
Abstract
Alcohol screening and brief intervention (SBI) is recommended for all primary care patients but is underutilized. This project trained 111 residents and faculty in 8 family medicine residencies to conduct SBI and implement SBI protocols in residency clinics, then assessed changes in self-reported importance and confidence in performing SBI and brief intervention (BI) rates. Clinicians reported significant increases in role security, confidence, and ability to help drinkers reduce drinking and decreased importance of factors that might dissuade them from performing SBI. Stage of change measures indicated 37% of clinicians progressed toward action or maintenance in performing SBI; however, numbers of reported BIs did not increase. At all time points, 33% to 36% of clinicians reported BIs with ≥10% of the last 50 patients. Future studies should focus on increasing intervention rates using more patient-centered BI approaches, quality improvement approaches, and systems changes that could increase opportunities for performing BIs.
Keywords
Introduction
Alcohol screening and brief intervention (SBI) reduces at-risk drinking (1, 2), is cost-effective (3), and decreases health risks (4). The US Preventive Services Task Force recommends SBI for all primary care patients (5); however, SBI is infrequently performed in primary care (6). If SBI is to become widely translated into outpatient practices, SBI training must become integrated into residency curricula. Previous studies have shown that clinicians’ lack of confidence in assessing alcohol use and providing brief advice (7) is a significant barrier to SBI practice. Research indicates that low screening and intervention rates correlate with lack of training and low clinician self-efficacy (8–10). Several training efforts with practicing physicians have produced modest increases in rates of advising patients to reduce drinking (11–13); however, studies in residency training programs have yielded conflicting results. Some generated increased resident confidence in identifying problem drinking (14) and advice to reduce drinking (14–16), whereas others showed increased alcohol interventions only among faculty (17, 18). One study conducted among practicing physicians suggested that physician intervention rates increased only among clinicians who already felt secure and committed to working with drinkers (19).
The Georgia-Texas “Improving Brief Intervention” Project offered alcohol SBI training in 8 Family Medicine residency programs in Georgia and Texas, in conjunction with providing assistance to local personnel in designing protocols for instituting routine alcohol screening and prompting of providers to conduct brief interventions. The project's aims were to (1) train residents and faculty to conduct alcohol SBI in their outpatient practices; (2) design and implement local SBI protocols at each of 8 residency clinics via collaboration between project leaders and local clinic personnel; (3) assess changes in clinicians’ perceived importance and confidence related to SBI; and (4) measure project impact on clinicians’ self-reported BI rates.
Methods
Sample
Eight family medicine residency training programs participated in this study between January 2006 and December 2007. Nine programs in Texas and Georgia were invited to participate, and 8 agreed to do so. Two programs withdrew prior to inception for financial reasons and a third was lost due to relocation to a new hospital. Three additional residency programs were recruited to replace them, resulting in 8 participating residency programs out of 12 potential participants (67%). Methods for training clinicians and implementing routine SBI in residency clinics were based on those utilized in the University of Connecticut's “Cutting Back” program (11, 12) and adapted for residency use in the Macon Healthy Habits Project (15).
Project Implementation
The project was presented to faculty and key residency and clinic stakeholders at an informational meeting. On-site stakeholders selected a faculty site coordinator and created an SBI implementation committee. The typical committee consisted of the residency director, faculty site coordinator, clinic director, nursing supervisor/administrator, a resident, and representatives from medical records, registration, and information technology. A clinic implementation guide, also adapted from “Cutting Back,” was used to guide the committee in adapting training procedures, implementing SBI protocols, and assigning individual tasks for preparation and startup.
Sbi Protocol
The SBI protocol integrated tobacco and alcohol screening into nursing vital signs. Nurses asked the National Institute on Alcohol Abuse and Alcoholism (NIAAA) single alcohol screening question (20) as an initial alcohol prescreening question, then administered the Alcohol Use Disorders Identification Test (AUDIT) (21), the project's screening instrument, to prescreen-positive patients. Patients were asked to complete paper AUDITs before seeing the physician. Physicians scored the AUDITS during office visits, then conducted stratified brief interventions modeled after those of the Cutting Back program (11, 12). For patients with AUDIT scores of 15 or less, clinicians offered a brochure-based brief intervention focused on contracting with patients to cut back to NIAAA “safe drinking limits” (for men under age 65, no more than 14 drinks per week and no more than 4 drinks per occasion; for women and men aged 65 and over, no more than 7 drinks per week and no more than 3 drinks per occasion) (20). For patients with AUDIT scores of 16 or more, clinicians encouraged abstinence, assessed and addressed potential withdrawal risk, and attempted to contract with patients for drinking cessation. For patients who were unwilling to quit, physicians attempted to negotiate a lower drinking goal. Clinicians also offered a menu of additional services, including medication, self-help groups, or specialty referrals. Four residency clinics with electronic medical records (EMRs) created mechanisms for accommodating information regarding prescreen and screening results, diagnoses, and documentation of interventions performed; 4 other clinics used traditional paper charts.
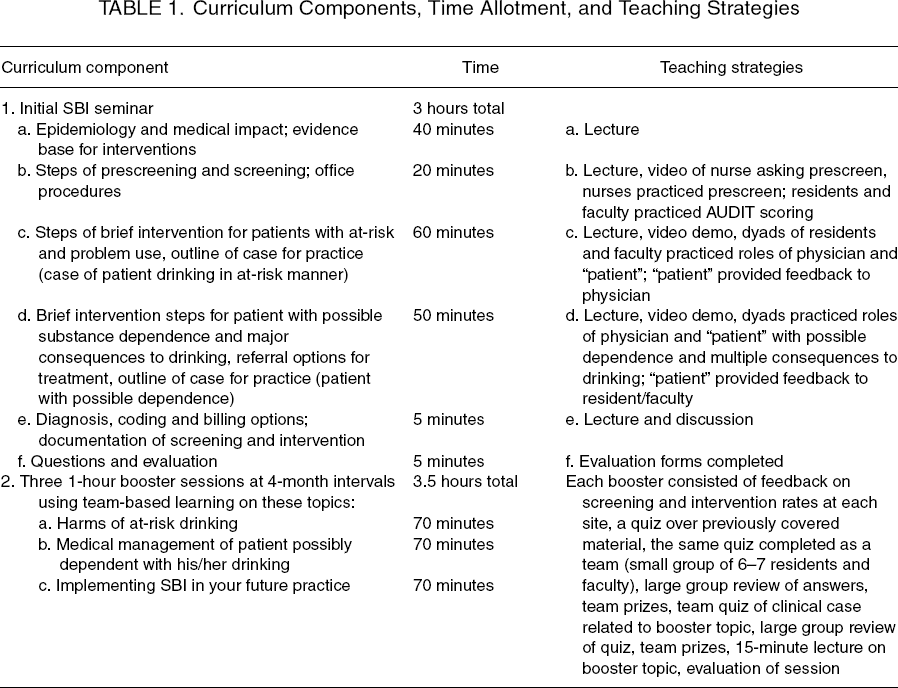
Curriculum
Curriculum Components, Time Allotment, and Teaching Strategies
Faculty
Four faculty and 3 project staff members prepared the teaching materials. The principal investigator, whose background includes a substance abuse faculty development fellowship and certification by the American Society of Addiction Medicine, taught all of the initial workshops assisted by other project faculty and staff. The other 3 faculty had graduate training in substance abuse or 3 to 25 years of previous experience of SBI teaching and curriculum development. Each booster session was taught by 2 faculty and 1 staff member. At least 2 faculty from each participating residency participated in a faculty development workshop of 1½ days to learn SBI skills and implementation strategies.
Participants
Residents and faculty who participated in the 3-hour SBI training seminars were recruited to participate in the project's research component, which was approved by the Institutional Review Board of Mercer University. Written informed consent was obtained. Of 300 physicians (106 faculty and 194 residents) who attended initial training seminars, 195 (65.0%) enrolled in the study and completed a pre-training clinician questionnaire. Among enrollees, 134 (68.7%) completed post-training questionnaires within 30 days of training, and 125 (64.1%) completed 12-month follow-up questionnaires. Statistical analyses were performed on the 111 clinicians (34 faculty and 77 residents; 56.9% of enrollees) for whom all 3 data points were available.
Comparison of Completers and Noncompleters
Because a relatively large number of participants did not complete surveys at all 3 time points and were not included in these analyses, a comparison of the 111 with complete data and those with only 1 or 2 surveys completed (n = 84) was conducted. There were no significant demographic differences (age, gender, race, ethnicity) between the 2 groups. SBI measures were also compared across the 2 groups. Results showed significantly higher levels of role security for those with complete data compared to those with incomplete data (mean pre-training score = 7.75 vs. 7.26; P < .05). All other measures (therapeutic commitment, importance, confidence, pros, cons, number of BIs performed) were similar for each group.
Measures
Definitions and Assessment of Behavior Change Constructs for SBI for Alcohol
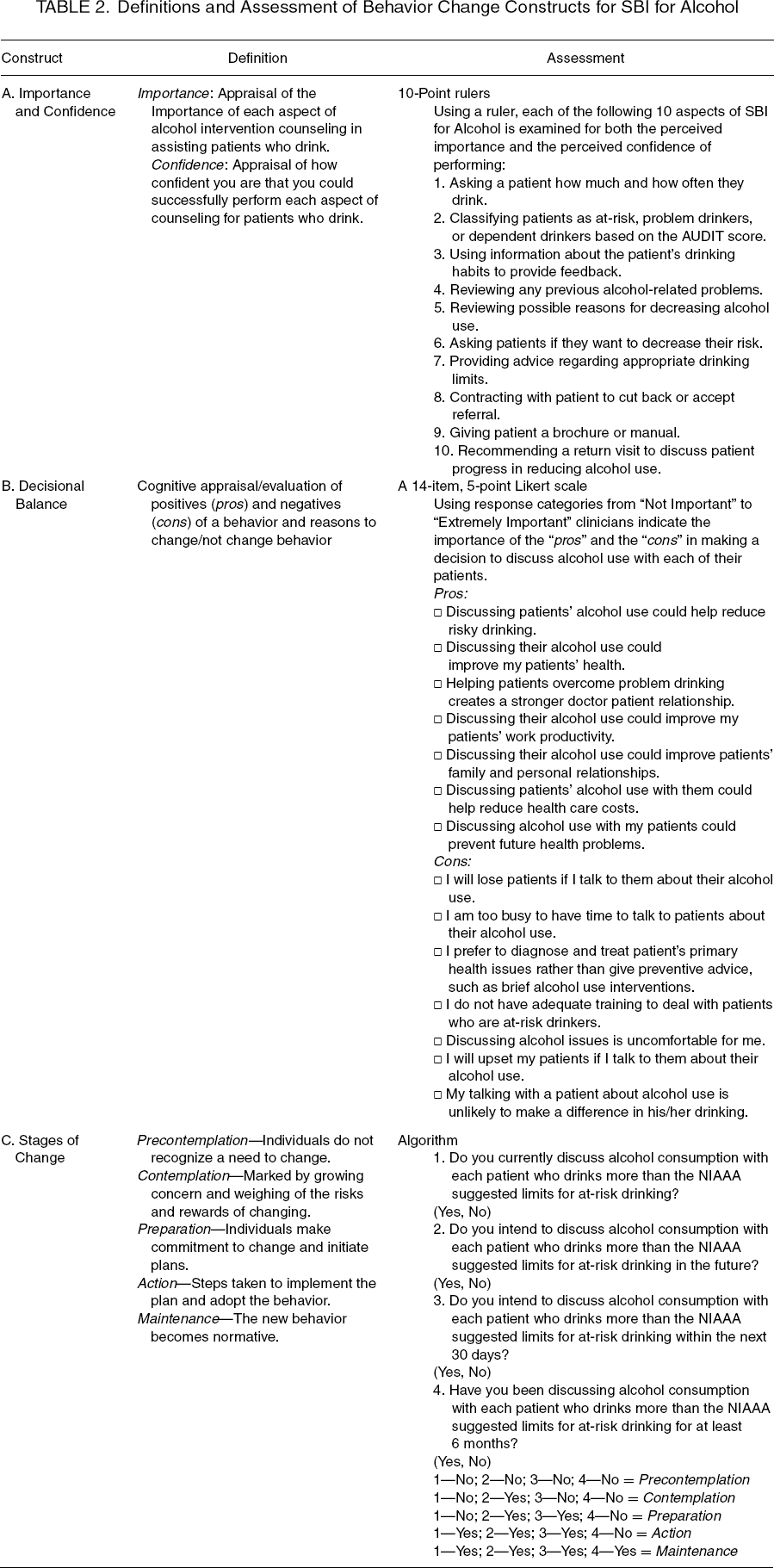
Participants recorded their level of importance and confidence on a 10-point Likert scale. Three other items designed to measure respondents’ confidence in performing critical SBI tasks were also included. These items, rated on a 5-point Likert scale (from “not at all confident” to “extremely confident”) asked clinicians to rate their confidence in asking patients about their alcohol use, advising them to cut down or quit, and helping them cut down or quit. A decisional balance measure, patterned after measures developed for smoking cessation intervention (25), was used to evaluate clinicians’ pros and cons for performing alcohol SBI. These items measure how important each “pro” and “con” item is to the clinician in deciding whether to engage in SBI behaviors. Items were scored from 1 (not important at all in their decision) to 5 (very important—see Table 2, Section B, for list of items). Additionally, an algorithm, composed of a series of yes/no questions, was created to identify physicians’ stage of change in regard to performing BI with at-risk drinkers (see Table 2, Section C, for items and scoring).
Statistical Analyses
Cronbach's alpha was used to measure internal consistency at post-test of 5 self-assessment instruments (importance scales, confidence scales, 3-item confidence scale, and 7-item pros and cons scales), and all were found to be acceptable (.961, .973, .863, .828, and .861, respectively). Paired-sample t tests and chi-square analyses were used to compare pre-training responses with responses post-training and at 12 months. Physicians were also asked at each time point how many BIs they had performed among the last 50 patients they had seen.
Results
Demographics
Demographic Characteristics of Residents and Faculty (N = 111)
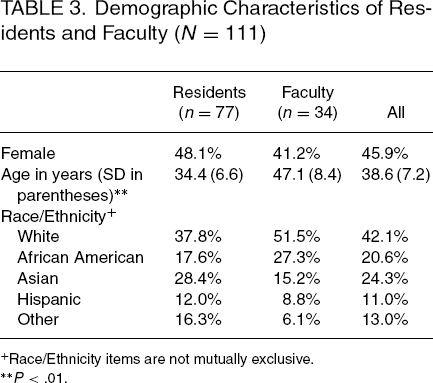
Race/Ethnicity items are not mutually exclusive.
P < .01.
Role Security and Therapeutic Commitment Measures
Mean scores for role security and therapeutic commitment scales were tracked longitudinally. Clinicians’ scores for role security (acceptance of and comfort with their role in screening and brief intervention), increased from 7.75 at pre-training to 8.74 (P < .001) after training. Increases were still significant after 12 months (8.44; P < .001). Modest, statistically insignificant changes in scores were observed on the therapeutic commitment scale (commitment to perform screening and brief intervention). A mean pre-training score of 6.94 increased to 7.04 (P = .46) after training and to 7.09 after 12 months (P = .34).
Measures of Importance and Confidence in Performing SBI
Mean pre-training composite scores on the 10-point SBI importance scale were high (8.52). The composite mean increased significantly to 9.10 (P < .001) after training; however, this increase was not sustained at 12 months (8.60, NS). Individually, all 10 importance items showed significant increases in mean scores between pre- and post-training. Only 1 item remained significantly higher at 12 months—the importance of giving the patient a brochure/manual.
Analyses of composite confidence scores showed significant increases over pre-training levels both immediately post-training (7.53 to 8.84; P < .001) and after 12 months (8.41; P < .001). All 10 individual confidence items showed significant increases between pre- and post-training. Although there was some decline at the 12-month follow-up, the mean scores for all items were still significantly higher than pre-training levels.
Comparison of Physicians’ Global Confidence in Performing Specific SBI Tasks (N = 111)
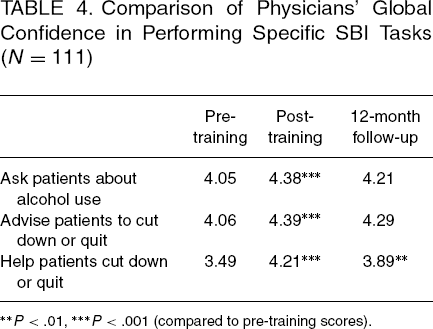
P < .01
P < .001 (compared to pre-training scores).
Decisional Balance Measures
Composite scores were calculated by combining all 7 positive items into a single “pros” factor and the 7 negative items into a “cons” factor (see Table 2 for all 14 items). No significant changes were seen in the composite “pro” score (perceived positive factors that can influence clinicians in favor of performing SBI) between pre-training and post-training (3.97 to 4.08; NS) or at 12 months (3.86; NS). Although there was no change in the “con” score between pre-training and post-training (2.11 to 2.12; NS), there was a significant decrease in the composite “con” score between pre-training and the 12-month follow-up (2.11 to 1.94; P < .05), indicating a decrease in the relative importance of perceived negative factors that could influence clinicians against performing SBI.
Readiness to Perform Interventions for At-Risk Drinking: Stage-of-Change Measure
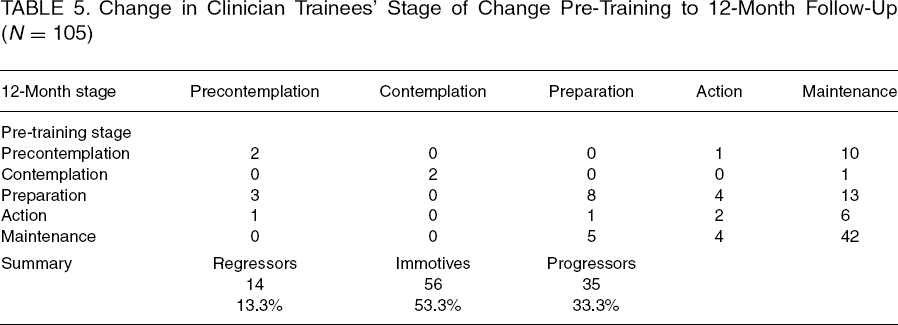
Using the scoring algorithm described in Table 2, clinicians were assigned to 1 of 4 stages of change at all 3 time points (see results in Table 5). The resulting stage of change variable at pre-training was cross-tabulated with the same variable at the 12-month follow-up to identify how clinicians progressed, or in some cases regressed, in their stage of change. A slight majority of clinicians maintained the same stage of change between pre-training and 12-month follow-up (53.3%) and about one third progressed to a higher stage of change. Only 13.3% reported a lower stage of change at 12-month follow-up. There was an overall increase in those endorsing the “maintenance” stage (47.7% pre-training, 69.7% after 12 months), indicating that for them SBI had become normative.
Change in Clinician Trainees’ Stage of Change Pre-Training to 12-Month Follow-Up (N = 105)
Clinician Self-Report of Interventions Performed
At each time point, clinicians reported how many of their last 50 patients had been counseled to cut down or quit using alcohol. Responses were categorized into 3 groups: 0, 1–5, and 6 or more interventions. There were no significant changes in self-reported BIs over time. At all 3 time points, about one third of clinicians reported performing 6 or more interventions among their last 50 patients (35.6%, 35.6%, and 33.0%, respectively), whereas 6% to 10% reported performing no interventions. The largest percentage of respondents reports conducting 1 to 5 interventions among their last 50 patients. Comparisons of BI rates between the 4 clinics with EMRs and the 4 with paper-based records revealed no significant differences.
Discussion
This study provides new knowledge of the impact of SBI training efforts and SBI systems interventions on clinicians in residency training settings. It is one of the first residency training studies to demonstrate an increase in clinician role security, a factor previously shown to correlate with clinician intervention rates (13, 23). It is also one of the first studies to use transtheoretical model measures to evaluate residency clinicians’ attitudes toward SBI and the impact of SBI training on these attitudes. Of further interest is the high level of both importance and confidence ascribed by clinicians to SBI at pre-training, a finding that differs from numerous previous studies reporting significant clinician reluctance to screen and advise patients about alcohol use (26–29). Although reported levels of importance of performing SBI tasks did not increase, perhaps due to high pre-training levels, clinicians reported increased confidence in their ability to perform all 10 SBI-related tasks surveyed. Decisional balance analysis also found declines in the perceived importance of negative factors that sometimes discourage physicians from conducting SBI. Clinicians’ “readiness” to perform SBI also improved considerably, as evidenced by progression across the stages of change by one third of participants and the high percentage of participants (68%) who reported maintenance of SBI activities after 1 year, indicating that SBI had become normative for them.
Despite these positive changes, clinicians’ therapeutic commitment only showed a transient increase, which disappeared after 12 months, and self-reported BI rates did not increase. These findings are consistent with other studies that have found major challenges to increasing primary care clinicians’ brief intervention rates despite investment of significant time and resources (13, 29, 30). Residency systems issues appeared to complicate attempts at increasing intervention rates, as programming screening and intervention into EMRs proved problematic at most sites, nurses screened only 45% of patients and preceptors failed to reinforce the need for SBI for at-risk patients. Provision of preventive services has also been shown to be lower in patient populations with high levels of competing demands and high percentages of Medicaid patients (31, 32). These characteristics were present in most of our residency clinics. The low level of intervention rates suggests that, for many participants, brief interventions remained limited to only the most obvious problem drinkers, who are often more resistant to intervention efforts and less likely to reduce their alcohol use. Such experiences could in fact serve to discourage novice clinicians from further SBI activities. This highlights the need for future efforts to include systems changes that strategically integrate SBI into EMRs while also reinforcing SBI compliance at multiple levels including nursing, where more consistent screening could prompt more resident interventions, and precepting, where faculty insistence on residents’ performing BIs on all patients with positive screens could also increase BI rates. Creation of EMR fields for recording BIs could also provide a more objective method for tracking clinician BI rates.
This project also points toward 2 other important issues that may remain as obstacles to increasing SBI rates in primary care. One is the focus of primary care clinicians on treatment rather than prevention in primary care settings (28). Alcohol SBI has been found to be one of the most underutilized effective prevention interventions in primary care (3). Sustained increases in preventive services have been difficult to achieve in US primary care clinics, although individual projects (33) have been successful using intensive interventions that were highly individualized to meet particular practice needs. Our physician trainees frequently questioned the need for doing prevention-focused BIs with patients who consumed alcohol in risky amounts with few negative consequences. Changing this attitude and behavior may require a major paradigm shift, which is unlikely to result from brief SBI training. Emerging US primary care models such as the patient-centered medical home are attempting to reengineer primary care clinics to utilize primary care teams to provide preventive services. Until preventive care becomes a higher priority in primary care practice, future SBI training efforts may continue to experience significant challenges.
Another issue that may explain physicians’ hesitance to perform SBI after training is strain on the doctor-patient relationship created by physician-driven advice-oriented BIs with some patients. During trainings, several faculty members suggested that they would prefer not to broach the sensitive issue of alcohol at an initial patient visit. Beich et al. (34) reported that numerous Danish general practitioners with BI training found it difficult to establish rapport with patients with positive alcohol screens, noting that SBI interrupted the natural course of office visits and created strain in the doctor-patient relationship. Given the centrality of the doctor-patient relationship to primary care practice, this critical concern deserves further exploration. Future training efforts should explore clinicians’ responses to use of alternative BI intervention methods such as motivational interviewing (24), which has been shown to strengthen the doctor-patient relationship while also facilitating patient behavior change and improving the efficiency of consultations (35).
One encouraging finding is that at all time points, 33% to 36% of clinicians reported performing more than 5 interventions in their last 50 patients. Similarly, Anderson et al. found that 40% of clinicians trained in a multisite SBI implementation study reported performing a higher percentage of BIs than their colleagues (≥10% of at-risk drinkers) (19). Future studies may benefit from exploration of the individual characteristics of these “high-activity” clinicians. Additionally, previous studies have found that nonphysicians can effectively perform SBI and may do so at higher rates than physicians (11). Future SBI trials may benefit by exploring effective ways of designing multidisciplinary SBI teams that also utilize nonphysicians to perform BIs. In such multidisciplinary SBI teams, “high-activity” physicians might be used to train others in BI and referral and serve as champions in implementing SBI systems in their practices, whereas other physicians might simply provide reinforcement and encouragement to patients following a visit with nonphysicians, prescribe alcohol medications for dependent patients, or refer patients to higher levels of treatment. In practices that lack nonphysician providers who can perform BIs, perhaps high-activity clinicians could accept referrals from other clinicians in their practice who are more reluctant to perform SBI.
Findings of this study could be biased due to limited clinician participation rates and follow-up rates. However, participation and follow-up rates are similar to those reported by Anderson et al. (13) in their World Health Organization (WHO) study of SBI implementation. Likewise, comparisons of completers and noncompleters found no significant demographic differences and minimal differences on the various SBI measures. Future studies should explore methods for increasing clinician participation rates in translational SBI studies. Another limitation of this study is its reliance on self-report to measure physician attitudes and intervention behavior following training.
In conclusion, this program, which provided skills-based training in alcohol SBI and implemented SBI protocols in 8 residency clinics, resulted in increases in physicians’ role security regarding SBI, greater confidence in performing SBI tasks, and reduced importance of negative factors discouraging brief intervention; however, clinicians reported no increase in the numbers of BIs performed. Future efforts should continue to explore methods for creating effective SBI systems as a part of comprehensive primary care prevention efforts and in identifying the optimal role for physicians in such systems.
Footnotes
Acknowledgments
This study was funded by the US National Institute on Alcohol Abuse and Alcoholism, grant R25-AA-014915.