
Abstract
The objectives of the present paper were to determine the rate and factors associated with seeking readmission among the clients admitted to an inpatient medical withdrawal management program, Vancouver Detox (VD). All clients who were admitted to VD between July 1, 2003, and June 30, 2004, were included in the study, and were followed up for 1 year. Multinomial logistic regression was performed to investigate the potential risk factors associated with short-term (1 month) and long-term (2 to 12 months) requests for readmission simultaneously. The risk factor associated with short-term request for readmission was leaving VD against medical advice (AMA) during the index admission. Clients who reported to have hepatitis C virus (HCV) infection, whose primary preferred substance was alcohol, and those who were poly-drug users were more likely to request readmission in long-term. Clients with no fixed address were less likely to seek readmission between months 2 and 12.
Introduction
Detoxification is the safe management of physical withdrawal symptoms from a substance of misuse or dependence so that the associated risks are minimized. Generally, detoxification is considered as the beginning phase of treatment, and offering it alone, without follow-up to an appropriate level of care, is considered to be of little long-term value and an inadequate use of limited resources (1). However, detoxification improves the overall health and well-being of many substance dependent individuals. It is also invaluable as a gateway to more extensive services and interventions (1).
When detoxification is not followed by further addiction treatment, it is very likely that clients will need detoxification again (2). Several studies have attempted to identify correlates of readmission, to determine whether there are specific populations at risk of readmission that could be targeted early in the treatment process, and to reduce the likelihood of readmission. Findings from these studies have shown that older age (2, 3), being male (2), lack of stable housing (3, 4), alcohol as a primary drug of choice (3), ploy-drug use (3), treatment incompletion at baseline (3), and lack of follow-up treatment (2) are associated with an increased risk of detoxification readmission.
By the nature of the factors associated with readmission, their impacts on the risk of readmission may differ over time. For instance, it is reasonable to hypothesize that the impact of treatment incompletion is higher on a short-term readmission than on a long-term readmission. However, to out knowledge, there are no such studies (2, 3, 5) that investigate risk factors associated with short-term and long-term readmission separately. Instead, the effects of the factors on the risk of readmission in the previous studies (2, 3) were assumed to be constant over time due to the use of Cox proportional hazards model.
It is also known that the majority of detoxification services require waiting time, ranging from several days to several weeks, and over 30% of clients may drop out while waiting for treatment (6–9). These previous studies on readmission are not able to capture clients who request readmission but drop out before engaging in the treatment. This does not mean that these clients do not need treatment. Instead, it may imply that either they may use alternative health care resources, such as emergency departments, or hospitals, or they are unable to overcome systemic barriers to readmission. Therefore focusing on readmitted clients might not allow a full description of characteristics of people who relapse after detoxification treatment and might underestimate the relapse rate.
In addition, we have previously shown that some specific groups such as male, aboriginal people, people without a fixed address, and people on methadone maintenance treatment (MMT), are more likely to drop out before engaging in treatment (8). Those factors may be also associated with clients’ request for readmission. Therefore, focusing on readmitted clients might also bias the estimated impact of the factors on relapse in either direction.
In the present study we investigate this issue from a different perspective. Instead of examining people who are actually readmitted to the detoxification service, we focus on people who request the service again after being discharged. The objective of the present study is to investigate the factors that are associated with time-dependent requests for readmission to an inpatient medical withdrawal management program.
Methods
Study Design
All clients who were admitted to Vancouver Detox (VD) between July 1, 2003, and June 30, 2004, were included in the study.
The first admission of the selected clients was defined as index admission. In order to avoid including censored cases, each individual was followed-up for one year and the first referral to VD after being discharged from the index admission was used for the analyses. Ethical approval for the study was granted by the Behavioural Research Ethics Board at the University of British Columbia.
From our preliminary data analysis, we found that request-for-readmission patterns were different over time, especially between the first follow-up month and the other 11 months, which implied that some of risk factors associated with short-term and long-term requests for readmissions might be different. To explore potential risk factors associated with seeking readmission over short-term and long-term, we classified clients into three groups: no request group—if clients did not seek readmission to VD during the 1-year follow-up; short-term readmission request group—if clients requested readmission to VD within 1 month after being discharged from the index admission; and long-term readmission request group—if clients requested readmission to VD between 2 and 12 months after being discharged from the index admission.
Treatment Setting
VD offers a medically managed 24-bed mixed-gender inpatient withdrawal management treatment in Vancouver, British Columbia. The detailed description of treatment setting can be found elsewhere (9). In brief, VD is staffed by a multidisciplinary team. It provides 24-hour nursing staff, onsite medical assessment and treatment, medical management of withdrawal symptoms, and other identified health concerns. The entry point to VD is by ACCESS 1, a central telephone intake service. After an initial telephone screening, ACCESS 1 determines whether the client is eligible for the service. If the client meets the criteria for VD, he/she is either admitted to VD immediately or placed on a waitlist for a bed to become available. Once admitted, the clinical staff completes a comprehensive assessment and develops an individualized treatment plan. Clients admitted on methadone maintenance are maintained on this medication throughout the admission. Clients are either discharged by successfully completing the program or voluntarily dropping out by terminating against medical advice (AMA). Upon discharge clients are referred to other services if required.
Data Collection
During the initial phone interview, ACCESS 1 staff collects basic information such as age, gender, address, and conduct a brief addiction assessment using a Vancouver Coastal Health Authority online, real-time system, Primary Access Regional Information System (PARIS) database. Once a client is admitted to the VD, the clinical staff verifies the information inputted by ACCESS 1 and completes a more comprehensive assessment, which is entered into the database. During the admission, the VD staff updates the clinical information in PARIS until the client is discharged.
The PARIS database is comprehensive and includes many variables. For the purpose of this study, the following variables were extracted: clients’ unique identification (PARIS number), demographic information (age, gender, ethnicity, parenting status), housing information (no fixed address [NFA] versus others), system characteristics (referral, admission, and discharge dates), substance use disorder-related information (substances recently used, primary preferred substance(s), discharge reason, if on existing methadone maintenance treatment (MMT), and preexisting injection drug use [IDU]-related diagnoses such as hepatitis C [HCV] or human immunodeficiency virus [HIV] infection).
Participants
Descriptive Characteristics of Study Sample (N = 1102)
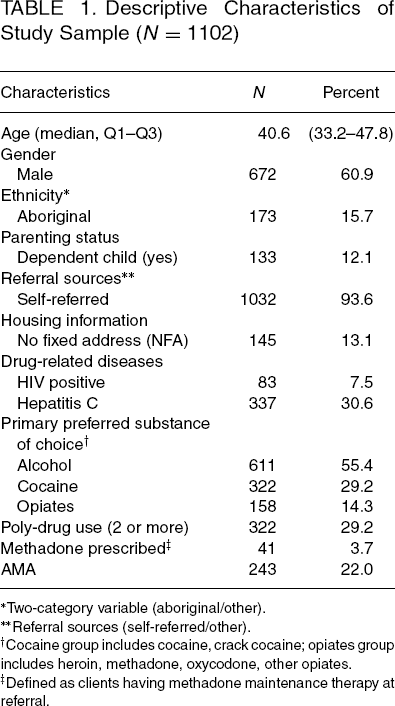
Two-category variable (aboriginal/other).
Referral sources (self-referred/other).
Cocaine group includes cocaine, crack cocaine; opiates group includes heroin, methadone, oxycodone, other opiates.
Defined as clients having methadone maintenance therapy at referral.
Statistical Analysis
Contingency table analysis (the chi-square test or the Fisher's exact test) and the Kruskal-Wallis test were used for bivariate comparisons of categorical and continuous variables, respectively.
Instead of using the Cox proportional hazard regression model (2, 3, 5), a multinomial logistic regression model was employed to examine the risk factors associated with requests for readmission to VD. This was due to the following reason. Our preliminary data analyses results implied that the impacts of some factors on the risk of readmission might vary over time. As a result, the assumption of Cox proportional hazards model that the effects of explanatory variables on the risk of an event were constant over time was not met. On the other hand, although a logistic regression model could be used in the present study, this would not allow exploration of the possibility of distinguishing short-term and long-term risk factors simultaneously.
The outcome variable was polychotomous with three categories: if clients were in no request group, the outcome was zero; if clients were in short-term readmission request group, the outcome was 1; if clients were in long-term readmission request group, the outcome was 2. The reference category was no request group. The variables that were strongly bivariately associated (P value <.25) with readmission or were clinically significant were then included in the multinomial logistic regression model to identify the prognostic factors for requests for readmission. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed. All statistical analyses were performed using SAS 9.1 software program (SAS Institute, Cary, NC).
Results
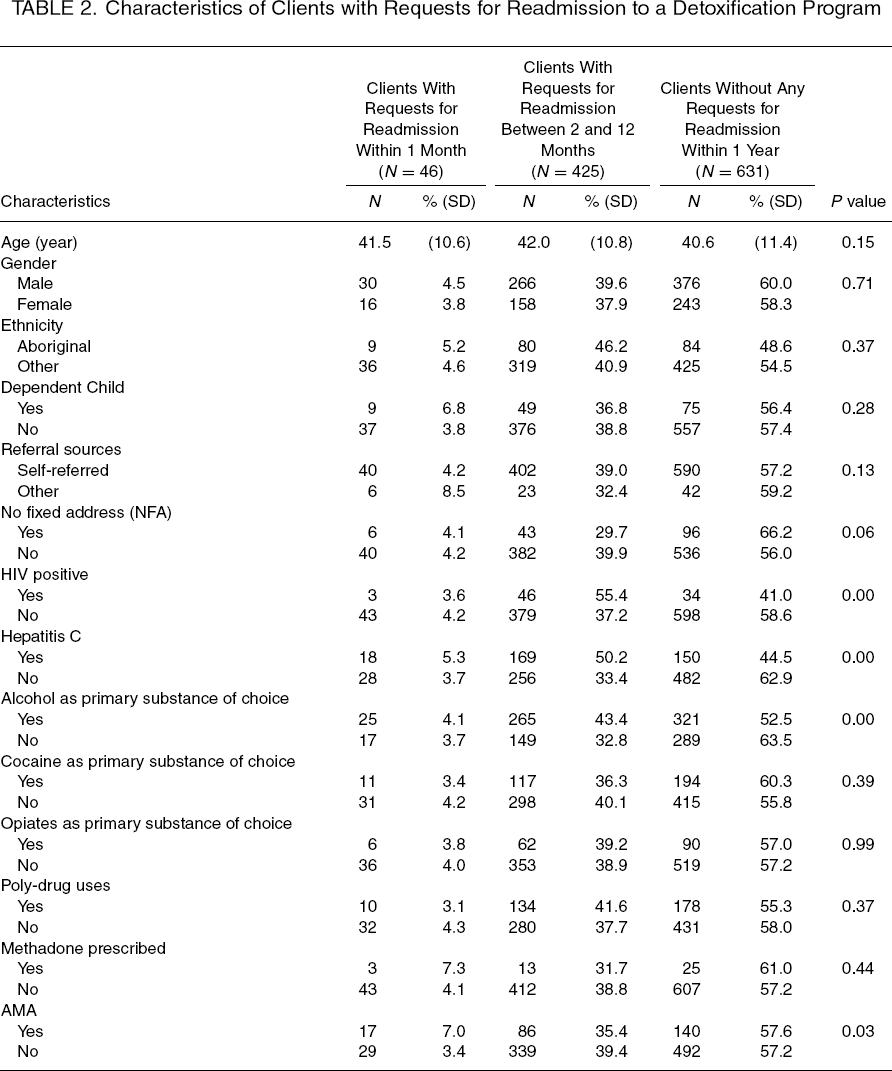
Characteristics of Clients with Requests for Readmission to a Detoxification Program
Multinomial Logistic Regression Model of Variables Associated with Requests for Readmission to a Detoxification Program
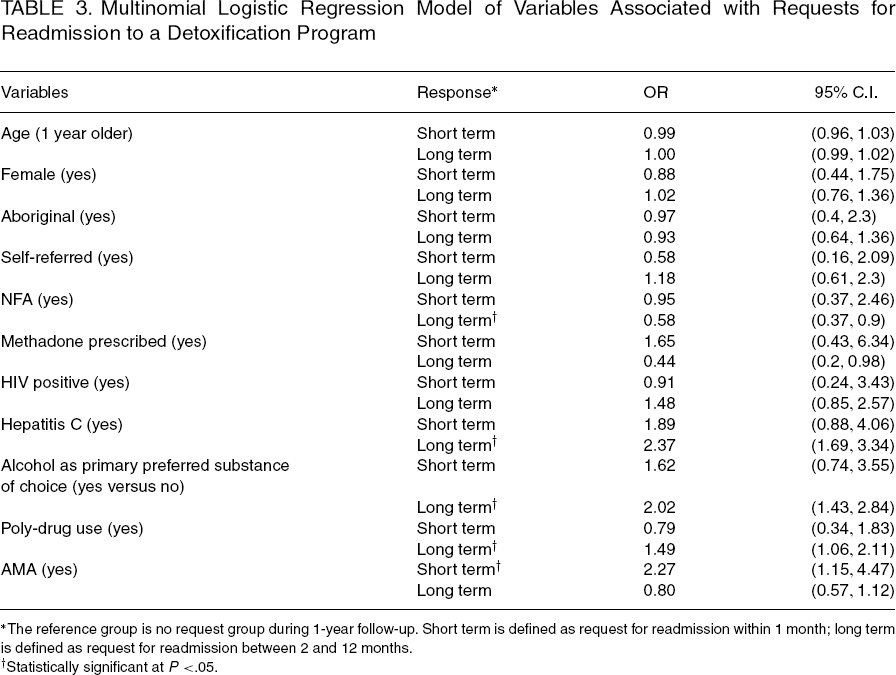
The reference group is no request group during 1-year follow-up. Short term is defined as request for readmission within 1 month; long term is defined as request for readmission between 2 and 12 months.
Statistically significant at P <.05.
Discussion
The present study reported rates and correlates of requests for readmission at a medically managed residential withdrawal management program for substance use disorders. Our results showed that 43% of the clients requested readmission within 1 year of their index admission. In addition, different sets of risk factors were associated with short-term and long-term requests for readmission.
Previous studies have investigated several risk factors, such as older age, being male, lack of stable housing, alcohol as a primary drug of choice, ploy-drug use, treatment incompletion at baseline, and lack of follow-up treatment, associated with readmission (2–4). These findings may help decision makers to tailor programs for at-risk groups to decrease the likelihood of need for readmission. However, these studies are not able to capture clients who request to be readmitted but drop out before engaging in the treatment. Our estimate is based on all clients who requested readmission and not just those who were actually readmitted. By investigating the risk factors associated with all requests for readmission a more complete picture of the need for further treatment can be developed.
Our results showed that AMA was the only significant risk factor that was associated with request for readmission within 1 month of the index admission. Requesting service again in such a short period indicated high inefficiency of the service and waste of health care resources. Our finding suggested that greater efforts should be taken to motivate clients completing the treatment program once admitted. Several factors have been identified to be associated with AMA in the previous studies, such as being younger of age, reporting opiates as the primary preferred drug, having HCV infection, and lower education level (3, 4, 8, 10–12). In addition, our recent study also found that the probability of dropping out of treatment was higher during welfare check issue period (8). The findings from these studies may provide information that can help clinicians and decision-makers to initiate preventive measures to decrease AMA, and therefore to reduce short-term request for readmission.
Clients who reported lack of a fixed address were found to be significantly less likely to request another service during 1-year follow-up. This finding contradicted other findings in the previous literature, which showed that residential instability was a significant predictor of detoxification treatment readmission (4, 9). This discrepancy might be explained by the setting of the current referral system. As mentioned above, instead of dropping by detoxification service in person, clients have to call ACCESS 1 to request the service. Previous research has shown that the clients with NFA are less likely to be admitted following their first request for admission (8). This may lead to frustration and discourage future requests. Our finding suggests that the current referral system might need to be adjusted to better meet the needs of the clients with NFA.
Our findings showed that the clients who reported alcohol as the primary preferred drug, and who reported to have HCV infection were more likely to request readmission, which were consistent with the literature (9). Our sample included the clients who lived in Vancouver's Downtown Eastside (DTES), where a high concentration of people with substance use disorders and injection drug use reside (13). In addition, a previous study showed that 87% of the injection drug use population residing in the DTES was infected with HCV (14). Therefore, even though we did not have data on injection drug use (IDU), the high correlation between HCV and both IDU and social marginalization could indicate that it was these factors instead of HCV infection that accounted for the high rate of requests for readmission.
The following limitations merit discussion. First, we did not have data on whether the clients receive further addiction treatment after completing the index admission, and it is possible that this could influence requests for readmission (2).
Specifically, clients who receive further addiction treatment are expected to be less likely to request for readmission. Second, the information on substance use and drug-related diseases were based on self-report. Although substance abuser's self-reports may vary as a function of different cognitive, motivational, and social factors, previous studies have shown that clients’ self-report of drug use are reasonably reliable and valid to provide descriptions of drug use, drug-related problems and the natural history of drug use (15, 16). Self-reported HIV and HCV status, however, are likely to underrepresent the true prevalence of these infections (17). Because some HIV or HCV positive clients might be misclassified into HIV or HCV negative category, the impacts of HCV and HIV on readmission might be underestimated.
Having acknowledged some of its limitations, this study extends research on withdrawal management programs by examining risk factors that may be associated with requests for readmission for substance use disorders. Information about the risk factors for recurrent treatment seeking may be especially useful to decision makers, allowing them to initiate measures to improve the effectiveness of initial admissions.
Footnotes
Acknowledgments
Xin Li holds a postdoctoral fellowship from the Michael Smith Foundation for Health Research. The authors would like to gratefully acknowledge the staffs at ACCESS 1 and Vancouver Detox for their administrative support and helpful comments. In particular, John Collens and Mary Marlow deserve special mention