. La relevancia personal percibida podría ser crítica también para el impacto emocional percibido de la información disponible sobre la amenaza. Lench y Levine (2005) sugerían que el miedo podría disminuir las creencias optimistas poco realistas. Sin embargo, cuanto mayor era el miedo señalado por los participantes, menor era el control que percibían tener sobre los resultados y la memoria del propio riesgo, lo que se traduce en una disminución de los comportamientos de prevención. Kok et al. (2018) señalaron que el papel del miedo podría ser más perjudicial que beneficioso en la adopción de comportamientos saludables o de evitación de la amenaza y que las personas podrían ser dependientes de su autoeficacia percibida para afrontar dicha amenaza.
Joffe (2003) sugirió que los textos y las imágenes se procesan a través de representaciones prexistentes. El anclaje con la gripe podría condicionar cómo procesamos la información disponible sobre la enfermedad, disminuyendo la percepción del riesgo. De hecho, la mayoría de nuestros participantes expresaron la improbabilidad de infectarse con el virus, a pesar del incremento en el número de infecciones. Asimismo, se esperaba que las dinámicas cambien y que el miedo, como reacción emocional, disminuya (Mayor et al., 2012), lo que podría dar a las personas una perspectiva ilusoria de seguridad y llevarlos a abandonar las medidas preventivas o, al menos, sentir que estas podrían chocar con los valores democráticos de libertad de expresión y acción.
Sin embargo, esta representación parece dar servicio a un sentido de afrontamiento simbólico colectivo (Páez & Pérez, 2020). Incluye información sobre los métodos de control de la infección (higiene, distancia social, medidas de protección), información clara sobre los síntomas (fiebre) y también un anclaje a la gripe conocida, así como un vínculo con China (primer brote conocido de la enfermedad). Anclar esta enfermedad letal y desconocida a otros conceptos conocidos como la gripe tiene la función representativa de normalizar la situación y hacerla más familiar (Moscovici, 1976), al mismo tiempo que facilita información útil sobre cómo gestionarla y cómo hacer los cambios conductuales necesarios en términos de protección. No obstante, la información en torno a la manifestación del virus y el comportamiento sigue cambiando y se espera que ocurra una transformación de esta representación social.
Los participantes parecen estar bien informados sobre las medidas preventivas y la identificación de los síntomas de la infección. Del total de participantes, el 93.5% sabían que este virus no afecta únicamente a los ancianos, 89.1% de ellos sabían que no deberían acudir a los centros de asistencia primaria si tenían síntomas de la infección y sabían también que la tos y la fiebre eran los síntomas que había que tener en cuenta. Sin embargo, casi la mitad de la muestra creía que el virus causante de la COVID-19 es idéntico al virus de la gripe y más de un 60% cree que el origen del virus está sólidamente establecido. Nuestros participantes parecen poseer unos conocimientos más bien contradictorios.
Nuestros resultados parecen corroborar los obtenidos por Chesser et al. (2020), que identificaron conocimientos contradictorios sobre la COVID-19 entre estudiantes universitarios. Los estudios existentes sobre el conocimiento y las actitudes en torno a la COVID-19 (Gupta et al., 2020; Khader et al., 2020; Shi et al., 2020) demuestran que las muestras utilizadas — educadas y vinculadas al ámbito de la salud — tenían un alto nivel de conocimientos, aunque podrían presentar algún déficit respecto a la medidas avanzadas de prevención (Khader et al., 2020). Desde una perspectiva funcional, la muestra del estudio tiene un alto nivel de conocimientos sobre las medidas de higiene, los síntomas y los procedimientos necesarios en caso de infección. Sin embargo, parecen albergar una serie de creencias erróneas sobre la infección y en particular sobre el origen del virus (en el momento de realizar las medidas), la semejanza o diferencias con la gripe, el tratamiento de la enfermedad y las vías de transmisión. Por tanto, el nivel de conocimientos parece ser menor que el de los grupos relacionados con la salud. No obstante, el nivel es más elevado en las dimensiones más relevantes relacionadas con la protección personal.
Esta falta de consistencia, aunque esperada, refuerza el uso de la representación social para gestionar la información disponible sobre el riesgo. A diferencia de otras pandemias, la de COVID-19 se ha caracterizado por un flujo constante de información en diversas plataformas mediáticas. Hay información disponible y está ampliamente difundida. Más que considerar que las personas interpretan mal la información o la procesan mal, deberíamos considerar la hipótesis de que la representación social está condicionando cómo reaccionan las personas a la COVID-19 y construyen su representación de estar exentos de riesgo. Como concluía Joffe (2003) en su revisión, la teoría de la representación social contribuye a la teoría del riesgo con un ‘posicionamiento sobre cómo el “nosotros” se incorpora y contribuye a la construcción del “yo”’ (p. 68).
También parece haber una relación entre el conocimiento exhibido y el perfil de la evocación individual, Los individuos que responden con mayor frecuencia ‘no lo sé’ tienden también a evocar la palabra alarmismo con mayor frecuencia. Los participantes que obtienen mayor número de respuestas incorrectas tienden a evocar con menor frecuencia las palabras preocupación e incivismo, mientras que aquellos con mayor número de respuestas correctas evocan distancia social con mayor frecuencia. Estos resultados sugieren que un nivel más bajo de conocimientos sobre la COVID-19 podría resultar en una apropiación de la representación social que depende de elementos periféricos para ajustar la experiencia personal y aumentar el riesgo. Estos resultados son de particular interés si consideramos esta pandemia como una infodemia (Cinelli et al., 2020). La desinformación en torno a la COVID-19 se ha asociado con la falta de conocimientos, la falta de compromiso con las medidas de prevención y creencias erróneas sobre la enfermedad (Lee et al., 2020).
Por lo que respecta a las actitudes, los resultados sugieren que los participantes no creen que vayan a infectarse y ni siquiera se muestran preocupados por esta posibilidad. Se observó una preocupación ligeramente mayor sobre los cambios observados en el comportamiento.
Esperábamos observar una relación entre el contenido de la representación social de la COVID-19 y las actitudes medidas. Sin embargo, esta relación no está clara ni bien establecida. Las correlaciones observadas son débiles y apenas indican la posibilidad de alguna asociación entre las evocaciones y la evaluación de la enfermedad.
Los participantes con un nivel elevado en la dimensión afectiva de las actitudes parecen evocar con mayor frecuencia miedo y peligro, y en menor medida gripe y cerveza. Los que evocan peligro parecen más predispuestos a modificar su comportamiento para protegerse. La evocación de la gripe está relacionada con una postura menos preocupada y menor predisposición a modificar el comportamiento (e.g., un lavado de manos más frecuente). La evocación de la cerveza — en alusión a la marca de cerveza Corona — está inversamente relacionada con las dimensiones afectiva y conductual, y con una actitud más permeable frente a la COVID-19.
Cabe destacar también que el número de respuestas ‘no lo sé’ estaba inversamente relacionado con la dimensión conductual. Quienes respondían de este modo con mayor frecuencia parecen menos predispuestos a modificar su comportamiento y son también quienes evocan en mayor medida la palabra alarmismo.
No se corrobora la relación anticipada entre la representación social y las actitudes. Esperábamos que las representaciones sociales condicionasen las actitudes frente a la COVID-19, puesto que las actitudes hacia un objeto se basan en los componentes de su representación social (Moliner & Tafani, 1997). Sin embargo, hay que tener en cuenta que la principal contribución de las representaciones sociales se basa, precisamente, en el proceso dinámico de su formación. Entender la representación social desde el punto de vista estático de la organización cognitiva es ignorar la riqueza de información que ofrece sobre el modo de aprehender el mundo y el proceso de deconstrucción del objeto para la creación del sentido común (Joffe, 2003).
A pesar de no ser lineal, la representación social de la COVID-19 podría revelar la emergencia de dos grupos. En conjunto, ambos forman distintas representaciones que contribuyen a su autoidentidad. Hay un grupo que tiene una actitud menos favorable respecto a la COVID-19 con una preocupación mayor sobre la enfermedad y mayor intención conductual de adoptar comportamientos compatibles con la protección personal (lavado de manos, etiqueta respiratoria y distanciamiento social). Este grupo parece tener una representación en torno a miedo, protección, distanciamiento social y comportamiento cívico. Por otra parte, parece haber otro grupo con una actitud más positiva hacia la enfermedad, con menor nivel de preocupación o ansiedad y menos intención de cambiar su comportamiento. Este segundo grupo está más orientado a incluir las palabras alarmismo, cerveza y gripe y presentan niveles más altos de respuestas de tipo ‘no lo sé’ (sobre su conocimiento).
Futuros estudios
El estudio se realizó en los primeros estadios de la pandemia de COVID-19, mientras se estaba formando la representación social. Mayor et al. (2012) mostraron cómo los patrones en la representación social cambian a lo largo de la situación de pandemia. La representación social identificada en este estudio presenta diversos elementos de un primer contacto con la amenaza (un exogrupo responsable, clasificación de los síntomas, maneras de disminuir el riesgo de infección). Con la expansión de la infección, es probable que más personas lleguen a infectarse o conozcan a personas que han se hayan infectado o incluso lleguen a sufrir las consecuencias de la pandemia. El conocimiento sobre la COVID-19 aumenta con rapidez y sigue difundiéndose entre las personas legas. Por tanto, se anticipa una evolución de la representación social que debería ser estudiada, puesto que parece contribuir a la explicación de la complejidad de los comportamientos individuales frente a la pandemia de COVID-19.
Footnotes
National funding through FCT — Fundação para a Ciência e a Tecnologia (Portuguese national funding agency for science, research and technology) as part of the project CIP/UAL — UID/PSI/04345/2019. / Se obtuvo financiación nacional a través de la FCT — Fundação para a Ciência e a Tecnologia (Agencia nacional portuguesa para la financiación de las ciencias, la investigación y la tecnología) como parte del proyecto CIP/UAL — UID/PSI/04345/2019.
Both authors were responsible for designing, collecting and analysing all data. Alexandra Gomes was responsible for writing the final document. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Due to online data collection, participants gave their consent in the questionnaire. The front page informed participants of the objective, andtheir rights and specifically asked if they wanted to participate in the study voluntarily. If so, they chose to continue. If not, they decided to finish the questionnaire. No data were collected before the consent to participate. / Ambas autoras son responsables del diseño, recolección y análisis de los datos. Alexandra Gomes es responsable de la redacción del documento final. Todos los procedimientos con participantes humanos se realizaron de acuerdo con los estándares éticos del Comité ético de investigación y con la Declaración de Helsinki y sus modificaciones posteriores u otros estándares comparables. Dado que la recolección de datos se realizó en línea, los participantes confirmaron su consentimiento informado en el cuestionario. En la página inicial se facilitó información sobre el objetivo del estudio y los derechos de los participantes y se les preguntó explícitamente si aceptaban participar voluntariamente en el estudio. En caso afirmativo, seleccionaban continuar con el estudio. En caso contrario, podían optar por finalizar el cuestionario. No se recabó ningún dato antes de obtener el consentimiento del participante.
No potential conflict of interest was reported by the authors. / Los autores no han referido ningún potencial conflicto de interés en relación con este artículo.
Appendix A
Attitudes towards COVID-19
Cognitive
I believe I am at the same risk of contracting COVID-19 as the rest of the population.
Anyone can avoid infection if they are careful enough.
I believe COVID-19 is as dangerous as any other viral infection, such as the flu or a common cold.
COVID-19 is a viral infection that should raise more concern than other common infections.
Infection can hardly be avoided, even with prevention measures.
My health risks are unaltered, even with the dissemination of COVID-19 infection.
Affective
I am afraid of being infected with COVID-19.
I feel that I am more anxious since the first cases were detected.
I am paying more attention to my general health state.
I am more concerned over the possibility of becoming ill.
I am not worried about the evolution of the COVID-19 pandemic situation.
I am not afraid of infection by COVID-19.
Behavioural
I tend to wash my hands more since COVID-19 was detected.
I monitor my health condition.
I avoid personal, direct contact with strangers.
I continue to maintain the same level of intimacy with my family.
I reduced contact with my close friends.
I screen for symptoms of a viral illness on those around me.
I avoid public spaces such as malls, supermarkets, etc.
I intend to change my behaviour if cases are detected near me.
Actitudes frente a la COVID-19
Cognitivas
Creo que tengo el mismo riesgo de contagiarme de COVID-19 que el resto de la población.
Cualquier persona puede evitar la infección si tiene el cuidado suficiente.
Creo que la COVID-19 es tan peligrosa como cualquier otra infección viral como la gripe o el resfriado común.
La COVID-19 es una infección viral que debería preocuparnos más que otras infecciones comunes.
Es muy difícil evitar la infección, incluso tomando las medidas de prevención.
Los riesgos para mi salud siguen siendo los mismos, incluso con la difusión de la infección de COVID-19.
Afectivas
Tengo miedo de contraer la infección de COVID-19.
Creo que estoy más preocupado/a desde que se detectaron los primeros casos.
Estoy prestando más atención a mi estado general de salud.
Estoy más preocupado/s por la posibilidad de caer enfermo/a.
No me preocupa la evolución de la pandemia de COVID-19.
No tengo miedo de contraer la infección de COVID-19.
Conductuales
Me lavo las manos con mayor frecuencia desde que se detectó la COVID-19.
Vigilo mi estado de salud.
Evito el contacto personal directo con extraños.
Sigo manteniendo el mismo nivel de intimidad con mi familia.
He reducido el contacto con mis amigos más cercanos.
Intento detectar síntomas de una infección viral en las personas que me rodean.
Evito espacios públicos como grandes centros comerciales, supermercados, etc.
Trato de modificar mi comportamiento si se detectan casos en mi entorno.