
Abstract
The objectives of this study were to compare characteristics of outpatient substance abuse treatment (OSAT) units that serve high proportions of involuntary clients (ICs) with those that serve a low percentage of such clients. The authors analyze unit-level 1995–2005 data from the National Drug Abuse Treatment System Survey (NDATSS). Approximately 1/6 of OSAT units draw the dominant majority of their clients from involuntary referrals. OSAT units that treat a high proportion of ICs are less likely to be accredited by professional organizations, have fewer treatment staff with advanced degrees, and have shorter average treatment duration than do OSAT units that serve few ICs. OSAT units that serve ICs are more likely to offer legal and domestic violence services but are less likely to offer mental health services or aftercare. OSAT units that serve ICs are less likely to be hospital-affiliated than are other units. Clients at such facilities are more likely to be convicted of driving while intoxicated (DWI), are younger, are less likely to have received prior treatment, are more likely to remain abstinent after treatment, but are more likely to be remanded back to courts. The authors conclude that ICs are an important market niche in OSAT care. DWI is by far the most common offense reported in units that specialize in ICs. Aside from legal and domestic violence services, units with a high proportion of ICs appear to offer somewhat less intensive and professionalized services than do other facilities; however, clients at these units are more likely to be abstinent at the end of treatment and but more likely to be remanded back to the courts.
Introduction
The use of drug courts and diversion from prisons to drug treatment has received much attention from citizens and policymakers (1). Initiatives such as California's Proposition 36 seek to reduce social costs of incarceration by shifting nonviolent drug offenders into treatment interventions. Criminal justice referrals to substance abuse treatment have steadily increased over time, accounting by 2002 for 36% of all admissions into substance abuse treatment (2). Despite many evaluations of court-mandated drug treatment, the role and proper design of such interventions in reducing drug abuse and criminal recidivism remains contested (3, 4).
These and similar initiatives have engendered a long line of studies that find that involuntary clients experience no worse treatment outcomes than those experienced among other treatment participants. This general finding has been supported by the National Institutes of Health (NIH) consensus panels and by expert committees of the Institute of Medicine (e.g., 5,6). Most recently, Kelly, Finney, and Moos (7) report 1-year and 5-year outcomes from a prospective study of 2095 patients with substance use disorders. These authors find that patients required to undergo treatment by the criminal justice system reported similar or better outcomes as were found in two comparison groups: criminal justice–involved clients who were not required to seek treatment, and clients who were not involved in the criminal justice system.
Several data sources provide national overviews of treatment effects for involuntary clients. Meta-analyses have been reported, though few studies are designed to address differences across treatment programs (3, 8, 9). Anglin and colleagues (3) note that program heterogeneity and differences in implementation pose a key challenge to inferring the impact of involuntary treatment for client outcomes. Evidence that involuntary clients (ICs) enter treatment with different, often greater needs than voluntary clients (4, 10), provides a second obstacle to gauging program effectiveness.
The quality and content of services offered to court-mandated treatment clients has also received limited attention, though useful studies have been reported in particular areas, such as in mandated treatment for convicted drunk drivers (11). Other studies suggest that the content and quality of OSAT services influence client outcomes. Differences in staffing, treatment duration, and intensity of treatment, for example, help to account for general differences in client outcomes, and for outcomes within the specific population of involuntary clients (4, 9, 12). There is also evidence that counselor competency (13), group therapy (14), and the number of therapy sessions (15) are associated with better outcomes for involuntary clients. Howard and McCaughrin (9) found that for-profit facilities, facilities affiliated with a hospital, and facilities that offered more group therapy sessions had better outcomes as measured by the percent of involuntary clients completing treatment (9).
The existing literature has mostly focused on the link between involuntary referral and subsequent substance use. Although substance use is a key outcome, ICs have other distinctive needs. Many ICs require legal services (16). Other needs include housing and treatment for comorbid mental illnesses. Provision of ancillary services tailored to clients’ specific needs is linked to better outcomes and social performance, and has been identified as central to effective care (14).
Many studies on court-mandated clients focus on a particular drug court and the treatment centers to which the court refers offenders. Evaluations of one drug court or one set of treatment interventions rarely allow researchers to control for differences across drug treatment programs that clients are mandated to attend (8). Differences in ancillary services and quality of care may be important. Individuals receiving mandated treatment could attend higher- (or lower-) quality treatment facilities than are received by otherwise similar peers. Facilities that serve large numbers of mandated clients may systematically differ from others in available resources, treatment practices, and other factors that influence client outcomes. Such systematic differences in unit quality and practice could thus bias evaluations of mandated treatment interventions. If unit quality is associated with higher percentages of involuntary clients, studies that do not control for unit quality may find differences in mandated clients’ outcomes that are attributable to unit quality instead of the compulsory treatment.
This paper considers how variations in key outpatient substance abuse treatment (OSAT) unit characteristics are associated with the proportion of involuntary clients being served at such facilities. It examines whether and how OSAT units that serve mostly involuntary clients differ from otherwise similar OSAT facilities that serve mostly voluntary clients. This paper also documents the trends in these relationships and how services and unit characteristics have changed from 1995 to 2005.
It is the first study of its kind to use nationally representative OSAT panel data to examine trends and correlates of services provided in representative units that serve court-mandated clients. Given increasing numbers of criminal referrals to drug treatment, such data are important for policy makers to consider the population of OSAT units that serve involuntary clients, and the resulting quality and scope of services involuntary clients are likely to receive.
Data
The data for this study come from the National Drug Abuse Treatment System Survey (NDATSS). The survey covers a national sample of OSAT facilities. OSAT centers are defined as physical facilities that use at least half of their resources treat individuals with substance abuse problems on an outpatient basis. NDATSS is a mixed panel survey administered by the Institute for Social Research at the University of Michigan. Units previously surveyed are reinterviewed in subsequent waves. To maintain a representative sample and to replace panel units that die or exit, a new random sample of OSAT units is added at each wave. The sample is derived from a census of outpatient substance abuse treatment programs, excluding treatment programs run by correctional facilities and the Veterans Administration. NDATSS includes a representative sample of OSAT units using methadone maintenance and outpatient drug-free (nonmethadone) modalities. The sampling frame and methodology have been described in greater detail in and Adams and Heering (17) and Heering (18). Further details on NDATSS may be found in Pollack, D'Aunno, and Lamar (19).
Established survey methodology was followed to produce reliable and valid data. Data were collected in two phone interviews, one with the unit director and one with the clinical supervisor. The unit director and clinical supervisor are each asked to participate. The director answers questions pertaining to ownership, affiliations, funding, accreditation, and managed care arrangements. Clinical Supervisors were asked about staffing, treatment practices, client characteristics, and services. A total of 1454 nonmethadone observation points were surveyed for this analysis. We excluded methadone programs from the sample because most methadone programs had no or very few involuntary clients. There were 486 nonmethadone units surveyed in 1995 (88% response rate), 563 nonmethadone units surveyed in 2000 (89% response rate), and 405 nonmethadone units surveyed in 2005 (88% response rate). Involuntary clients made up less than 25% of clients in 955 units, and more than 75% of the clients in 320 units.
Measures
Some data in the survey are available regarding the specific sample of involuntary clients. Other data are only available as an average for all clients served by the OSAT unit. Clinical supervisors were asked: “In the most recent complete fiscal year, how many of your unit's outpatient substance abuse clients were involuntary clients who were compelled to come for treatment because of a court order?” They were also asked the percents of involuntary clients who were African American, Hispanic, and female. Data were also collected regarded the percentage of ICs charged with different specific crimes, including driving while intoxicated (DWI), theft, domestic violence, drug possession, and drunk and disorderly conduct.
NDATSS data contain three measures of outcomes specific to court-mandated clients: the percent abstinent at the end of treatment, the percent who meet treatment goals, and the percent who are remanded back to the courts. Although some programs may not expect or require abstinence at the end of treatment, this is a central treatment goal. Meeting treatment goals is a second, broader measure of overall compliance. Remand back to the referring courts represents noncompliance by the client serious enough to suggest a violation of the terms of diversion into treatment. Remand can represent different levels of noncompliance depending on the requirements of the referring court, the treatment facility, and the amount of involvement of the courts in the treatment program.
Supervisors also responded to questions about the sociodemographic and substance-use characteristics of all clients they serve. In addition, NDATSS explored key unit characteristics such as the number of clients treated per year; the percent of treatment staff with a masters degree, MD, or PhD; accreditation status from the Joint Council on Accreditation of Healthcare Organizations (JCAHO); for-profit, not-for-profit, or public ownership status; free-standing or affiliation with a hospital or mental health center; and the age of the unit.
Provision of various services was operationalized as the percent of clients who received that service. Services of interest included in the study are after-care, domestic violence counseling, mental health services, physical exams, employment counseling, and criminal legal counseling. We also included unit-level measures of mean treatment duration and a combined measure of average weekly number of hours of individual and group therapy. We controlled for both geographic and year effects.
Methods
We seek to examine the extent to which involuntary clients are referred to certain OSAT units and how treatment services compare across OSAT units that serve varying percentages of ICs. NDATSS includes repeated observations of the same units. Because unobserved (but stable) characteristics of specific units may be important, we use generalized estimating equations (GEEs) to account for repeated observations of the same OSAT unit.
Many OSAT units reported item nonresponse for at least one variable included in our regression specifications. To address potential biases associated with item nonresponse, we use multiple imputation in our baseline specifications (20, 21, 22). We use the STATA command mvis for the imputation and micombine for the analysis. Ten imputations were used for this analysis. As shown by Schafer (23), this is sufficient for sufficient estimation in large samples.
In our baseline regressions, the dependent variable is percent of clients who are court mandated. Our baseline regression includes client and organizational characteristics, both of which may be correlated with services provided by the unit and with the proportion of ICs. We also account for organization characteristics (accreditation, ownership and affiliation) and treatment practices (duration of treatment, treatment staff, number of therapy sessions per week).
We examined several different correlations between the percent of ICs and the independent variables. The first multivariate analysis included unit and client characteristics and crimes associated with involuntary clients. Because of the large number of covariates in the main regression, we also ran separate regressions looking only at unit characteristics, clients characteristics, and crimes. Each regression was run on all three waves combined and for each wave individually.
To sharpen distinctions across units, we also performed logit analyses using only units that had either less than 25% or more than 75% involuntary clients. We only report the bivariate results of this analysis because the results from logit regressions did not differ from regressions where the dependent variable was percent of involuntary clients. For convenience, we refer to the under-25% group as “non-IC” OSAT units. We refer to the over-75% group as the “IC” OSAT units.
We also performed the same regressions as above using outcome measures for involuntary clients as the dependent variable. We ran separate regressions on each of the outcomes at the end of treatment (% abstinent, % met goals, and % remanded). To examine various correlations, we ran these models on all independent variables, on client characteristics only, unit characteristics only, and criminal characteristics.
Results
Bivariate Means of Various Client and Unit Characteristics in Units with > 75% and < 25% Involuntary Clients
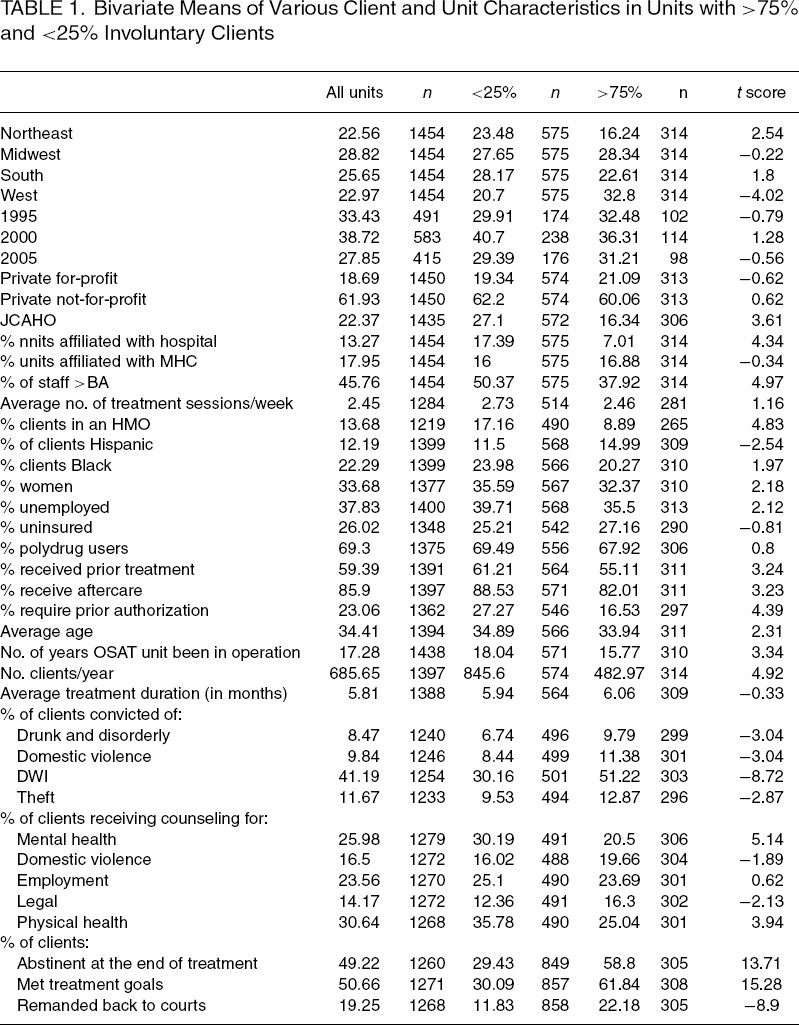
IC units appear to have less professionalized treatment staff. Only one third of IC-unit staff have advanced degrees, compared with 50% in non-IC units. In similar fashion, only 16% of IC units are JCAHO accredited, compared with 27% of non-IC units. IC units are less likely to be affiliated with a hospital and are more likely to provide legal services. More clients receive criminal legal counseling at IC units. We found no differences between the two groups on the average number of therapy sessions per week and in average treatment duration.
There is also a decline in the average number of involuntary clients at the units over time. In the average OSAT unit in our sample, 33% of clients were involuntary in 1995. This climbed to 38% in 2000 and fell to 28% in 2005. These changes were not accompanied by changes in the units who had less than 25% or greater than 75% of the clients involuntarily participating in treatment.
We also examined the average number of clients who were reported to complete treatment, who were abstinent, and who met treatment goals. Fifty-eight percent of involuntary clients at IC units were reported abstinent at the end of treatment compared with 30% at non-IC units. Approximately 60% of IC clients met treatment goals within IC units. Only 30% of ICs met treatment goals when they received services at non-IC units. IC units reported more clients remanded back to the court (22%) than did non-IC units (12%). These results were significant and stable across all three waves.
Regression Results
GEE analyses confirmed many observed bivariate relationships. There were 831 complete observations available for the full regression. After multiple imputation (MI), the analysis was performed on 1342 nonmethadone units. The point estimates for the regression results did not change, but the MI did create tighter confidence intervals. This increased the significance level of some variables and making a few variables significant that previously were close, but not significant. The use of MI did not appreciably alter our point estimates.
Regression of Unit and Client Characteristics on Percent of Involuntary Clients
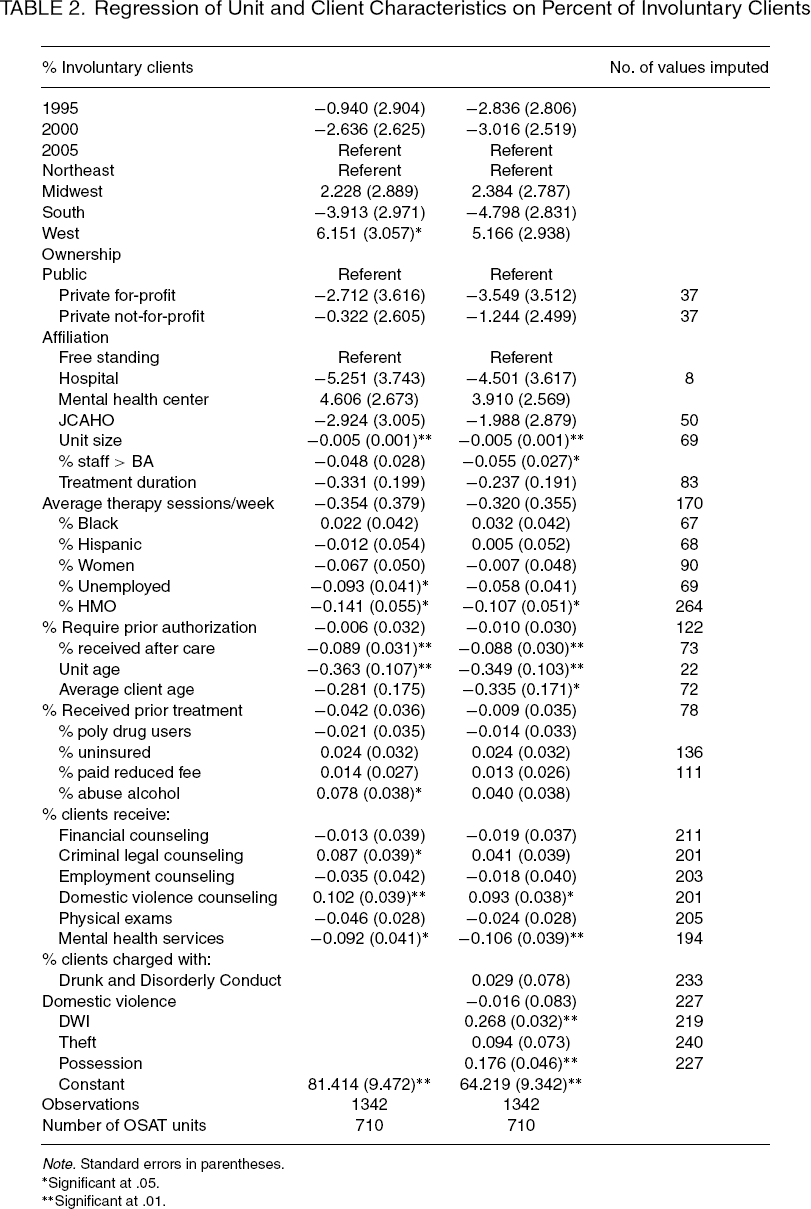
Note. Standard errors in parentheses.
Significant at .05.
Significant at .01.
In the main model with criminal offenses included (Table 2), the criminal legal counseling was no longer significantly associated with the percent of involuntary clients, but average age and the education level of the treatment staff were both negatively associated with the percent of involuntary clients. DWI and possession were the only two offenses that were associated with increasing involuntary clients.
Examining the relationship between client characteristics and the percent of ICs (results not shown) highlights other patterns in the data. A higher proportion of IC clients is associated with a smaller proportion of Hispanic clients. It is also associated with reduced prevalence of prior treatment for substance use disorders, and with a smaller proportion of female clients. No additional results are significant.
Other patterns emerge in year-specific regressions (not shown). Again, units with larger proportions of ICs have lower mean client age, and a higher proportion of clients experiencing alcohol disorders. In 1995 more units in the West had higher numbers of involuntary clients, but this relationship disappears by 2005.
In regressions of the percent of ICs on unit characteristics (not shown), several additional variables were significantly associated with an increasing percent of involuntary clients. Units with larger proportions of ICs were staffed with fewer people with advanced degrees and had fewer clients receiving mental and physical health services.
Treatment duration does not appear to differ between IC and non-IC units in multivariate analysis. The 2005 data contained questions about treatment duration for involuntary clients as well as the overall treatment duration. The average treatment duration for involuntary clients (6.5 months) is shorter than the average treatment duration on the whole (10.5 months).
Multivariate analyses (not shown) of criminal convictions indicate that “driving while intoxicated” was the only crime that showed a consistent, significant association with more involuntary clients. There was an association with drug possession and more involuntary clients. This association was significant in both pooled and year-specific regression specifications.
Treatment Outcomes
Unit Characteristics Associated with Treatment Outcomes of Involuntary Clients

Note. Standard errors in parentheses.
Significant at .05.
Significant at .01.
In the full model (results not shown), only being charged with a DWI was significantly associated with all three outcomes (% abstinent, % met goals, and % remanded). The effect was larger for being abstinence and meeting treatment goals. Being charged with possession was significantly associated with the percent of clients who were abstinent and who met the treatment goals at the end of treatment. Fewer clients were remanded back to the courts at units with a high proportion of treatment staff with advanced academic degrees. There is also an association between the percent of clients who receive criminal legal counseling and the percent of clients who met their treatment goals.
In the models that included criminal offending history, the results changed slightly. Treatment duration, criminal legal counseling, and employment counseling were no longer associated with clients meeting treatment goals. Among the criminal offenses, drunk and disorderly conduct was negatively associated with abstinence and treatment goals, and domestic violence was associated with more clients remanded back to courts. DWI and possession were associated with all three outcomes.
Examining the relationship between client characteristics and the three outcomes (not shown), units with more Hispanic clients had more clients remanded back to the courts. Fewer clients were remanded back to the courts in units that served a greater proportion of women. Polydrug users were less likely to be abstinent at the end of treatment. We also found strong time trends. Clients were more likely to be remanded back to the courts in 1995 and less likely to be abstinent in 2000 than in 2005.
Crimes Associated with Treatment Outcomes
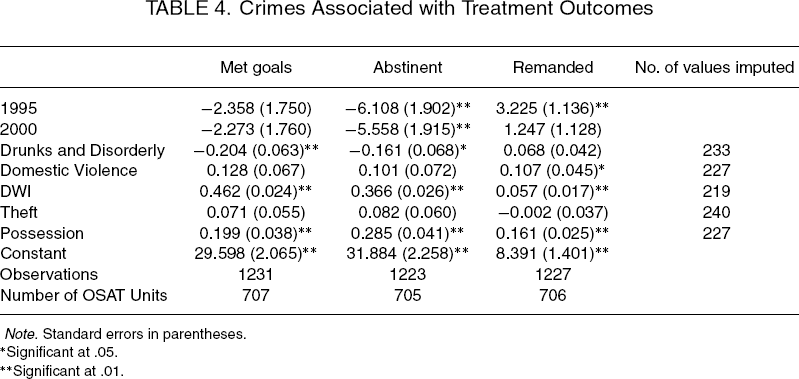
Note. Standard errors in parentheses.
Significant at .05.
Significant at .01.
Discussion
Study Limitations
Our analysis has several limitations that must be considered in evaluating the findings.
First, NDATSS only examines OSAT care. We do not analyze care for involuntary clients in residential facilities. Existing data indicate that OSATs care for more than three quarters of involuntary clients receiving substance abuse treatment (24). Estimates from the Treatment Episode Data Set (TEDS) find that, of clients referred from the criminal justice system, 77.6% entered OSAT units in 1995 and 80.2% of them went to OSAT units in 2004 (25). Our analysis is therefore pertinent to the average involuntary client, but likely does not apply to the most intensively served and monitored subset of involuntary clients. We presume that our analysis does not apply to offenders charged with serious felonies, who may be referred to residential, governmental, or prison programs for treatment.
Second, NDATSS data capture unit-level associations. We cannot determine the extent to which involuntary clients receive different services from those provided to voluntary clients in the same units.
Third, our data contains no information on differences in the underlying treatment need. As noted above, ICs may have greater needs at baseline than voluntary clients in the same facilities (4).
Fourth, we have little information regarding the content of OSAT services of special import to ICs. We capture, for example, whether legal assistance is provided to clients. We know little about how such services are provided or the proportion of clients who require these services. More clients receive criminal legal counseling at IC units than at non-IC units. Still, less than 20% of clients at units with high proportions of ICs receive legal counseling. Our data do not indicate how many need further legal assistance. IC units are also more likely than others to offer domestic violence counseling. This pattern is consistent with the higher prevalence of criminal domestic violence charges among involuntary clients.
Other findings suggest that ICs receive a somewhat less intensive mix of services, provided by somewhat a less professionalized (as measured by academic degrees) distribution of OSAT staff. For some services, such as mental health services and physical exams, the proportion of ICs is inversely related to the proportion of clients receiving these specific services.
Finally, we have no measure of court involvement and communication between courts and treatment facilities, a factor that some studies have associated with favorable outcomes (3).
Despite these limitations, we find evidence that IC units offer services that (imperfectly) match the distinctive needs of involuntary clients. Our data do not allow us to draw strong inferences about the effect of cross-unit differences on client outcomes. More clients on average are remanded to the courts at IC units. At the same time, a higher proportion of clients successfully complete treatment and are abstinent at the end of treatment in the same units. These apparently contradictory results are consistent with the view that coercive treatment strategies can increase clients’ likelihood of attaining abstinence and other treatment goals, even as such strategies increase the likelihood that some clients will receive more explicit punishment and pressure from legal authorities. One caveat about this finding is that we cannot be certain that higher reported abstinence is unbiased. There is a strong incentive for IC clients to report abstinence to avoid punishment. Depending on the requirements of the referring court and the treatment center, deception may or may not be possible. Drug and alcohol testing, for example, may elicit more candid responses regarding substance use.
Many OSAT clients receive services through involuntary referrals from legal authorities. Involuntary referral is especially common within particular client subgroups: Younger individuals, first-time offenders, men, and individuals without previous substance abuse treatment (10).
It may surprise some readers that the population of ICs captured in our data is a relatively criminally inactive, majority-white population. The majority of ICs receiving OSAT services are charged with relatively minor, often alcohol-related offenses. IC units included twice the prevalence of previous DWI offenses as non-IC units. ICs charged with DWI do not appear to have high rates of other criminal convictions related to their OSAT care. Individuals charged with DWI, typically alcohol users, appear to be the largest population of clients served by such interventions. The association with more clients being remanded back to the units suggests that there is heterogeneity among these clients and coercion is effective for many, but not all clients.
Our results suggest that treatment units where most clients are court mandated are a specific market segment served by a subset of OSATs that specialize in such care. This market segment for alcohol abusers charged mainly with domestic violence and DWI may also explain why those units offer less intensive services and still have good compliance (higher percentages of clients abstinent at the end of treatment and more clients meeting their treatment goals). Such offenses provide an important pathway for (often nondependent) alcohol abusers to come to the attention of legal authorities and the treatment system. This population of alcohol abusers may require less intensive services than do clients with dependence disorders. The threat of coercion may also prove more effective for this population than for other clients. Another finding that points to a market niche is that many units with high concentrations of court-mandated clients are smaller and newer, suggesting that these units arose to meet a demand created by drug diversion courts and similar interventions.
Individualized trial data would help disentangle how clients charged with different offenses would likely respond to differing levels of treatment. Coercion and lower intensity services may work well for the subset of involuntary clients charged with alcohol-related misdemeanors and for first-time offenders without prior treatment. More intensive services are likely required for more criminally active clients and for those with more severe dependence disorders. Policy makers and courts should implement diversion programs that entail a more comprehensive assessment of needs and a broader range of services, tailored to meet the needs of each client and effective in achieving good outcomes for a broader range of offenders. Many facilities that serve involuntary clients offer a relatively narrow range of services that are not tailored to individuals with severe disorders. We hope to explore these questions in future work.
Footnotes
Acknowledgments
Grant R01-DA32727 from the National Institute on Drug Abuse (NIDA) and a seed grant from the Chicago Center of Excellence in Health Promotion Economics supported this research. The views expressed here are the authors’ and not necessarily those of NIDA. The Institutional Review Board of the University of Michigan approved this research