
Abstract
Although screening, brief intervention, and referral to treatment (SBIRT) has been a popular model to address potential substance abuse issues in primary care, there is a need for innovative approaches for training providers and staff on SBIRT protocols. An interdisciplinary approach to SBIRT training, named ICARE, was implemented at 3 different medical settings. The ICARE team trained 85 employees at an academic family medicine residency center and 37 employees across 2 rural community health care clinics. Using an innovative “learner-driven” approach, the authors implemented a combination of didactic and interactive training strategies that included on-site coaching, patient simulation exercises, as well as large- and small-group learning.
We conducted a screening, brief intervention, and referral to treatment (SBIRT) implementation project using an innovative “learner-driven” curriculum and training approach. Our project, referred to as “ICARE,” was facilitated by interdisciplinary teams comprising medical family therapists and substance abuse counselors at 2 unique primary care settings in rural eastern North Carolina. What follows is a brief report on our implementation experience.
Learner-Driven Training Matrix
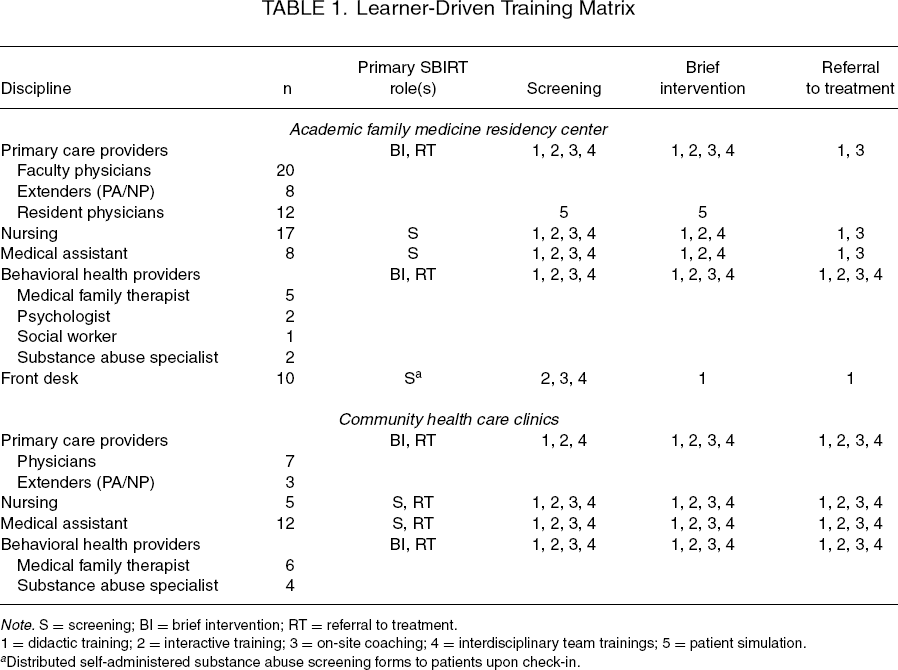
Note. S = screening; BI = brief intervention; RT = referral to treatment.
1 = didactic training; 2 = interactive training; 3 = on-site coaching; 4 = interdisciplinary team trainings; 5 = patient simulation.
Distributed self-administered substance abuse screening forms to patients upon check-in.
A learner-driven approach to curriculum development was an essential aspect of ICARE. Unlike other projects with a preset SBIRT training curriculum, ICARE's curriculum evolved from interdisciplinary team members’ feedback. ICARE enlisted content experts who included substance abuse specialists, medical family therapists, members of the Motivational Interviewing Network of Trainers, as well as faculty and clinical providers with expertise to serve as SBIRT trainers. The use of content experts allowed for the dissemination of the most recent and relevant knowledge to further the implementation of the SBIRT protocol into each clinic.
Initially, all team members were trained in the general SBIRT protocol. This included an introduction to brief screen and secondary screening tools, training in motivational interviewing (MI), brief interventions, and options for advanced training and skill development via the ICARE coaches. Further training was based on needs and requests elicited both formally and informally from individual coaching sessions, as well as group trainings. Common requests included topics similar to those reported in previous SBIRT implementation literature (1), such as confidence with substance abuse basics and diagnostics, navigating regional referral processes, engaging specific populations (e.g., patients with pain management concerns), competence with brief intervention skills and strategies, and strategies for engaging patients resistant to or ambivalent about addressing their substance abuse issues. If the ICARE team believed someone from outside the project could provide better training around a specific topic (e.g., local narcotics officers to speak on prescription drug abuse), experts were scheduled to provide additional didactic training.
A combination of didactic and interactive training strategies, as well as the provision of coaching and feedback, is essential to the implementation SBIRT (1). Thus, ICARE training experiences included innovative teaching techniques to help reinforce the material and increase competency in SBIRT. For example, AFMRC resident education included use of didactic sessions, as well as standardized patients (trained actors) who simulated substance abuse issues. Residents practiced SBIRT elements, particularly brief interventions during these simulated encounters, with coaches, actors, and peers providing immediate feedback. Content-specific trainings were embedded into their residency afternoon didactic sessions and at grand rounds with faculty and mid-level providers (i.e., extenders) present.
Content-specific trainings on substance abuse basics and diagnostic issues, SBIRT protocol information, and information vital to treating special populations were disseminated via didactic presentations. However, team member feedback often revealed a need for enhancing competence and confidence on SBIRT skills. ICARE staff developed interactive trainings that provided interdisciplinary team members the opportunity to learn and practice specific SBIRT skills in a one-on-one format (i.e., coaching with actual patients, impromptu role-playing, lively discussions about worst-case scenarios and SBIRT successes). Although brief intervention skills were not formally assessed through a checklist or video review, coaches were routinely available at each site for modeling and feedback.
Team members requested and responded best to on-site coaching. ICARE staff with specialized skills in substance abuse counseling and MI served as on-site coaches. They circulated to each part of the system and were regularly available to join patient encounters and work alongside team members (e.g., front desk staff, nurses, providers) to model elements of SBIRT. This regular “on the job” coaching reinforced the SBIRT training and protocol implementation, and frequently helped the protocol reach completion as opposed to stalling at the earlier SBIRT steps. For example, team members would often struggle navigating a treatment referral, so a coach would provide guidance in completing this task. ICARE staff responded to all feedback with a potential solution or validation of a larger systemic concern within a week to maintain implementation momentum. Larger systemic concerns (e.g., lack of placement options, laboratory protocols for admission) were communicated to the state's leadership for consideration and future policy recommendations. Contact between team members and coaches were dependent upon level of complexity of the patient scenario and comfort level of the individual provider. A total of 3500 hours of coaching was supported via this project.
Although interdisciplinary team members faced many challenges to SBIRT implementation, preliminary findings support the importance of incorporating a mechanism for team members to drive their SBIRT training. Specifically, based on preliminary focus group data, team members reported feeling more comfortable with the SBIRT process over time, a greater awareness of the prevalence of substance use disorders, and a greater confidence in the benefits of screening as a method of prevention. Researchers should continue to explore innovative training topics and techniques for implementing SBIRT into primary care settings, specifically studying issues around the benefits of an existing integrated care infrastructure and financial sustainability.
Footnotes
Acknowledgments
This study was supported by the North Carolina Foundation for Advanced Health Programs, awarded to Jennifer L. Hodgson.