
Abstract
Background
Krathom (Mitragyna speciosa Korth.) is the most commonly used illicit substance in Thailand, and its use has become widespread internationally. Studies on krathom dependence and its health impact are scarce, as there has been no instrument to measure its dependence syndrome and classify krathom users. This study aimed to develop and explore the factor structure, reliability, and validity of a Krathom Dependence Scale (KDS).
Methods
This study comprised 2 phases. First, cross-sectional surveys were conducted with 523 (Phase I) and 595 (Phase II) male villagers aged >25 years who were regular, occasional, ex-, or nonusers of krathom. Scale construction was based on the qualitative results from users and previous literature. Exploratory factor analysis (EFA) using maximum likelihood extraction with oblimin rotation was conducted in Phase I and confirmatory factor analysis (CFA) in Phase II to confirm the construct of the scale. Internal consistency of the KDS was assessed using Cronbach's alpha coefficient. Discriminative validity was examined by checking its ability to differentiate between regular and occasional users and patterns of krathom use and its concurrent validity by comparing its levels of score with the Fagerstrom Test for Nicotine Dependence (FTND). The KDS contains 16 items on a 0–3 (never–always) rating scale, making a total score of 0–48.
Results
Phase I EFA revealed a single-factor solution for the scale, which was confirmed by the CFA in Phase II, with an alpha coefficient of .98. The KDS discriminates regular from occasional users reasonably well and is highly correlated with the FTND score. Two cutoffs were suggested: 34/35 for distinguishing moderate from high dependence and 13/14 for low from moderate.
Conclusions
The KDS appears to capture key theoretical constructs and correlates with indices of drug dependence by standard criteria. It should be useful in early intervention for those with krathom use disorders in community and primary care settings.
Introduction
Krathom (Mitragyna speciosa Korth.) is a tropical tree that grows naturally in Malaysia and southern Thailand. Although krathom use is illegal in Thailand, its leaves have been traditionally chewed by the natives of Thailand, especially in the south. 1 The typical users are agriculturists and manual workers in rural villages, who chew fresh krathom leaves several times daily in the belief that this increases their work capacity. 2 , 3 At present, it is a popular agent for obtaining legal highs in Europe, and it is available for purchase online. 4 Moreover, krathom has been used as a substitute for opium and is reportedly effective in opioid withdrawal treatment. 5 , 6 It is also used as a traditional medicine for treatment of common and chronic diseases such as diarrhea, cough, toothache, and diabetes.1
Over 25 alkaloids have been isolated from krathom leaves, with mitragynine being dominant. 7 Mitragynine has an antinociceptive action through the supraspinal opioid receptors and descending noradrenergic and serotonergic systems. 8 Its alkaloid not only is an analgesic 9 but also has an inhibitory effect on electrically stimulated contraction of the isolated guinea-pig ileum. 10 It also has a direct effect on skeletal muscle by decreasing muscle twitches and has greater effect at the neuromuscular junction than on skeletal muscle or somatic nerve. 11 Chronic administration of mitragynine can alter and impair cognitive behavioral function in mice. 12 Mitragynine has been reported to account for 50% of methanol extract of krathom leaves (20 leaves contain about 17 mg of mitragynine). When high-dose mitragynine is used, its effects are opium-like. At low doses, it has stimulant-like effects similar to the coca plant.13
The first study on the health effect of krathom use reported psychotic symptoms, with “a hepatic disease–like face,” clouding of consciousness, behavioral disturbance, dizziness, and headache. 14 This study could not differentiate whether these were the effects of pure krathom use or the co-use of krathom with other substances. Other studies reported that long-term or heavy use of krathom did not cause paranoid disorders, and the users remained in good health, being mentally and physically “normal.” 13 , 15 Long-term users were found to be thin and have increased skin pigmentation. Furthermore, it was reported that if users did not spit out the leaf fiber after chewing, they may suffer gut obstruction or a stomach mass of accumulated krathom fiber/phytobezoar. 3 Recently, there have been reports of adverse health effects, including seizure and coma 16 and toxicity death, which were attributed mainly to krathom. 17 - 19
Regular krathom users reported suffering unpleasant symptoms upon cessation and being dependent on it. The dependence syndrome of krathom appears to be typical of other psychoactive substance dependence, including a strong desire to use krathom, preoccupation, impaired control, tolerance, withdrawal, and continued use despite knowing its harmful effects. Its withdrawal symptoms are reported to be very disturbing, including severe craving, muscle and bone pains, fatigue, insomnia, anxiety, depression, restlessness, irritability, chills, watery eyes, and runny nose, making users unable to stop using krathom. 2 , 6 , 20 , 21 The alkaloids in its leaves, producing opioid-like analgesic, adrenergic, muscle relaxant, and vasodilating effects, could explain these phenomena.22
Despite the prevalence of krathom use, little empirical research has been done to develop psychometrically sound measures specific to krathom use disorders. Such an instrument could provide clinically useful assessment information and might help primary care workers identify krathom-dependent users at an early stage and offer appropriate intervention for those with the problem.
This study was thus initiated to develop a Krathom Dependence Scale (KDS) and to explore its factor structure, reliability, and validity. The scale was designed to be useful as a screen for krathom dependence and as a severity rating that could be used for treatment planning. The study was divided into 2 phases. The goal of the first phase was to develop the scale and examine its factor structure using exploratory factor analysis (EFA), and the aim of the second phase was to evaluate the scale's construct validity using confirmatory factor analysis (CFA) and its discriminative and concurrent validity. EFA is an authentic discovery procedure; it enables one to see relationships among variables that are not at all obvious in the original data or even in the correlations among variables. CFA is used to test whether relationships expected on theoretical grounds actually appear in the data.23
Methods in Phase I Study
Study Settings
A cross-sectional data collection was undertaken in 10 villages of Nakhon Sri Thammarat province, southern Thailand, where krathom use is common and traditional. These areas are a center for the production of rubber and palm oil and the cultivation of other tropical crops. Some words are different from the official language, such as the words for twitching, feeling uncomfortable, and restlessness. Other words are similar to those generally used but differ in tone. During the interview with the respondents, some words of the local dialect were used.
Subjects
In each village, a systematic sampling with probability proportional to size was employed to select male villagers aged over 25 years from the list of households and residents of the village (village registry). As females do not generally use krathom, the study sample was limited to male users. Altogether, 529 males, including regular, occasional, ex-, and nonusers of krathom, were recruited between January and February 2011. Native dialect is spoken by almost 100% of the villagers, and communications require the use of local words.
A regular user was defined as an individual who had been using krathom 3 or more times per week for a period of at least 3 months. An occasional user referred to an individual who used krathom less frequently than 3 times per week or one who used it at certain times for a specific purpose (e.g., for a medicinal purpose or in social situations). A nonuser was defined as an individual who had never used krathom in his entire life. Ex-user was an individual who used to chew krathom in the past but had not used it within the previous 3 months.
Individuals with major psychiatric or physical illness, cognitive impairment, or an impaired sensorium and those who co-used krathom with other psychoactive substances, which could diminish the quality of the collected data, were excluded from the study. Six subjects were excluded: one co-used krathom with krathom cocktail and cannabis, and another co-used with heroin. Three were alcoholics. The last one was schizophrenic with a history of inhalant addiction. Altogether, 523 completed the instrument, including 114 regular users, 82 occasional users, 19 ex-users, and 308 nonusers. It is suggested that the sample size needed for the EFA approximately equals 5–10 times the number of questionnaire items. 24 Initially, KDS contained 42 items, so the sample size was considered more than adequate.
Study Instrument
To prepare the initial draft of the KDS, we reviewed the international diagnostic criteria and guidelines for psychoactive substance dependence, including the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, 25 and the International Classification of Diseases 10th revision (ICD-10) Classification of Mental and Behavioural Disorders, 26 and papers related to screening and diagnostic instruments for other psychoactive substances (e.g., Humeniuk et al., 27 Kavanagh et al., 28 Raistrick et al., 29 Legleye et al., 30 Meneses-Gaya et al., 31 etc.). Then, in-depth interviews were performed with 34 krathom traditional users and nonusers to elicit information on their patterns and reasons of krathom use, perceived benefits and risks, and characteristics of krathom dependence and withdrawal states. Statements were obtained from regular krathom users regarding how they felt dependent on krathom, their use behavior, and how they felt when they stopped using krathom (e.g., a strong desire and thinking of krathom all of the time, with its being the first thought after getting up; having to use krathom first thing in the morning; rarely going out of the village and almost never spending a night elsewhere because of being unable to live without krathom and because of withdrawal symptoms, i.e., chills, general malaise like catching a cold, sleepiness, yawning, craving, having no power to work or to do anything, or feeling as if something was missing in their lives). 2 An initial list of 41 items of krathom dependence symptoms and signs was derived by pooling these reports and by using diagnostic criteria and items of other instruments.
The first drafted questionnaire, comprising questions on demographic characteristics, patterns of krathom use, and the list of krathom dependence symptoms and signs, was tested on a convenience sample of 20 krathom users and nonusers in another subdistrict in the same district as the study villages, where the villagers speak the same dialect and are engaged in similar occupations. The list was then modified, splitting 1 item with 2 meanings into 2 separate items, thereby creating a questionnaire with 42 items. Each item was rated on a Likert scale of 0–3: never, sometimes, often, and almost always/always.
Data Analysis
In Phase I, the descriptive analyses and the exploratory factor analysis of the KDS were performed using R software epicalc, R-psych, and nFactors packages. 32 , 33 Maximum likelihood with varimax rotation and, subsequently, with oblique rotation was used for factor extraction because the data were relatively normally distributed. The oblique rotation method allows for the computation of a wide range of indices of goodness of fit of the model and permits statistical significance testing of factor loadings and of correlations among factors and the computation of confidence intervals for these parameters. 34 The number of factors was retained based on the eigenvalue being greater than 1 and also on heuristic and practical grounds. 35 Internal consistency was evaluated using Cronbach's alpha coefficient.
Results of Phase I Study
Demographic Characteristics
Demographic Characteristics
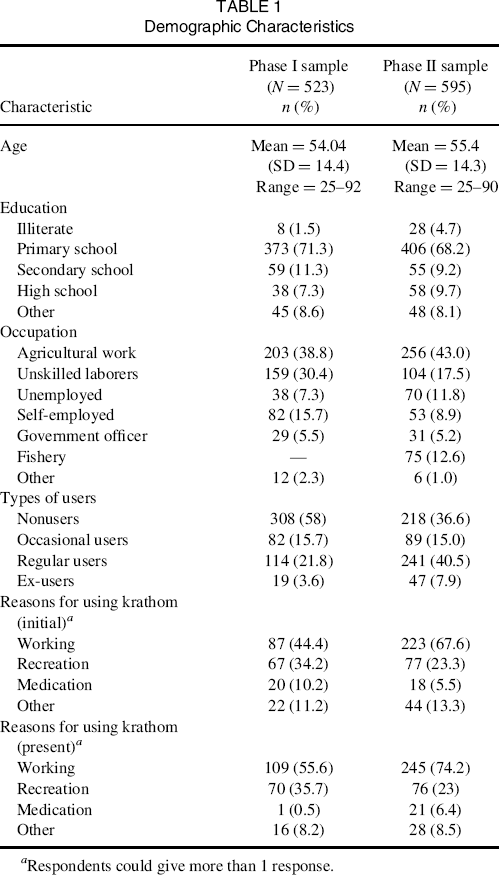
Respondents could give more than 1 response.
Factor Structure of the KDS
Krathom Dependence Scale: Factor Structure a
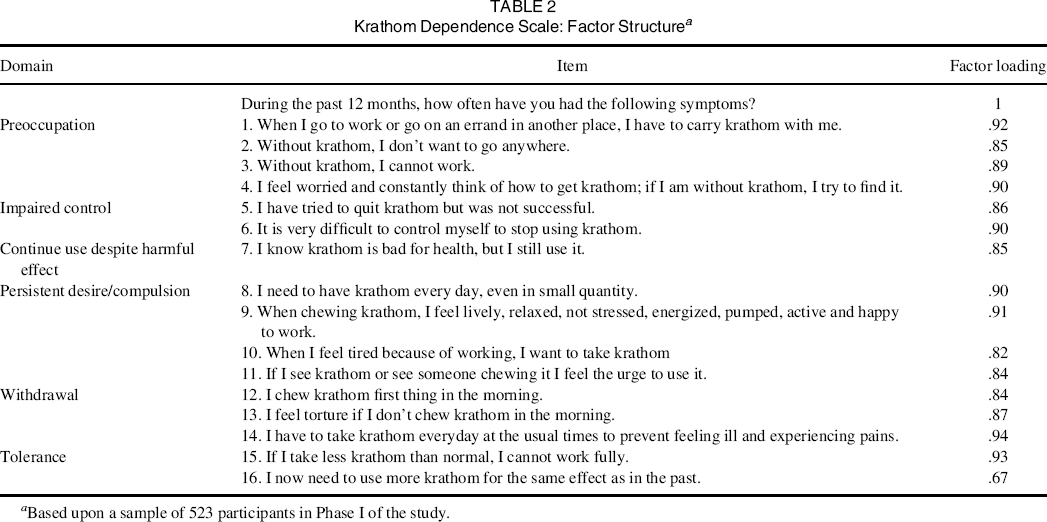
Based upon a sample of 523 participants in Phase I of the study.
The items with similar meaning were modified and collapsed together, yielding 16 items of KDS, with a Cronbach's alpha coefficient of .98. The KDS captures key theoretical constructs of the substance dependence in the International Classification of Diseases, 10th revision (ICD-10). 37 It consists of: preoccupation with use (items 1–4), impaired control over use (items 5 and 6), continued use despite harmful effect (item 7), persistent desire/compulsion to use (items 8–11), withdrawal (items 12–14), and tolerance (items 15 and 16).
Methods in Phase Ii Study
Study Settings and Subjects
Phase II of the study was conducted in 29 villages of the same province as in Phase I. Altogether, 653 male villagers aged over 25 years who were regular, occasional, or nonusers were randomly selected from the village registries between January and March 2012. Fifty-eight subjects were excluded and 31 refused to participate, leaving 595 for statistical analysis. The excluded participants included 54 alcoholics, 1 heroin user, 1 amphetamine user, 1 amphetamine and cannabis user, and 1 psychiatric patient. As the sample size needed for CFA approximately equals 15–20 times the number of questionnaire items 24 and the KDS contains 16 items, the required sample size was calculated to be at least 320 (16 × 20).
Study Instruments
The refined KDS and its factor structure from the first phase were reviewed by 3 experts in substance studies for content and construct validity as well as to receive feedback on the comprehensibility, flow, and language used in the scale. Item selection and refinement was done again after the review by the experts. Items that were somewhat ambiguous or otherwise difficult to understand were revised using simpler language. The KDS was then pilot tested with a convenience sample of 20 krathom users in another area outside the study site. The results of the pilot test for understandability of the items showed that the respondents required a total of approximately 5–7 minutes for completing the questionnaire. Again, ambiguous and difficult to understand items were further simplified. Each of the 16 items was rated on a Likert scale of 0–3; 0 = Never (the subject has never used krathom, or he has used krathom but he never had the symptom); 1 = Sometimes (the subject has used krathom and he sometimes has this symptom); 2 = Often (the subject has used krathom and he often has this symptom); 3 = Always (the subject has used krathom and he regularly has this symptom). None of the items needed to be reversed before analysis.
As there was no existing standard for krathom dependence, the Fagerstrom Test for Nicotine Dependence (FTND), modified to replace nicotine with krathom, was used to examine its correlation with the KDS. The FTND is a 6-item instrument, measuring the severity of dependence on nicotine. 38 The FTND was selected as a comparator because the pattern of krathom use among regular users was similar to that of nicotine, where users need to use it every day and many times a day, with some chewing krathom leaves continuously in a manner similar to that of a chain smoker. Regular users reported using krathom first thing after awakening and that using krathom did not interfere with their work or daily activities, which is also similar to tobacco use. Additionally, both instruments were designed to be used as screens for substance dependence and to provide ordinal measures of the severity of substance dependence in both clinical and nonclinical settings where the substance use was prevalent.39
Data Collection Procedure
After demographic and pattern of use questions were asked by the researcher, the KDS was either self-completed by the respondent or interviewed by D.S. Then, the respondent was asked to self-complete the FTND or was interviewed by the research assistant, who did not know the results of the KDS beforehand.
Ethics Statement
Institutional ethical approval was obtained from the Faculty of Medicine, Prince of Songkla University. In each phase of data collection, the village health volunteers helped the researcher to identify the subjects. When an individual was judged to meet the eligibility criteria, he was informed of the purpose of the study and the confidentiality and anonymity of the data. Verbal consent was obtained before the interview and written consent given during or after the interview. This is an acceptable practice in a field study in Thailand where villagers are reluctant to sign a document before they are sure of the information they are giving. Each respondent was given a small gift (a handkerchief or a small can of balm) upon the completion of the interview. The interview was done in private at the respondent's house or workplace (e.g., rubber or palm plantation, rice field, orchard).
Data Analysis
Confirmatory factor analysis (CFA) was conducted in order to determine whether data were consistent with the specified model suggested by the EFA, using LISREL version 8.80. 23 Maximum likelihood and goodness-of-fit tests for the specified model were performed.
In order to see how well the KDS scores could differentiate between occasional and regular users (discriminative validity), the scores were divided into 7 equal levels (0–6, 7–13, 14–20, 21–27, 28–34, 35–41, and 42–48) and plotted against the user groups. Test of differences of the scores between groups of users was done using chi-square. Lastly, patterns of krathom use (duration, quantity, and frequency of use) were compared among krathom dependence groups with high, medium, and low score levels using Kruskal-Wallis test.
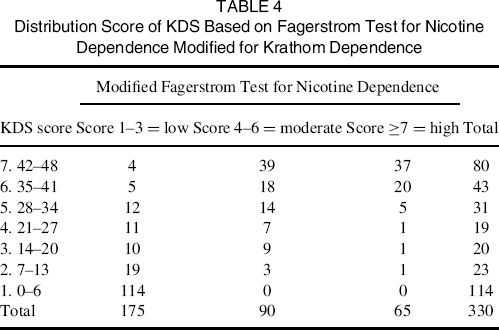
The concurrent validity of the KDS was analyzed by comparing its score levels with the modified FTND (with krathom replacing nicotine). This was done first by comparing the distributions of the KDS and the modified FTND and, subsequently, by examining the concordance between levels of the KDS scores and the recommended dependency levels of the modified FTND.
Results of Phase Ii Study
Demographic Characteristics
Demographic characteristics and patterns of krathom use of the respondents in Phases II were similar to those of respondents in Phase I (see Table 1).
Construct Validity of KDS
The 16 items with single-factor model obtained from Phase I were submitted to confirmatory factor analysis using the sample of Phase II. The goodness-of-fit statistics were as follows: chi-square = 479.12, df = 104, p < .001; root mean square error of approximation (RMSEA) = .11 (90% confidence interval [CI] = .09–.11); standardized root mean square residual (SRMR) = .04; comparative fit index (CFI) = .98; non-normed fit index (NNFI) = .98. These indices show that this model fitted the data reasonably well. The single-factor solution of the KDS was also confirmed.
The Cronbach's alpha coefficient was .97, indicating a high internal consistency of the scale.
Discriminative Validity of the KDS
Figure 1 shows proportions of regular and occasional users in each of the 7 levels of the KDS score. Regular users were significantly more likely to fall into the higher score levels of the KDS, compared with occasional users (p < .001). Although almost 90% of the occasional users scored 13 or less, 24.5% of the regular users did so. Furthermore, 50% of the regular users had scores of 35 or above, compared with 2.2% of the occasional users. Based on these score levels, 2 cutoffs are suggested for distinguishing between subjects with a high, moderate, and low probability of dependence on krathom: 34/35 for differentiating between medium and high scorers and 13/14 for low versus medium probability of dependence.
Proportion of regular and occasional users in each of the 7 levels of KDS score. Error bar = 95% confidence interval.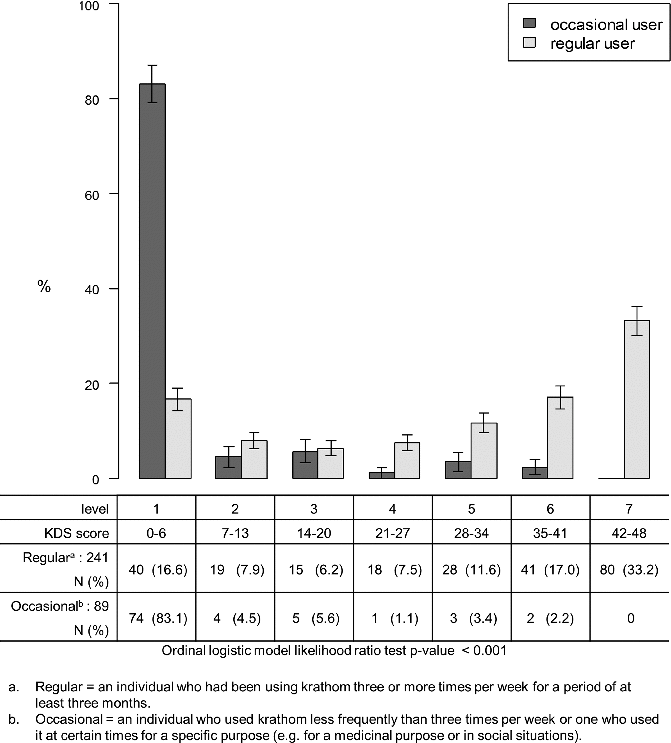
Correspondence between KDS Score and Parameters of Krathom Use Among Krathom Users (N = 330)
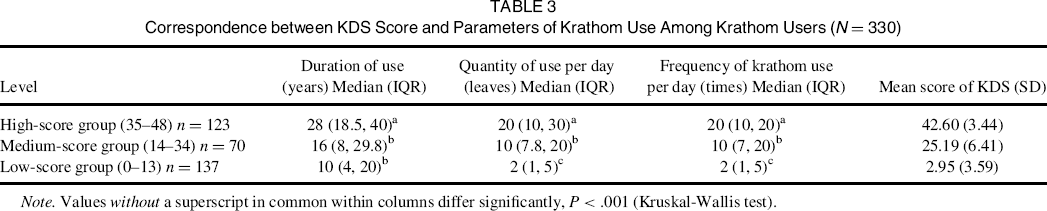
Note. Values without a superscript in common within columns differ significantly, P < .001 (Kruskal-Wallis test).
Correlation of the KDS with Modified FTND
Distribution Score of KDS Based on Fagerstrom Test for Nicotine Dependence Modified for Krathom Dependence
Discussion
The results of this study indicate that the KDS is a valid screen for krathom dependence and severity rating, with substantial discriminative and concurrent validity. Its construct validity based on the confirmatory factor analysis results supports the 1-factor model identified in the exploratory factor analysis. There was no poor-fitting item on the 16-item scale and the internal consistency of the scale was high. The single-factor structure was consistent with other measures of substance dependence. 28 , 29
Our respondents were middle-aged, and had been using krathom with widely varying frequency and quantity. This sample is, thus, a good representation of krathom users commonly seen in clinical and community settings. As aforementioned, research on krathom use is scarce, and there has not previously been any instrument for measuring krathom dependence. The KDS is the first measure developed for this purpose, making it impossible to compare its psychometric properties with those of other instruments. However, because the KDS was initially developed based upon our in-depth interviews with the actual krathom users, the items appear to be good measures of symptoms and signs of krathom use disorders. The KDS items captured all characteristic symptoms and signs of krathom dependence obtained from our in-depth interviews with the users, including having to chew krathom every day; difficulty to stopping or cutting down krathom use; having to chew krathom at the same time each day to avoid feeling sleepy and having muscle pain; having a slower work pace if chewing it less than normal; not wanting to go anywhere without krathom; and continuing to use krathom despite knowing its adverse health effects.2
Since no true gold standard for krathom dependence exists, absolute validity could not be assessed. However, good collateral validity was established through the high correlation of dependence with the pattern of krathom use. Based upon the comparison with the frequency, quantity, and duration of krathom use, the KDS could satisfactorily distinguish between subjects with a moderate to high probability of dependence from those with a low probability and had moderate ability to distinguish between moderate and high probabilities of dependence. Thus, the KDS could be a useful means of screening for dependence in communities with a high prevalence of krathom users or in the primary health care setting. Moreover, as the test can be administered either by self-completion or via interview and takes no more than 10–15 minutes, it is an easy instrument to use in practice.
Forty regular users had scores of 0–6, although they used krathom every day. Among these, 30 used less than 5 leaves per day. These users had been using it for a period ranging from 1 to 50 years. During the interview, these regular users reported that they used krathom on a regular schedule every day and never stopped using it because it was always available for them, as they grew krathom trees at home. Therefore, they never or rarely experienced the state of being “without krathom” and had only minimal symptoms of krathom dependence.
KDS was also highly correlated with the modified FTND. Krathom use patterns are similar to those of tobacco smoking. Neither substance interferes with the users’ function or daily activities but, in contrast, may be perceived as enhancing users’ capacity for work. The feeling of dependence, however, is strong, making users feel the need to use these substances almost all of the time. The tolerance pattern for each substance is also similar. We found that the behavior of the highly dependent subjects in our study was quite similar to that of chainsmokers, i.e., they needed to chew krathom leaves repeatedly to maintain the effect of krathom on their body. This could explain why the KDS scores were quite comparable with those of the modified FTND.
This study has some limitations. Although krathom use is common in this area, and the participants were willing to respond to all questions, it was almost impossible to obtain an accurate measure of krathom use. Also, there were problems of co-use with other substances. We found, in Phase I, that 36% of regular users and 46% of occasional users had used alcohol in the last 12 months, although not to the level of alcoholism. Moreover, most krathom users drank more coffee and tea and used more tobacco than people who did not use krathom.
It is important to point out that this study is limited to those who use krathom by chewing its fresh leaves, as all subjects used it in this way. This differs from users in other countries such as European countries and Malaysia, where approximately 90% of users use it in the form of a drink, by smoking, or by adding its leaves to food. 21 Furthermore, this study was undertaken in a community with high prevalence and traditional pattern of krathom use. The prevalence of krathom use in other communities may not be as high as that reported here. This point should be carefully considered when using these instruments in a different setting.
Our findings provide evidence that krathom is addictive, with characteristic symptoms and signs of dependence. Although krathom differs from other substances in the purpose of use, our findings on krathom dependence were relevant to the general term of dependence, which is the state of needing or depending on a substance for support or to function or survive. Applied to krathom, dependence implies the need for repeated doses to feel good or to avoid suffering.40
Overall, our results indicate that the KDS has a well-defined structure and successfully captures the key theoretical framework of substance dependence. It has potential to be used as a screen for krathom dependence in primary care settings with a high prevalence of krathom use and as a severity rating for treatment planning and prognostic judgments. The brevity and ease of scoring the KDS make it an efficient way to obtain clinically meaningful information. The KDS could also be incorporated into general health and lifestyle screening questionnaires in clinical and nonclinical settings.
Footnotes
Acknowledgments
The authors wish to thank village health volunteers who acted as assistant researchers, the Director of the Mae Chao Yu Hua Health Center, and all staff for help in coordinating the fieldwork. Ms. Walailuk Jitpiboon's help with the data processing and analysis was highly appreciated.
Author Contributions
S. Assanangkornchai, A. Geater, and D. Saingam each participated in designing the study. D. Saingam collected data. A. Geater, S. Lerkiatbundit and D. Saingam conducted the statistical analyses. All authors contributed to the writing of the manuscript.